
Abstract
Chronic kidney failure can be described as a chronic and progressive disfunction in metabolic-endocrine function and in adjustment of fluid-electrolyte balance of kidney, as a result of reducing of glomerular filtration value. Besides being a medical issue, chronic kidney failure affects social, economic, and psychological conditions of patients. Indwelling catheters can be placed in the right atrium by right mini thoracotomy in kidney patients who depend on dialysis and all central veins are used. In the patients whose central veins were used, were able to do catheterization by this technique, and this is a procedure that must be retentioned.
Introduction
Chronic kidney failure (CKF) is an important public health concern in our country and worldwide due to increasing frequency and high treatment cost. Diabetes, hypertension and glomerular disease take important places in CKF etiology.Citation1 Hemodialyses is a treatment method that is based on working diffusion and ultrafiltration of renal function, for patients able to continue their lives and who lost their kidney functions because of kidney failure disease.Citation2 By regular and periodic hemodialysis, metabolic end products are discarded; fluid–electrolyte–fluid balance of body is procured. In order to perform hemodialysis, high flow supplying vascular access is a must, hemodialysis instrument, membrane (dialyzer) and sets, and medical personnel are essential. Particularly, it is not possible to make dialysis without a sufficient vascular access. Losing vascular access is the biggest problem of chronic hemodialysis. Diseases like being old, inadequate feeding, diabetes mellitus that accompany hypoalimentation, cardiovascular diseases, infections, malignite can be counted as reasons of high mortality rate at these patients.Citation3 Catheterizations which are performed with permanent hemodialysis catheters are ideal catheterizations for long lasting use like situations that do not have a chance to apply arteriovenous fistula or contraindicate to form arteriovenous fistula. Indwelling catheters are usually in silicon elastomer structure. This structure enables a catheter to be more flexible and less thrombogenic. Those catheters have infection inhibiting properties by polyester structured cuff at the point where catheters go out from the skin surface. Enabling a high volume blood flow, rapid undergoing dialysis after procedure, feeling pain after used, enabling long-term vascular access can be considered as advantages of these catheters.Citation4 We placed indwelling catheters into the right atrium of 16 patients who were out of vascular access for hemodialysis by right mini thoracotomy, which is a minimal invasive technique. We aimed to present this rare technique.
Surgical technique
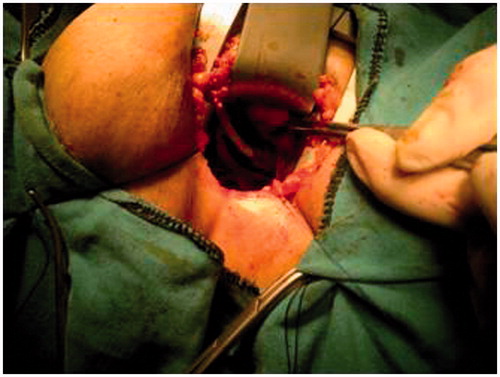
About 12 patients were male (%75), 4 patients were female (%25) of our 16 patients. The average age of patient was 62.3 (53–82). Last hemodialysis of patients could not be done because of insufficient vascular access. Peritoneal dialysis had been tried with 10 of our patients before, but patients could not continue on peritoneal dialysis because of varius problems. Peritoneal dialysis had not been performed on six patients as they were not eligible for peritoneal dialysis by the reason of abdominal operations. Central veins of patients immediately were viewed and evaluated by RDUS, in term of convenience. Vascular structure was reported as irregular, thrombosed, and occlusive partly by radiology clinic. Indwelling catheter setting to right atrium has been decided by mini thoracotomy since not enabling adequate blood flow at interventions at central vein structure before, disordered vein structure, and fragmentary occluded veins and having emergency dialysis indications in some patients and risks have been reported. Written confirmations were taken from patients. Hearth was reached by incision between right 4–5 intercostal gaps under general anesthesia. Pericard was uncovered. Four of our patients’ pericard were attached, this attached structure was removed. Purse string was applied when reached to right atrium. Guide wire was pushed forward in company with fluoroscopy to right atrium from inside of incision. After dilatation, catheter was pushed forward shifting on guide wire to right atrium and purse string was tied. Fastening sutures were applied and tied for immobilized position (). After bleeding control, tube drains were placed. Place and position of catheter were controlled with first fluoroscopy and then telecardiogram. There was no significant drainage from tube drains that were placed to patients, tube drains were pulled out, mean 2 days later. Patients' post-operation term passed without any problem and patient who took hemodialysis by this placed catheter, passed dialysis effective, and without any problem on next day.
