
Abstract
Introduction: Hepcidin, a small peptide hormone synthesized in the liver, plays central role in regulation of iron metabolism. Hepcidin generation in chronic kidney disease (CKD) is dependent on iron status, anemia, inflammation, and hypoxia and erythropoietin levels. In our study, the relationship between Prohepcidin levels and inflammation and iron indices in non-diabetic uremic patients was investigated. Methods: This study has a cross-sectional design which includes four groups: Non-diabetic 21 patients with stage 4 CKD (predialysis), 20 hemodialysis (HD) and 21 peritoneal dialysis (PD) patients and 17 healthy volunteers as the control group. Complete blood count, iron, total iron binding capacity (TIBC), ferritin, high-sensitive C-reactive protein (hsCRP), fibrinogen, parathyroid hormone, interleukin (IL)-6 and Prohepcidin levels were recorded. Results: Serum Prohepcidin levels in the predialysis, HD, PD and the control groups were 119.6 ± 45.1 ng/mL, 140.2 ± 41.8 ng/mL, 148.2 ± 35.0 ng/mL and 93.8 ± 21.9 ng/mL, respectively (p < 0.001). Prohepcidin was positively correlated with urea (r = 0.345, p = 0.002), creatinine (r = 0.465, p < 0.001), phosphorus (r = 0.253, p = 0.025), hsCRP (r = 0.275, p = 0.019), duration of dialysis treatment (r = 0.443, p < 0.001), fibrinogen (r = 0.467, p < 0.001) and IL-6 (r = 0.615, p < 0.001) levels. A negative correlation was detected between Prohepcidin levels and albumin (r = −0.286, p < 0.001), TIBC (r = −0.573, p < 0.001), GFR (r = −0.473, p < 0.001), hemoglobin (r = −0.351, p = 0.002) and hematocrit (r = −0.342, p = 0.002) levels. Discussion: Prohepcidin levels increase with deepening anemia and show positive correlation with inflammatory markers. Therapeutic interventions regarding Prohepcidin action on inflammatory status may play a role in the treatment of anemia due to inflammation. Functional iron deficiency is frequent in uremic patients. It may be beneficial to measure Prohepcidin level together with ferritin among these patients.
Introduction
Renal anemia is one of the most important problems that affect quality of life in chronic kidney disease (CKD). Renal anemia is mainly related to erythropoietin (EPO) and iron deficiencies.Citation1 Hepcidin is synthesized in the liver; and is described as the homeostatic regulator of iron absorption from the gut, iron turnover in macrophages and iron release from hepatic stores. Hepcidin inhibits cellular iron release by way of binding to and stimulating the destruction of ferroportin. The synthesis of hepcidin is increased by iron load and decreased by presence of anemia and hypoxia.Citation2,Citation3 The measurement of the biologically active hepcidin-25 is difficult due to technical and financial reasons. Therefore, Prohepcidin which is easier to measure due to its higher immunogenicity, is more commonly used in clinical investigations. Prohepcidin levels have been found to be elevated and negatively correlated with glomerular filtration rate in uremic patients. There are studies in which Prohepcidin levels were correlated with iron indices and hematologic parameters while there are others failing to show this relationship.Citation4–6
The aim of our study was to evaluate the relation of Prohepcidin levels with iron parameters and inflammatory markers in non-diabetic uremic patients.
Methods
Patient groups
This is a cross-sectional study involving uremic patients followed in our clinic. The study was conducted with four groups of patients who gave written informed consent:
Group 1 (predialysis group)
Patients with stage-4 CKD (glomerular filtration rate between 15–29 mL/min measured at two different times within the last six months).
Group 2 [hemodialysis (HD) group]
Patients on chronic HD program thrice a week for more than three months who met the dialysis adequacy criteria proposed by international guidelines.
Group 3 [peritoneal dialysis (PD) group]
Patients on chronic PD program for more than three months who met the dialysis adequacy criteria proposed by international guidelines.
