
Abstract
Objective: In this study, we aimed to investigate the effect of variations in renal pelvic angle on urinary calculi development. Materials and methods: A total of 2456 unenhanced abdominal CT scans were retrospectively evaluated and 262 kidneys of 131 patients were compared. Patients included in this study were identified and qualified as follows: Having unilateral calculi, having no calculi or a history of calculi in contra-lateral side and having totally normal renal morphology. Results: The mean angle of kidneys with calculi was 55 ± 9°, while the average angle measurement was 61 ± 11° in kidneys without calculi. The mean angle measured from the kidneys with calculi was statistically smaller (p < 0.001). Conclusion: Our study suggests that the possibility of calculi development in kidneys, which have more anteriorly localized pelvic angulation tends to be significantly higher in individuals, who did not have any congenital or acquired renal pathology before.
Introduction
Renal stone disease is a common condition with an incidence rate between 4% and 20% worldwide.Citation1 Underlying etiopathogenesis of renal calculi has not been fully revealed yet, although a wide spectrum of complicated mechanisms including metabolic, epidemiologic and anatomical factors have been suggested to explain the formation of renal stones.Citation1–5 Both kidneys are equally affected from these risk factors; however, stones are formed only in one kidney in some patients and the recurrence of calculi formation occurs at the same kidney. Beside this, renal stones can also be observed even in some individuals with relatively very low risk.Citation2,Citation4,Citation6 This condition does not necessarily depend on metabolic or epidemiologic factors, which in turn may suggest that structural kidney abnormalities and variations may play a role in stone formation process. The incidence of renal stone can increase due to urinary obstruction and stasis seen in some major renal abnormalities such as horseshoe kidney, malrotation, renal ectopia and fusion. However, only a few patients who have a unilateral stone suffer from abnormalities.Citation4,Citation7–10 This raises the following question: Can anatomical variations lead to stone formation? Conducted studies in this field have indicated that renal stones more commonly occur due to dependent anatomical configuration of the lower pole calyxes in addition to their other features and it is more frequent in kidneys of people who sleep at the same side position in bed.Citation2,Citation4,Citation10,Citation11 Individual habits and minor variations in anatomical structure have a disadvantage and accumulated urine has to flow into the renal pelvis against gravity, which in turn may ameliorate the calculi formation.
The CT scans of healthy people reveal that renal pelvis angles vary for each individual and even between two sides ( and ).Citation8 It can be assumed that urinary flow between the calyxes and pelvis gets slower in supine position in anteriorly faced kidney hilus. A person spends a considerable time in sleep and the possibility of renal stone occurrence is more pronounced during the nocturnal period when the urinary density reaches to its maximum point via accumulation of various crystals.Citation2 In this study, we aimed to investigate the effect of renal pelvic angle on calculi formation by evaluating the patients with unilateral kidney stone who have normal kidney morphology.
Figure 1. Difference of the renal pelvis angle from one person to another.
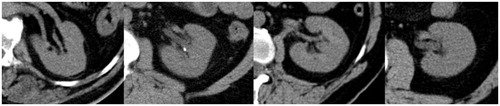
Figure 2. Difference of the renal pelvis angle from right to the left side.

Materials and methods
Patients
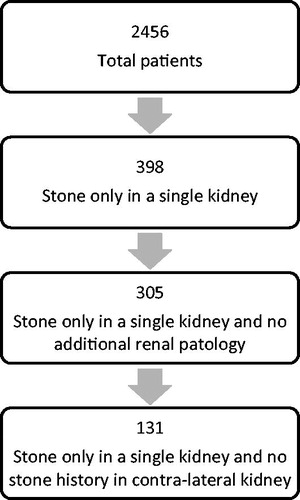
A total of 2456 unenhanced abdominal CT scans which have been performed between 1 January 2013 and 30 March 2014 dates at radiology department of our hospitals were retrospectively examined. Based on these CT scans, 398 patients who were older than 18 were identified to have a calyx stone only in one kidney. Individuals with renal parenchymal defect, chronic kidney failure, renal hypoplasia/agenesis, major renal structural abnormality (horseshoe kidney, pelvic kidney, etc) and those who have had additional pathologies such as parapelvic cysts, hydronephrosis, ureteral or pelvic stones, hepato-splenomegaly, tortuosity in renal artery, perirenal edema and inflammation, which may affect the pelvic shape-angle were excluded from the current study. Malrotations at borderline level (nonrotation, reverse rotation and hyper rotation) were not taken into consideration, whereas only the kidneys at anteromedial position within 90° of range were selected. Moreover, CT scans that displayed scoliosis and similar vertebral abnormality which might technically complicate the measurements and distorted images were not included to the study. Hospital registry records and oldest CT images of the remaining 305 cases were reviewed. Patients who have a previous history of passing stone from the other kidney were also excluded. The study was finally designed with the remaining 131 cases ().
