
Abstract
Association of angiotensin II type-1 receptor (AT1R) A1166C gene polymorphism with the susceptibility of immunoglobulin A nephropathy (IgAN) is still controversial. This meta-analysis was conducted to evaluate the association of AT1R A1166C gene polymorphism with IgAN susceptibility. The search was performed in the databases of PubMed, Embase, and Cochrane Library as of 1 May 2014. The eligible investigations were recruited for this meta-analysis. Four literatures on the association between AT1R A1166C gene polymorphism and IgAN susceptibility were identified for this meta-analysis. Interestingly, all the included studies were from Asian population. There was no association between AT1R A1166C gene polymorphism and IgAN susceptibility for overall populations (C allele vs. A allele: OR = 1.04, 95% CI: 0.78–1.39, p = 0.76; CC vs. AC + AA: OR = 1.20, 95% CI: 0.48–2.98, p = 0.70; AA vs. AC + CC: OR = 0.97, 95% CI: 0.70–1.34, p = 0.85), and in Asians. In conclusion, AT1R A1166C gene polymorphism was not associated with IgAN susceptibility in Asian population. However, more case-control association investigations on larger, stratified populations are required in the future.
Introduction
Immunoglobulin A nephropathy (IgAN) is one of the most common varieties of primary glomerulonephritis, and IgAN is characterized by excessive glomerular deposition of IgA1, C3, and C5b-9, which may lead to renal failure.Citation1,Citation2 IgAN represents the leading cause of kidney failure among East Asian populations and the most frequent form of primary glomerulonephritis among Europeans, and recent studies define IgAN as an autoimmune trait of complex architecture with a strong genetic determination.Citation3 Some current evidencesCitation4–7 indicated that genetic factors might play a key role in the onset of IgAN, and might be associated with the IgAN risk.
The angiotensin II receptor includes two subtypes: angiotensin II type 1 receptor (AT1R) and angiotensin II type 2 receptor.Citation8,Citation9 The angiotensin II type 1 receptor (AT1R) is the primary pathogenic effector for angiotensin II, and it is a member of the G-protein-coupled receptor superfamily expressed in most tissues, where receptor activation leads to vasoconstriction, water retention, and vascular smooth muscle cell proliferation and hypertrophy.Citation9,Citation10 AT1R A1166C gene polymorphism is an important mutation of AT1R. It might be implicated in the etiology of IgAN risk and had been investigated in numerous epidemiologic studies. There was no other meta-analysis to study the association of the AT1R A1166C gene polymorphism with IgAN risk. This meta-analysis was performed to assess the relationship between AT1R A1166C gene polymorphism and IgAN susceptibility.
Materials and methods
Search strategy
Search strategy for the association of AT1R A1166C gene polymorphism with IgAN risk
The relevant studies were searched from the electronic databases of PubMed, Embase, and Cochrane Library on 1 May 2014. The retrieval strategy of “(angiotensin II type-1 receptor OR AT1R) AND (immunoglobulin A nephropathy OR IgAN)” was entered into those databases mentioned above for search. Additional articles were identified through references cited in the retrieved articles.
Inclusion criteria: (1) A case-control study; (2) The outcome had to be IgAN; (3) There had to be at least two comparison groups (IgAN group vs. control group).
Exclusion criteria: (1) Review articles, editorials, and case reports; (2) Articles did not provide the detail genotype data; (3) Investigating the association of other genes with IgAN; (4) Investigating the role of drugs in diseases; (5) Multiple publications of the same data from the same study group.
Data extraction and synthesis
The following information was extracted from each study independently by at least two investigators: first author’s surname, year of publication, ethnicity of study population, and the number of cases and controls for A1166C genotype. Frequencies of C allele for the case group and the control group were calculated, from the corresponding genotype distribution. The results were compared and disagreements were resolved by discussion.
Statistical analysis
Available data were entered into Cochrane Review Manager (RevMan, Version 5, Oxford, UK) and analyzed. The pooled statistic was counted using the fixed effects model, but a random effects model was conducted when the p value of heterogeneity test was less than 0.1.Citation11–13 Results were expressed with odds ratios (OR) for dichotomous data, and 95% confidence intervals (CI) were also calculated. p < 0.05 was required for the overall OR to be deemed statistically significant.Citation14–16 I2 was used to test the heterogeneity between the included studies.