Group 4 (control group)
Age matched healthy individuals.
Exclusion criteria were the presence of diabetes mellitus, age under 18 or above 80 years, any active infection, bleeding episode, parenteral iron treatment or blood transfusion within the last one month, severe malnutrition, malignancy, acute or chronic liver disease, use of immunosuppressive medications, hemoglobin level below 8 g/dL, hemochromatosis, thalassemia or any other systemic disease related with anemia and dialysis duration less than three months.
The age, gender, body mass index (BMI), causes of primary kidney disease and duration of dialysis treatment were recorded. The levels of glucose, urea, creatinine, uric acid, cholesterol, triglyceride, total protein, albumin, leukocyte count, hemoglobin, hematocrit, iron, total iron binding capacity (TIBC), ferritin, high sensitive C-reactive protein (hsCRP), fibrinogen, interleukin-6 (IL-6) and Prohepcidin levels were studied and recorded.
Laboratory methods
Blood sample was obtained after 12 hours of fasting. Samples were taken just before the midweek session in HD group. Serum sample for the measurement of IL-6 and Prohepcidin were kept at −80 °C. Creatinine clearance was calculated by using CKD-EPI formula.
Biochemical and hematological parameters were studied by appropriate methods using Roche COBAS MIRA auto-analyzer (Basel, Switzerland) and ABX Pentra DX120 machine (Montpellier, France), respectively. Ferritin levels were measured by immunoassay method while hsCRP levels by turbidimetric method. IL-6 level was studied using EASIA Biosource kit (BioSource Europe, Nivelles, Belgium) by enzyme sensitive immunoassay method. For the measurement of Prohepcidin levels by enzyme linked immunosorbent assay (ELISA); DRG® Hepcidin Prohormon ELISA (EIA-4015) kit (Marburg, Germany) was used.
Statistical methods
Statistical analysis was conducted by using Statistical Package for Social Sciences (SPSS) for Windows ver. 16.0 package program (SPSS Inc., Chicago, IL). Numerical values were expressed as mean ± standard deviation (SD). For comparison of the groups; Student t-test or Mann–Whitney U test were used when necessary. For comparison of more than two groups; one-way ANOVA or Kruskal–Wallis test were used. Correlation analysis was conducted by using Pearson correlation test. Parameters found to be related with Prohepcidin levels were analyzed by multivariate analysis. p < 0.05 was regarded as statistically significant.
Results
Sixty-two patients and 17 healthy volunteers were included in the study. Causes of primary kidney diseases were hypertension (n = 13), chronic glomerulonephritis (n = 10), chronic pyelonephritis (n = 7), autosomal dominant polycystic kidney disease (n = 5), uropathologies (n = 4) and amyloidosis (n = 4); while it was unknown in 19 patients.
The demographic, clinical and laboratory data of the groups are presented in . The mean serum Prohepcidin levels in the predialysis, HD, PD and the control groups were 119.6 ± 45.1 ng/mL, 140.2 ± 41.8 ng/mL, 148.2 ± 35.0 ng/mL and 93.8 ± 21.9 ng/mL; respectively ( and ). Hematological and iron-related parameters are presented in .
Figure 1. The distribution of hepcidin levels of the groups. HD: hemodialysis, PD: peritoneal dialysis.
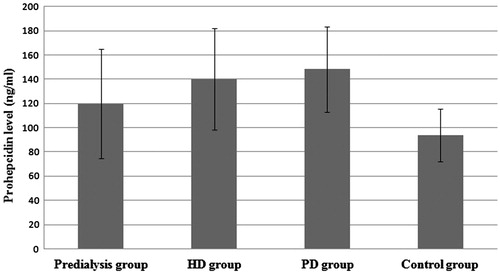
Table 1. The demographic and clinical data of the groups.
Table 2. Hematological and iron-related parameters.