Figure 3. Patient selection.
Evaluation of the CT images
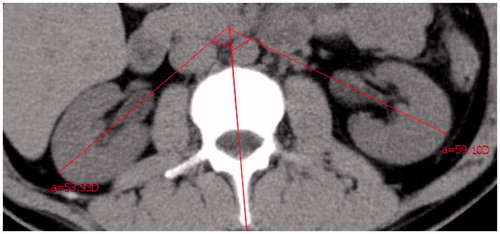
CT images were taken via using a dual-slice CT scanner (SOMATOM Spirit, Siemens Medical Systems, Erlangen, Germany). Measurements were made on scanned CT images with magnification on transverse plane. The sagittal median line that divides the adjacent vertebrae into two equal parts was taken as the vertical reference line. Slices with clear renal pelvic appearance were selected. The angular degree between renal pelvic line and the sagittal median line was accepted as the renal pelvic (or hilar) angle ().Citation8,Citation12 Whole measurements were performed on the same medical system (Siso Viewer—V2.9) and two radiologists who have more than 10 years of experience in abdominal CT field examined the images.
Figure 4. Measurement of the bilateral renal pelvis angle on computed tomography image.
Statistical analysis
Angle measurement results were assessed via using SOFA statistics v.-1.4.2 open source software (www.sofastatistics.com, Paton-Simpson & Associates Ltd.) and independent t-test was used for group comparison. Patients who have calculi were assigned to the patient group and those who did not have any stone were included to the control group.
Results
Of the whole participants, 51 were female (39%) and 80 were male (61%). The mean age was 39 ± 15 years and the age range was between 18 and 79. Mean pelvic angle of the right kidneys was 61 ± 11° (30–85), while the mean pelvic angle of the left kidneys was 55 ± 10° (34–81). The angles of both kidneys were statistically different (p < 0.001). Patients of both genders had similar renal pelvic angles in their right and left kidneys and did not display any statistically significant difference (right kidney p = 0.047; left kidney p = 0.053). In evaluation of the right kidneys, 61 (46.56%) have had stone. When the left kidneys were assessed, 70 (53.43%) kidneys were found to have stone. The mean angle of kidneys with stone was 55 ± 9° (30–82), while the mean angle of kidneys without stone was 61 ± 11° (32–85). The angle of kidneys with stone was statistically smaller (p < 0.001).
Discussion
Our study has revealed that the minor rotational variations between the right and left kidneys that were not at the borderline of anomaly could play a role in renal stone formation. Kidneys with anteriorly faced pelvis tend to more easily develop calculi. Numerous studies conducted to date have focused on to reveal the mechanisms underlying the stone formation with metabolic factors. However, this may not be enough to fully explain why calculi development occurs only in one kidney though both were exposed to same metabolic condition or why only in some renal calyces have stones in one kidney. The recurrence of stones mainly encountered at the same side with former calculi, which in turn suggests that anatomical kidney and calyx variations may play a role in this process.Citation5,Citation6
Malrotation abnormalities which seen during embryonic development are associated with horseshoe or ectopic kidneys. The abnormal course of the ureter and abnormal positioning of the ureteropelvic junction can lead to urinary stasis and stone formation.Citation7–9 Moreover, the removal speed of the calculi from a normal kidney is faster than that of the malrotated one during ESWL treatment.Citation13 These well-defined renal anomalies are known to be effective in renal stone formation and the removal speed of the calculi as well as our study demonstrates that subtle rotation differences of the kidney may also be an effective factor.