Results
Study characteristics
According to the inclusion and exclusion criteria, four articlesCitation17–20 were identified for the analysis of the association between AT1R A1166C gene polymorphism and IgAN susceptibility in our meta-analysis. All the included studies were conducted in Asians. These 19 studies contained 511 case series and 413 controls ().
Table 1. Characteristics of the studies evaluating the effects of AT1R A1166C gene polymorphism on IgAN risk.
Association of AT1R A1166C gene polymorphism with IgAN risk
In this meta-analysis, there was no significant association between AT1R A1166C gene polymorphism and IgAN risk in overall populations (C allele vs. A allele: OR = 1.04, 95% CI: 0.78–1.39, p = 0.76; CC vs. AC + AA: OR = 1.20, 95% CI: 0.48–2.98, p = 0.70; AA vs. AC + CC: OR = 0.97, 95% CI: 0.70–1.34, p = 0.85; for C allele, for CC genotype, for AA genotype; ).
Figure 1. Association between AT1R A1166C gene polymorphism and IgAN risk. (A) C versus A; (B) CC versus AA + AC; (C) AA versus AC + CC.
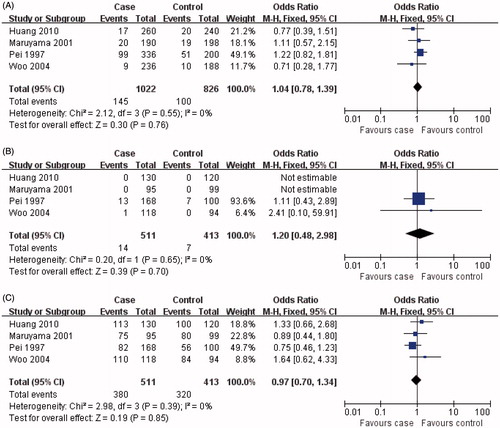
Table 2. Meta analysis of the association of AT1R A1166C gene polymorphism with risk of IgAN.
Interestingly, all the recruited studies were from Asian population, and the results of the relationship between AT1R A1166C gene polymorphism and IgAN risk in Asians were the same as those from overall populations ().
Discussion
Increasing evidence indicates that the AT1R A1166C gene polymorphism has well-documented participation in the pathogenesis of some renal diseases, and genetic markers might offer some benefit to better predict the risk of renal diseases. IgAN is one of the most common renal diseases. Data on the risk factors for the pathogenesis of IgAN were insufficient. There was rare genetic molecular marker to predict the onset of IgAN. This meta-analysis was performed to assess whether the AT1R A1166C gene polymorphism could predict the susceptibility of IgAN.
In this investigation, we found that AT1R A1166C gene polymorphism was not associated with the susceptibility of IgAN in overall populations. Interestingly, all the included studies were from Asian population. The results for Asian population were the same as those in overall populations. There were no any included studies from Caucasians. The role of AT1R A1166C gene polymorphism in the susceptibility of IgAN should be assessed in the future.
In the past years, there was no any meta-analysis to assess the association of AT1R A1166C gene polymorphism with the susceptibility of IgAN disease. In our investigation, we found that there was no association between AT1R A1166C gene polymorphism and IgAN susceptibility in overall population, and in Asians. However, these findings should be regarded cautiously because many other ingredients, such as heterogeneity of enrolled cases, limited statistical power, variable study designs and different interventions, were closely related to affect the results. Furthermore, whether the AT1R A1166C polymorphism is just linked with other discrete loci involved in the occurrence of IgAN is not clear at the moment.
In conclusion, AT1R A1166C gene polymorphism was not associated with IgAN susceptibility in Asian population. However, more case-control association investigations on larger, stratified populations are required to further clarify the role of the AT1R A1166C gene polymorphism in IgAN susceptibility in different ethnicities.
Declaration of interest
The authors declare no competing interests.
This study was supported by the sub-item of 985 Project Foundation of Sun Yat-Sen (The Hundred Talents Program Foundation; No. 88000-3311300).