Prohepcidin levels in each patient group were statistically significantly higher than the control group. Patients in the PD group had higher Prohepcidin level compared with those in predialysis group (p = 0.014). Uremic patients (predialysis + HD + PD groups) had higher Prohepcidin level than the control group (136.0 ± 42.0 ng/mL vs. 93.8 ± 21.9 ng/mL; p < 0.001). Prohepcidin levels were similar in patients using erythropoiesis stimulating agents or not (141.7 ± 45.4 ng/mL vs. 141.9 ± 42.40 ng/mL; p = 0.99).
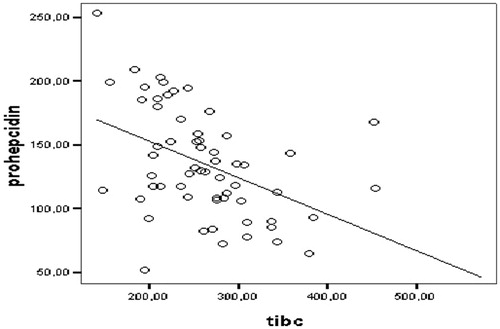
Prohepcidin was positively correlated with urea (r = 0.345, p = 0.002), creatinine (r = 0.465, p < 0.001), hsCRP (r = 0.275, p = 0.019), fibrinogen (r = 0.467, p < 0.001) and IL-6 (r = 0.615, p < 0.001) levels. Albumin (r = −0.286, p < 0.001), TIBC (r = −0.573, p < 0.001), creatinine clearance (r = −0.473, p < 0.001), hemoglobin (r = −0.351, p = 0.002) and hematocrit (r = −0.342, p = 0.002) levels were negatively correlated with Prohepcidin levels. A negative relationship of Prohepcidin with TIBC was detected with linear regression analysis ().
Figure 2. Relationship of prohepcidin with total iron binding capacity.
When correlation analysis was repeated dividing all patients into two groups (uremic patients and control group); Prohepcidin levels were correlated with creatinine clearance (r = −0.71, p < 0.001), IL-6 (r = 0.58, p = 0.018) in the control group; while TIBC (r = −0.44, p < 0.0001) was related with Prohepcidin levels. Linear regression analysis results revealed that creatinine clearance (B = −0.89, beta = −0.75 and p < 0.001) was effective on Prohepcidin levels in the control group; while only TIBC (B = −0.26, beta = 0.075 and p = 0.001) and the patient group (B = 12.1, beta = 0.23 and p = 0.043) were the parameters determining Prohepcidin in the uremic patients.
Discussion
In our study we detected that uremic patients had significantly higher Prohepcidin levels than the control group. Moreover, the negative correlation detected between Prohepcidin and creatinine clearance in the control group was consistent with the current literature.Citation4–6 This is probably due to renal clearance of Prohepcidin.Citation7 The only significant intergroup difference was between PD and predialysis groups.
Serum Prohepcidin level was found to be negatively correlated with hemoglobin, hematocrit and TIBC; and was positively correlated with hsCRP, IL-6 and fibrinogen levels. The strong correlation of Prohepcidin with iron parameters and inflammatory markers demonstrated that Prohepcidin reflects hepcidin activity accurately in both uremic and non-uremic population. Although TIBC levels of the groups were similar; ferritin levels were different; and there was no correlation between Prohepcidin levels and ferritin levels. This might have been related to medications given to the patients and the acute phase reactant nature of ferritin. So TIBC has been found in our study to be the determinant of Prohepcidin level, not ferritin. Studies with HD patients showed that intravenous iron treatment leads to increased serum hepcidin, Prohepcidin and urinary Prohepcidin levels.Citation8,Citation9 Therefore, patients receiving parenteral iron within the last month were excluded from the study. Besides, we excluded patients with active hemorrhage, deep anemia, use of immunosuppressive medications, parenteral iron treatment, and transfusion all of which may affect Prohepcidin levels. Besides, inclusion of these subjects also would affect the objectiveness of the study especially regarding comparison with the control group in which none of the patients had the mentioned factors.