Anterior localization of the pelvis decreases the mean renal angle and this may give rise to an increase in accumulation of the calcified matters. There are two possible mechanisms which have been postulated to explain this condition: First, the passage of urine from pelvis to the ureter is probably slower in kidneys with anteriorly faced pelvis (small-angle) due to gravity during supine position sleeping, compared to those of with medially faced pelvis. This is like the flow of water from a fountain and ultimately it may lead up to partial urinary stasis. In addition to this, nocturnal stone formation is more pronounced due to the maximum saturation of urine due to several crystals,Citation2 which is disadvantageous for the kidney in supine position at night and this may induce calculi development in long term.
Second, minimal excessive or insufficient kidney rotation prevents the renal pelvis from attaching to the ureter on the same oblique-sagittal plane. This may slow down the ureteropelvic passage of urine because of a small-step effect and result in chronic partial stasis. This would predispose the kidney to stone formation.
It is a reality that people do not sleep on the only supine position at night. However, on the prone position both renal pelvises are situated in the dependent position and urinary flow is toward the gravity and on the right and left lateral positions one kidney compensates the other one. One of the kidneys fall into a disadvantageous position only on the supine situation because of the difference of its pelvic angle.
Our study was subject to specific limitations. First, this is a retrospective study and therefore, it is not possible to suggest whether the patients with unilateral renal stone will develop calculi in the other kidney as well in the future. Second, the metabolic conditions of the patients with respect to stones disease were not analyzed. Additionally, renal position change is associated with the body position.
Conclusion
In conclusion, our study demonstrates that the rotational angle of the kidney might play a role in the formation of stone in individuals with normal kidneys. Stone is formed more easily or earlier in kidneys the pelvis of which faces anteriorly. However, our findings should be confirmed by prospective studies and studies done with wider case series.
Declaration of interest
The authors declare that they have no conflict of interest.
References
- Silva SFR, Matos DC, Silva SL, Daher EF, Campos HH, Silva CAB. Chemical and morphological analysis of kidney stones: A double-blind comparative study. Acta Cir Bras. 2010;25:444–448
- Shekarriz B, Hsueh-Fu L, Marshall LS. Correlation of unilateral urolithiasis with sleep posture. J Urol. 2001;165:1085–1087
- Johri N, Cooper B, Robertson W, Choong S, Rickards D, Unwin R. An update and practical guide to renal stone management. Nephron Clin Pract. 2010;116:159–171
- Acar C, Küpeli B, Gürocak S, et al. Is pelvicaliceal anatomy a risk factor for stone formation in patients with solitary upper caliceal stone? Urology. 2006;67:1159–1163
- Besiroglu H, Otunctemur A, Ozbek E. The metabolic syndrome and urolithiasis: A systematic review and meta-analysis. Renal Fail. 2014;37:1–6
- Kupeli B, Tunc L, Acar C, et al. The impact of pelvicaliceal anatomical variation between the stone-bearing and normal contralateral kidney on stone formation in adult patients with lower caliceal stones. Int Braz J Urol. 2006;32:287–294
- Muttarak M, Sriburi T. Congenital renal anomalies detected in adulthood. Biomed Imag Interv J. 2012;8:1–8
- Sakate M, Sakate ATY, Yamashita S, Teixeira ADS, Barbosa L, Correia LA. Normal abdominal computed tomography: A retrospective study of renal hila angles. Radiol Bras. 2006;42:27–29
- Kawada S, Ichikawa T, Koizumi J, et al. Assessment of renal shape of horseshoe kidney with multidetector row CT in adult patients: Relationship between urolithiasis and renal isthmus. Tokai J Exp Clin Med. 2013;38:159–166
- Zomorrodi A, Buhluli A, Fathi S. Anatomy of the collecting system of lower pole of the kidney in patients with a single renal stone: A comparative study with individuals with normal kidneys. Saudi J Kidney Dis Transpl. 2010;21:666–672
- Gozen AS, Kilic AS, Aktoz T, Akdere H. Renal anatomical factors for the lower calyceal stone formation. Int Urol Nephrol. 2006;38:79–85
- Glodny B, Unterholzner V, Taferner B, et al. Normal kidney size and its influencing factors-a 64-slice MDCT study of 1.040 asymptomatic patients. BMC Urol. 2009;9:1–13
- Tunc L, Tokgoz H, Tan MO, Kupeli B, Karaoglan U, Bozkirli I. Stones in anomalous kidneys: Results of treatment by shock wave lithotripsy in 150 patients. Int J Urol. 2004;11:831–836