References
- Qin YH, Zhou TB, Su LN, et al. Association between ACE polymorphism and risk of IgA nephropathy: A meta-analysis. J Renin Angiotensin Aldosterone Syst. 2011;12:215–223
- Rosenblad T, Rebetz J, Johansson M, et al. Eculizumab treatment for rescue of renal function in IgA nephropathy. Pediatr Nephrol. 2014;29:2225–2228
- Kiryluk K, Novak J. The genetics and immunobiology of IgA nephropathy. J Clin Invest. 2014;124:2325–2332
- Ko GJ, Lee EA, Jeon US, et al. The association of Klotho polymorphism with disease progression and mortality in IgA nephropathy. Kidney Blood Press Res. 2012;36:191–199
- Wang W, Sun Y, Fu Y, et al. Interaction of C1GALT1-IL5RA on the susceptibility to IgA nephropathy in Southern Han Chinese. J Hum Genet. 2013;58:40–46
- Zhou TB, Yin SS, Liang R. A meta-analysis of the association between angiotensin-converting enzyme insertion/deletion gene polymorphism and end-stage renal disease risk in IgA nephropathy patients. J Renin Angiotensin Aldosterone Syst. 2013;14:235–241
- Zhou XJ, Cheng FJ, Qi YY, et al. FCGR2B and FCRLB gene polymorphisms associated with IgA nephropathy. PLoS One. 2013;8:e61208
- Miura S, Karnik SS, Saku K. Review: Angiotensin II type 1 receptor blockers: Class effects versus molecular effects. J Renin Angiotensin Aldosterone Syst. 2011;12:1–7
- Zhou TB, Yin SS, Jiang ZP. Association of angiotensin II type-1 receptor A1166C gene polymorphism with the susceptibility of end-stage renal disease. J Recept Signal Transduct Res. 2013;33:325–331
- Wang JL, Li X, Hao PP, et al. Angiotensin II type 1 receptor gene A1166C polymorphism and essential hypertension in Chinese: A meta-analysis. J Renin Angiotensin Aldosterone Syst. 2010;11:127–135
- Zhou TB, Guo XF, Yin SS. Association of peroxisome proliferator-activated receptor gamma Pro12Ala gene polymorphism with type 2 diabetic nephropathy risk in Caucasian population. J Recept Signal Transduct Res. 2014;34:180–184
- Zhou TB, Guo XF, Yin SS. Association of T869, C509T, G915C gene polymorphism of transforming growth factor-beta1 with IgA nephropathy risk. Ren Fail. 2014;36:823–828
- Zhou TB, Jiang ZP, Qin YH, et al. Association of transforming growth factor-beta1 T869C gene polymorphism with diabetic nephropathy risk. Nephrology (Carlton). 2014;19:107–115
- Zhou TB, Drummen GP, Jiang ZP, et al. GSTT1 Polymorphism and the risk of developing prostate cancer. Am J Epidemiol. 2014;180:1–10
- Zhou TB, Jiang ZP. Association between plasminogen activator inhibitor-1 4G/5G gene polymorphism and immunoglobulin A nephropathy susceptibility. J Recept Signal Transduct Res. 2014; [Epub ahead of print]
- Zhou TB, Jiang ZP, Huang MF. Association of vitamin D receptor BsmI (rs1544410) gene polymorphism with the chronic kidney disease susceptibility. J Recept Signal Transduct Res. 2014; [Epub ahead of print]
- Pei Y, Scholey J, Thai K, et al. Association of angiotensinogen gene T235 variant with progression of immunoglobin A nephropathy in Caucasian patients. J Clin Invest. 1997;100(4):814–820
- Maruyama K, Yoshida M, Nishio H, et al. Polymorphisms of renin-angiotensin system genes in childhood IgA nephropathy. Pediatr Nephrol. 2001;16:350–355
- Woo KT, Lau YK, Choong LH, et al. Polymorphism of renin-angiotensin system genes in IgA nephropathy. Nephrology (Carlton). 2004;9:304–309
- Huang HD, Lin FJ, Li XJ, et al. Genetic polymorphisms of the renin-angiotensin-aldosterone system in Chinese patients with end-stage renal disease secondary to IgA nephropathy. Chin Med J (Engl). 2010;123:3238–3242