Malyszko et al.Citation5 studied 33 CKD, 104 HD and 70 renal transplant patients and found that hepcidin and ferritin levels were high in all groups compared with the control group. Hepcidin was correlated with total protein, albumin, creatinine and GFR in CKD patients. Hepcidin levels in HD patients were correlated with triglyceride, albumin, urea, creatinine, residual renal functions and hsCRP. Moreover; hepcidin was found to be correlated with total protein, ferritin, post-transplantation duration, creatinine and GFR in patients with renal allografts. It was correlated with only triglyceride and ferritin in the control group. They concluded that elevated hepcidin level is associated with chronic low-grade inflammation and impaired renal function. We demonstrated a positive correlation between Prohepcidin and hsCRP, IL-6, fibrinogen and impaired renal function; and negative correlation with anemia of increasing severity.
Zaritsky et al.Citation10 compared 48 pediatric and 32 adult patient with stage 2–4 CKD; and 26 pediatric PD patients for hepcidin, iron parameters, inflammatory markers and renal function. Hepcidin levels were measured as 127.3 ng/mL, 269.9 ng/mL and 652.4 ng/mL. With multivariate analysis; hepcidin was correlated with ferritin in the first and second groups and with ferritin and transferrin saturation in the third group. Moreover; ferritin and CRP were found to be correlated with hepcidin in the PD group. It was commented that elevated hepcidin may be a new marker for iron status and erythropoietin resistance in CKD. Our findings of higher Prohepcidin level in uremic patients and correlation with creatinine clearance and TIBC are consistent with this study.
Chronic inflammation plays role in the pathogenesis of anemia related with CKD and chronic inflammatory diseases through various ways including disturbed iron metabolism causing increased hepcidin synthesis. Hence, interventions targeting hepcidin may be effective in the treatment of inflammation related anemia. Moreover; measurement of hepcidin together with iron indices may be helpful in the diagnosis and management of anemia seen in patients with CKD.Citation2,Citation9,Citation11 The role of hepcidin in anemia related with chronic kidney disease has been clearly defined in many studies.Citation12 Inflammation is an important factor in the development of anemia in these patients. Canavesi et al stated that hepcidin is upregulated by inflammation.Citation13 Similarly, we found in our study that hsCRP levels were higher in the dialysis groups and there was a positive correlation between hsCRP and prohepcidin levels.
Some studies reported correlation between hepcidin and ferritin.Citation9,Citation11 Both of these parameters increase in case of low grade inflammation as in CKD; and decrease in the presence of iron deficiency. There is need for further controlled studies for hepcidin levels to be mentioned in international guidelines as a more valuable marker than ferritin for determination of iron status of patients with CKD. In our study, we excluded patients with overt infectious or inflammatory diseases to omit the effect of these pathologies on ferritin which is an acute phase reactant also. But considering the study population, they may have subtle infections due to vascular access or other reasons; and also inflammation directly related to chronic kidney disease. This may be the reason of lack of correlation between Prohepcidin and ferritin levels. Meanwhile, the higher ferritin levels in HD group compared to the PD group may be related with more frequent use of parenteral iron in HD patients. It is clear that this finding was not related to the acute phase nature of ferritin regarding lower mean hsCRP levels in HD group, although statistically not significant.
Diabetes mellitus is a disease in which many systems are involved including inflammatory pathways as well as glucose and lipid metabolism. Besides, diabetes mellitus is associated with infectious complications. Therefore, inclusion of diabetic subjects in both the patient and control groups would lead to heterogeneity and would affect the results. So we excluded diabetic subjects.
Previous studies reported correlation between hepcidin and triglyceride levels. Xue et al.Citation14 found this correlation in patients with renal allografts. Samouilidou et al.Citation15 reported that hepcidin level is correlated with triglyceride levels in patients with end stage renal disease. Both Prohepcidin and triglyceride levels were higher in uremic patients (p = 0.004), but here was no statistically significant correlation between them.
