
Intraocular lymphoma has traditionally been divided into two general types—vitreoretinal lymphoma and uveal lymphoma.Citation1 These diseases are typically considered different in the structures they invade and in their behavior, prognosis, and treatment regimens. We describe a patient with a diagnosis of lymphoma involving both the iris and the vitreous both to illustrate the different components of each disease and to review an example of a masquerade syndrome.
Our patient, a 77-year-old woman, presented to an outside clinic with a chief complaint of blurry vision in her left eye (OS). Nine days prior she had developed tearing and a pressure sensation OS.
Her vision was 20/20 right eye (OD) and 20/30-2 OS. Intraocular pressure (IOP) was 16 mmHg in both eyes (OU). Anterior segment exam of the left eye revealed multiple mutton fat keratic precipitates making views of the anterior chamber cells difficult. Posterior synechiae were present inferotemporally OS. There was a 1–2+ nuclear sclerotic cataract OS. Dilated fundus exam was normal in both eyes but with a hazy view in the left eye secondary to the keratic precipitates. Quantiferon TB gold, ACE, and FTA ABS were negative, while lysozyme was “slightly elevated.” Prednisolone 1% drops and cyclopentolate drops were started OS. On follow-up, acyclovir 400 mg by mouth 5 times daily was begun.
Nine days after initial presentation, her IOP rose to 52 mmHg OS. She was given a sub-Tenon’s dexamethasone injection, received a few unknown doses of acetazolamide orally, and was started on brinzolamide and brimonidine drops, while atropine was substituted for cyclopentolate. The next day’s IOP had decreased to 8 mmHg. Acyclovir and previous eyedrops were continued while dexamethasone drops were added every hour. Eventually the keratic precipitates extended through the rest of her cornea. A small neovascular area appeared at the pupil margin at about 3 o’clock in the iris, and this region appeared slightly elevated. IOP rose to 23 mmHg a few weeks later so a “low dose” of acetazolamide was initiated. Anterior segment optical coherence tomography and gonioscopy did not reveal abnormalities.
At the time of referral to our institution, the patient was taking drops of dexamethasone 0.1%, homatropine, brimonidine, brinzolamide, as well as acetazolamide 500 mg twice daily. Her vision was 20/20 OD and 20/60+2 OS. IOP were 11 and 28 mmHg OD and OS, respectively. She had 2+ anterior chamber cells and macular edema OS but no other abnormalities on her fundus examination. A sub-Tenon’s injection of triamcinolone for inflammation improvement was given OS. Serologies for ANA, Bartonella henselae, Bartonella quintana, Lyme antibody, ANCA, rheumatoid factor, RPR, and HLA B27 were all negative.
Our patient was followed at the outside institution for the next 3 months. During this time, the patient underwent a combined cataract extraction plus aqueous drainage shunt placement, and intraoperative samples for HSV, VZV, and CMV PCRs were negative. Upon return to our institution, she was found to have left eye visual acuity of 20/100, IOP 19 mmHg, new temporal iris mass with neovascularization (), and persistent anterior chamber cells. Her CBC was normal and serologies for syphilis, toxoplasmosis, and toxocariasis were negative. ACE was found to be within normal limits with an elevated lysozyme of 28 μg/mL. Due to the extent of her anterior chamber inflammation, including her keratic precipitates, iris mass, poor dilation, and anterior chamber cells, a view of the fundus was very limited (). Macular OCT did not reveal much more detail (). For this reason, and to better characterize her iris mass, an ocular ultrasound was planned.
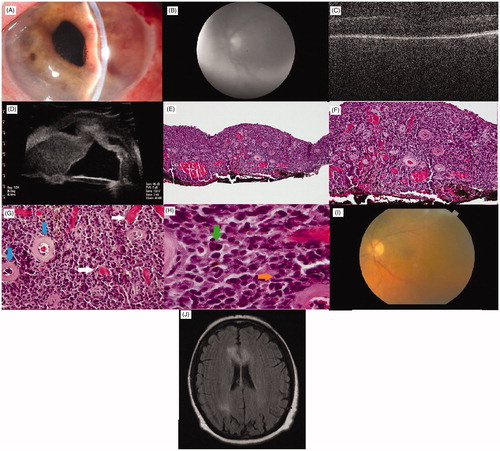
FIGURE 1. (A) Slit lamp photograph of anterior segment of left eye prior to surgery. Note raised contour of iris and keratic precipitates. Note also temporal iris neovascularization. (B) Red free photograph of fundus of left eye prior to surgery. Poor view secondary to keratic precipitates and vitreous debris. (C) OCT of the macula of the left eye prior to surgery. (D) Ultrasound showing thickened iris stroma actually touching cornea. E–H. Representative light photomicrographs of a diffuse lymphoproliferative infiltration of the iris stroma, involving the entire specimen. The infiltrate consists of large lymphocytes demonstrating malignant features including pleomorphism, high nuclear:cytoplasmic ratios, clumped chromatin and rare nucleoli. Note also the prominent vascularity of the iris stroma. (E) The tumor infiltrate is composed of large lymphocytic cells present throughout the entire iris, (hematoxylin-eosin stain; original magnification 100×). (F) Appearance of densely packed, large cell lymphoma that overwhelms the normal loose architecture of the iris stroma (hematoxylin-eosin stain; original magnification 200×). (G) Throughout the iris there is an increased amount of vascular channels (horizontal arrows) among the normal hyalinized appearing vessels (vertical arrows) (hematoxylin-eosin stain; original magnification 400×). (H) Higher power view showing large pleomorphic tumor cells with indistinct cell borders, clumped chromatin (vertical arrow) and mitotic figures (horizontal arrow) (hematoxylin-eosin stain; original magnification 1000×). (I) Color fundus photo of the left eye months after surgery. (J) MRI brain. Axial image with FLAIR showing bilateral enhancement of the corpus callosum along with involvement of the right parietal lobe.