Figure 1. Operation image of our one patient.
Discussion
Chronic kidney failure (CKF) is an important public health concern in our country and worldwide due to increasing frequency and high treatment cost. Diabetes, hypertension, and glomerular disease have an important place in CKF etiology. It is essential to take precautions, decelerating progress, and treating properly when disease first shows up since it affects all of the systems. Although kidney transplant is on the first rank in treatment options for chronic kidney failure patients, peritoneal dialysis or hemodialysis are important options which are time saving through transplant process. Donor problems at kidney transplantation restrict this treatment. On the other hand, peritoneal dialysis can be performed properly in a limited number of patients since it necessitates a good hygiene and educational level. For this reason, large majority of patients continue their lives as dependent on hemodialysis. Hemodialysis usually is performed by hemodialysis catheter or arteriovenous fistulas that were made surgically. Large majority of chronic kidney failure patients continue their lives as dependent on hemodialysis. For these patients, vascular access has vital importance. Temporary and usually indwelling hemodialysis catheters are used in patients whom arteriovenous fistulas do not provides sufficient vascular access. For indwelling catheters, usually jugular, subclavian, and femoral veins are used. If these veins were used and peritoneal dialysis can not be done, transhepatic,Citation5 and translimbalCitation6 ways can be used. These ways are technically difficult, can cause serious complications like hemothorax and pneumothorax. These complications effect mortality and morbidity negatively by prolong hospitalization of patients. We placed indwelling hemodialysis catheter to right atrium by right mini thoracotomy to 16 dialysis-dependent kidney patients whom all central veins were used. Our patients were mobilized in the same post-operation day. The most important post-operative complain of our patients was determined as wound site pain. Average hospitalization period of our patients was estimated between 3 and 8 days.Citation3–5 This technique is less invasive than trans-sternal and transhepatic methods. Since not to encounter with post-operative serious complications in our patients, this method make us think it is more safety and reliable method than others. Moreover, patients who are undergoing dialysis effectively and without having any problem at both post-operative and after discharge showed us that this method is practicable.
Result
According to us, placing indwelling hemodialysis catheter to right atrium by mini thoracotomy in patients whom all central lines were extinct is a technique that should be considered before other more invasive surgical techniques.
Declaration of interest
The authors declared no conflicts of interest with respect to the authorship and/or publication of this article.
References
- James SH, Ruffenach SJ. An overview of hemodialysis. In: Berman SS, ed. Vascular Access in Clinical Practice. 1st ed. New York: Marcel Dekker; 2002:3–13
- Tezel E, Velidedeoğlu E, Haberal M. Arteriyovenöz Fistüller. In: Haberal M, ed. Transplantasyon 1994. Ankara: Haberal Eğitim Vakfı; 1994:199–204
- El Minshawy O, Abd El Aziz T, Abd El Ghani H. Evaluation of vascular access complications in acute and chronic hemodialysis. J Vasc Access. 2004;5:76–82
- Rooijens PP, Burgmans JP, Yo TI, et al. Autogenous radial-cephalic or prosthetic brachial-antecubital forearm loop AVF in patients with compromised vessels? A randomized, multicenter study of the patency of primary hemodialysis access. J Vasc Surg. 2005;42(3):481–486
- Klahr S, Miller S. Acute oliguria. N Engl J Med. 1998;338(10):671–675
- Jenkins AL, Buist TAS, Glover SD. Medium-term follow-up of forty autogenous vein and forty (Gore-Tex) grafts for vascular acsess. Surgery. 1980;88:667–672