Although; there are limited number of studies showing that serum hepcidin level is not valuable in the evaluation of response to treatment with erythropoiesis stimulating agents in HD patients;Citation9,Citation11 this needs to be studied further. Measurement of hepcidin levels would add to prediction of response to treatment of anemia with parenteral iron and erythropoiesis stimulating agents.Citation12
The major limitations of our study are its cross-sectional nature and small number of patients which prevent to make a cause-result relation. In addition, discrepancies between the groups regarding some parameters (hsCRP and BMI) may weaken the results of the study. The comparison of hepcidin with Prohepcidin in a wider and more homogenous population of patients may be more informative.
Conclusion
We detected that Prohepcidin level is elevated in uremic patients with CKD. Moreover; the strong correlation between Prohepcidin and inflammatory markers is striking indicating increased inflammation in the presence of anemia. Measurement of hepcidin level together with iron indices would be valuable in the diagnosis and treatment plans of CKD patients who have functional iron deficiency.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of this article.
References
- Kazmi WH, Kausz AT, Khan S, et al. Anemia: An early complication of chronic renal insufficiency. Am J Kidney Dis. 2001;38:803–812
- Ganz T. Hepcidin – a regulator of intestinal iron absorption and iron recycling by macrophages. Best Prac Res Clin Hematol. 2005;18(2):171–182
- Atanasiu V, Manolescu B, Stoian I. Hepcidin-central regulator of iron metabolism. Eur J Hematol. 2007;78:1–10
- Taes YE, Wuyts B, Boelaert JR, De Vriese AS, Delanghe JR. Prohepcidin accumulates in renal insufficiency. Clin Chem Lab Med. 2004;42:387–389
- Malyszko J, Malyszko JS, Pawlak K, Mysliwiec M. Hepcidin, iron status, and renal function in chronic renal failure, kidney transplantation, and hemodialysis. Am J Hematol. 2006;81:832–7
- Troutt JS, Butterfield AM, Konrad RJ. Hepcidin-25 concentrations are markedly increased in patients with chronic kidney disease and are inversely correlated with estimated glomerular filtration rates. J Clin Lab Anal. 2013;27:504–510
- Peters HP, Laarakkers CM, Pickkers P, et al. Tubular reabsorption and local production of urine hepcidin-25. BMC Nephrol. 2013;14:70
- Malyszko J, Malyszko JS, Mysliwiec M. Serum Prohepcidin and hepcidin in hemodialyzed patients undergoing iron therapy. Kidney Blood Press Res. 2009;32:235–238
- Nakanishi T, Kuragano T, Kaibe S, Nagasawa Y, Hasuike Y. Should we reconsider iron administration based on prevailing ferritin and hepcidin concentrations? Clin Exp Nephrol. 2012;16:819–826
- Zaritsky J, Young B, Wang HJ, et al. Hepcidin – a potential novel biomarker for iron status in chronic kidney disease. Clin J Am Soc Nephrol. 2009;4:1051–10516
- Kato A, Tsuji T, Luo J, Sakao Y, Yasuda H, Hishida A. Association of Prohepcidin and hepcidin-25 with erythropoietin response and ferritin in hemodialysis patients. Am J Nephrol. 2008;28:115–121
- Swinkels DW, Wetzels JF. Hepcidin: A new tool in the management of anaemia in patients with chronic kidney disease? Nephrol Dial Transplant. 2008;23:2450–2453
- Canavesi E, Alfieri C, Pelusi S, Valenti L. Hepcidin and HFE protein: Iron metabolism as a target for the anemia of chronic kidney disease. World J Nephrol. 2012;1:166–176
- Xue D, He X, Zhou C. Serum hepcidin level correlates with hyperlipidemia status in patients following allograft renal transplantation. Transplant Proc. 2014;46:156–159
- Samouilidou E, Pantelias K, Petras D, et al. Serum Hepcidin Levels Are Associated With Serum Triglycerides and Interleukin-6 Concentrations in Patients With End-Stage Renal Disease. Ther Apher Dial. 2014;18:279–283