Ocular ultrasound showed a normal-appearing retina and choroid, with mild intravitreal opacities, implying a vitritis that could not be seen on exam. Immersion scan using high-frequency 35-MHz probe to visualize the anterior segment revealed iris and ciliary body masses in 3 quadrants (). This was most suggestive of an infiltrative process, e.g., lymphoproliferative disease, amelanotic melanoma, parasitic process, or other nonspecific inflammation.
An iris biopsy combined with vitreous biopsy was planned, and to decrease intraoperative hemorrhage an intravitreal injection of bevacizumab was given OS in clinic. Two days later she had a vitrectomy and iris biopsy. She tolerated the procedure well and postoperative day 1 had an IOP of 15 mmHg.
Analysis of the vitreous specimen revealed that lymphocytes were present. There was a mixture of B cells and T cells and the T cells were heterogeneous with a CD4:CD8 ratio of 8.7. Flow cytometry was used to determine that the B cells were monoclonal. It was also found that the B cells “express kappa light chains, CD19, and CD20, but do not express CD5 or CD10.” The vitreous specimen was deemed “suggestive of a B-cell lymphoproliferative disorder."
The iris biopsy showed large atypical lymphoid cells with high nuclear to cytoplasmic ratio, vesicular chromatin, and prominent nucleoli with relatively scant cytoplasm. Immunohistochemical studies were positive for CD20, BCL2, BLC6, and MUM-1, along with negative CD3, which confirmed the diagnosis of large B-cell lymphoma. Through the MIB1 stain, there was found to be a proliferative rate of >90%. Examination of the specimen with light microscopy revealed medium-sized lymphocytes with occasional clumped chromatin with rare nucleoli ().
Postoperatively, her iris dilated to a greater extent and a better view of the left fundus was obtained. No retinal infiltrates were noted (). A lumbar puncture performed at an outside hospital reportedly showed no abnormalities according to the patient’s hematologist, though the records were not obtained prior to the patient moving to a different part of the country and no flow cytometry was done on the sample. An MRI of the brain showed bifrontal enhancement involving the corpus callosum and an additional 1.5-cm enhancement in the parietal lobe (), which was also considered to be from lymphoma. The patient also had a PET scan, which was reviewed with a radiologist who specialized in nuclear medicine at our facility who confirmed that outside the head, the PET scan showed no abnormalities. The PET scan stopped at the waist so did not show any of the lower extremities. The patient was referred to an oncologist who concurred with a diagnosis of intraocular and central nervous system (CNS) lymphoma.
Systemic and intrathecal chemotherapy, whole brain and ocular radiotherapy, and intraocular chemotherapy with rituximab and/or methotrexate were discussed. Per their notes, the oncologists spoke with the patient about the fact that systemic chemotherapy would involve the patient spending significant amounts of time in the hospital. Our patient was more concerned with quality of life at the time and opted against systemic chemotherapy with the associated side effects and required hospital stays. It was felt that since systemic chemotherapy would not be administered, a bone marrow biopsy would not significantly contribute to the decision-making process for the patient so it was not performed. Our patient opted for intraocular methotrexate and she also took routine postoperative ophthalmic medications.
During her workup by oncology, she was also found to have a lesion on her medial right ankle. A punch biopsy was taken and the results were as follows. There was a “diffuse and focally nodular infiltrate of large and atypical mononuclear cells.” These cells had a moderate amount of cytoplasm with prominent nucleoli. Apoptotic bodies and mitotic figures were prominent. Immunohistochemical staining was performed and revealed “a large population of CD20 positive cells,… with a background population of CD3 positive cells.” Most of the large cells were positive for BCL 2, BCL 6, and IRF4/Mum-1, which implies the same phenotype as the lymphocytes found in the iris. CD10 positive cells were rare. The biopsy sample was reviewed by three separate pathologists, including a hematopathologist and a dermatopathologist, who agreed that with the clinical setting, this was consistent with systemic large B-cell lymphoma with secondary involvement of the skin.
After a few months our patient moved to a different part of the country and decided to undergo brain and ankle radiation treatment. At the first visit with her new ophthalmologist, she was found to be 20/20 OD and 20/200 with pinhole to 20/80 + 2 OS. She still had keratic precipitates inferiorly OS along with posterior synechiae from 1:30 to 2:30. Regrettably, she passed away from complications related to metastatic lymphoma 3 months later.
Classically, iridal lymphoma and vitreoretinal lymphoma have been considered two different diseases, though involvement of the iris and vitreous has been reported to occur in the same eye simultaneously.Citation2 It is thought that lymphoma of the uveal tissues tends to be less aggressive than lymphoma involving the vitreous or retina. Our patient’s simultaneous finding of central nervous system involvement, and final diagnosis of large B-cell lymphoma would seemingly make her case more consistent with that of a vitreoretinal lymphoma and, more specifically, a central nervous system lymphoma (CNSL); however, her anterior uveitis with keratic precipitates and an elevated intraocular pressure all correlate well with iridal lymphoma. Anterior segment inflammation is typically uncommon in the case of vitreoretinal lymphoma. This dilemma makes treatment planning challenging as CNSL tends to be quite aggressive, while uveal lymphomas are not quite so. As she had central nervous system involvement and her histologic diagnosis was that of a more aggressive tumor it seemed appropriate to approach this situation as if our patient had a more aggressive tumor.Citation1,Citation3
Another critical dimension of this case is that of diagnostic confusion. This patient’s presentation is an excellent example of masquerade syndrome, which ultimately was diagnosed as an unusual case of lymphoma involving the iris, vitreous, CNS, and ankle. Initially she was approached as having an anterior uveitis and she responded well to topical steroid treatment. According to a retrospective case series by Rothova et al., out of 828 patients diagnosed with uveitis, 40 were diagnosed with a uveitic masquerade syndrome and out of those 40, 13 were found to have intraocular lymphoma—the most common type of malignancy encountered in the study.Citation4
Our patient’s intraocular pressure continued to climb in spite of medical therapy, and the development of an iris mass was ominous. This is not, in fact, that unusual in the case of an iridal lymphoma, as is described in a case report by Duker et al.Citation5, and in the case series by Mashayekhi et al.Citation3 In this series of 14 eyes from 13 patients diagnosed with iridal lymphoma, 6 were treated with topical, periocular, and/or systemic steroids prior to their final diagnosis. Similarly, the patient described by Ahmed et al.Citation6 was also treated with steroids prior to a final diagnosis. Seven of the patients had previously been diagnosed with lymphoma elsewhere in the body, with only 1 patient having the brain involved. Every patient had an anterior chamber reaction and 10 out of the 13 had keratic precipitates. While the authors of this series note that follow-up was one of the shortcomings of the study, it should be noted that the prognosis depends heavily on whether there is systemic involvement at diagnosis.Citation3 A previously reported patient with iris, vitreous, and central nervous system involvement remained tumor-free after 6 years of follow-up following systemic and vitreous chemotherapy. This patient unfortunately also developed neovascular glaucoma in her affected eye and needed an enucleation. No lymphoma cells were found in the eye after enucleation, illustrating that these patients may do well from a tumor standpoint yet develop other complications such as glaucoma.Citation2
In our patient, it was unclear whether her primary diagnosis should be that of primary central nervous system lymphoma or iridal lymphoma. She had characteristics of both and both diagnoses were made simultaneously. The iris mass was not noted at her presentation, but anterior segment inflammation was present from the start. It is possible that earlier ocular ultrasound (including ultrasound biomicroscopy of the anterior segment) could have led to an earlier diagnosis. This exemplifies the importance of including masquerade syndromes such as lymphoma on the differential of patients with difficult-to-control intraocular inflammation. While this is one patient, it is possible that uveal and vitreoretinal lymphoma could be considered part of a spectrum of disease rather than two completely separate disease states.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
Supported in part by an Unrestricted Grant from Research to Prevent Blindness, Inc., New York, NY, to the Department of Ophthalmology & Visual Sciences, University of Utah.
References
- Chan CC, Rubenstein JL, Coupland SE, et al. Primary vitreoretinal lymphoma: a report from an International Primary Central Nervous System Lymphoma Collaborative Group symposium. Oncologist. 2011;16:1589–1599
- Velez G, de Smet MD, Whitcup SM, et al. Iris involvement in primary intraocular lymphoma: report of two cases and review of the literature. Surv Ophthalmol. 2000;44:518–526
- Mashayekhi A, Shields CL, Shields JA. Iris involvement by lymphoma: a review of 13 cases. Clin Exp Ophthalmol. 2013;41:19–26
- Rothova A, Ooigman F, Kerkhoff F, et al. Uveitis masquerade syndromes. Ophthalmology. 2001;108:386–399
- Duker JS, Shields JA, Ross M. Intraocular large cell lymphoma presenting as massive thickening of the uveal tract. Retina. 1987;7:41–45
- Ahmed M, Androudi S, Brazitikos P, et al. 360 degrees iris-ciliary body B-cell lymphoma masquerading as post-cataract uveitis. Semin Ophthalmol. 2004;19:127–129