Abstract
Purpose: Visual disturbances that make it difficult to read text are often termed “visual stress”. Coloured filters in spectacles may help some children overcome reading problems that are often caused by visual stress. It has been suggested that for optimal effect each child requires an individually prescribed colour for each eye, as determined in systems such as the “Harris Foundation” coloured filters. Alternatively, it has been argued that only blue or yellow filters, as used in the “Dyslexia Research Trust” (DRT) filter system, are necessary to affect the underlying physiology. Method: A randomised, double blind trial with 73 delayed readers, was undertaken to compare changes in reading and spelling as well as irregular and non-word reading skills after 3 months of wearing either the Harris or the DRT filters. Results: Reading improved significantly after wearing either type of filter (t = −8.4, p < 0.01), with 40% of the children improving their reading age by 6 months or more during the 3 month trial. However, spelling ability (t = 2.1, p = 0.05) and non-word reading (f = 4.7, p < 0.05) improved significantly more with the DRT than with the Harris filters. Conclusion: Education and rehabilitation professionals should therefore, consider coloured filters as an effective intervention for delayed readers experiencing visual stress.
Any disability that impacts on a child’s capacity to read has serious implications for academic development as well as the ability to participate independently in activities of daily living.
One reading disability, generally termed “visual stress”, is related to visual disturbances that make it difficult to read text.
This research demonstrates the beneficial use of coloured filters for promoting visual reading capacity for children with visual stress.
Professionals who are involved in the needs of children with reading delay, may like to consider the benefits that coloured filters can afford children with visual reading problems.
Implications for Rehabilitation
Introduction
In a typical school day, children spend up to 60% of their time on reading, writing and other close work [Citation1]. Any disability that impacts on a child’s capacity to read, or to learn to read, or to read their own writing, therefore, has serious implications for academic development as well as the ability to participate independently in activities of daily living, work and leisure. Impaired reading capacity can lead, not only to reduced educational outcomes, but also to secondary emotional and behavioural difficulties [Citation2]. Education professionals are well placed to identify those children with delayed reading abilities, but both educational and rehabilitation professionals, such as special needs educators, occupational therapists and psychologists as well as optometrists and orthoptists need to be aware of the varied causes of reading disabilities, and the wide range of interventions available. Although there have been major developments in the perceptual and vision literature for some of these professions, for example the publication of several detailed guides for occupational therapists working in the domain of functional visual behaviour [Citation3–5], there are some disabilities and related interventions that affect reading ability, which require more professional attention.
One lesser known reading disability, generally termed as “visual stress”, is related to visual disturbances that make it difficult to read text [Citation6–8]. People experience one or more of the following: words seem to blur, the letters move around, go double or the white spaces glare [Citation9]. However, people, especially children, with this visual disturbance do not always realise that others do not experience these same difficulties and therefore do not commonly report their problems. The effects of visual stress include visual discomfort, headaches and tiredness. These symptoms lead to a reduced reading duration capacity and a lack of ability to read with sufficient fluency to grasp meaning. The prevalence is though to be high at 5–20% of the population [Citation10], however, in people with dyslexia it is thought to be even higher at around 35–40% [Citation9]. The use of coloured filters to alleviate it was recognised in 1980 by Olive Meares, a school teacher in New Zealand [Citation11], but the condition has been well known to optometrists for many decades with early pioneers such as Kraskin and Skeffington advocating the use of stress-relieving lenses to ameliorate discomfort and permit optimal visual efficiency [Citation12].
Theories about the causes of visual stress
A variety of theories have been developed to explain the mechanisms whereby coloured filters can relieve visual stress. Irlen suggests that it is sensitivity to certain wavelengths of light that distort the perception of the environment; she called the problem Scotopic Sensitivity Syndrome [Citation7]. She thought that the syndrome included light sensitivity, inadequate background accommodation, poor print resolution, restricted span recognition and lack of sustained attention. Wilkins developed the visual stress hypothesis and refers to the condition as Meares–Irlen syndrome to give honour to the early pioneers [Citation8,Citation10]. He suggests that some people have an abnormal visual cortex rendering them hypersensitive to coarse high contrast stripes, such as lines of black text on a white background. He proposes that this interferes with their control of accommodation and convergence, which is why they experience distortions and apparent text motion.
The binocular vision theory of visual stress views poor capacity in convergence, accommodation and fusion as the cause of visual symptoms when doing close work [Citation13]. Binocular vision involves the control and co-ordination of both eyes; it has a role in maintaining single clear vision when reading.
Stein’s theories focus on the role of the magnocellular system [Citation14–16]. If this system is developmentally impaired, he suggests that high contrast lines of text may saturate magnocells giving rise to the symptoms of visual stress. Alternatively, Harris’ theory proposes that there may be differences between the two eyes in transmitting visual information to the brain, which might cause information from one eye to arrive in the visual cortex later than from the other eye [Citation17].
The use of coloured filters as an intervention.
Since Meares’ observations in the 1980, the benefits of coloured overlays, to improve perception of text, have been well documented [Citation18]. In order to facilitate reading and composing text, the manipulation of colour (background or foreground colour) has become recognised as a useful form of assistive technology for people with learning disabilities [Citation19] as well as a method of cognitive intervention within neuropsychological rehabilitation [Citation20].
In the 1980s, the use of coloured overlays was developed into using coloured filters in spectacles. This was a welcome advance as it allowed for the therapeutic benefits of being able to read at close range, to extend reading from the board at the front of a classroom or overseeing writing as it is undertaken. The different theories, which underpin views of what causes visual stress, have led to different coloured filter systems being developed. However, few professionals are educated in the use of coloured filter spectacles although they may be important to consider as an intervention. Further detail on some of the systems available will be discussed now.
Irlen was the first to patent a set of coloured filter lenses for treatment purposes in 1983 [Citation21]; she felt that a different colour was needed for each child [Citation7]. In the next decade, Wilkins et al. [Citation22] developed the “intuitive colorimeter” to help in selecting the specific tint optimal for each child. They felt that coloured filters may alleviate these symptoms by rebalancing input to the visual cortex. This system was used to choose the correct colour for spectacle filters, known as Medical Research Council (MRC) “intuitive” filters [Citation23].
The Dyslexia Research Trust (DRT) system was founded in 1995 by Stein and Fowler [Citation24]. Arguing from the important role of the visual magnocellular system in reading, they developed the DRT deep blue or deep yellow filters. The glasses were worn with the same colours being used for both eyes; the choice between the two colours was determined by the subjects’ symptoms. DRT filters used just the two colours as it was proposed that only these two colours had specific effects on the magnocellular system [Citation14].
Harris, developed two filter systems: initially he developed the ChromaGen filters [Citation25] and subsequently the Harris Foundation filters [Citation26]. These both involved a range of colours; but different colours are prescribed for each eye.
Efficacy of coloured filters in spectacles
However, the use of coloured-filtered spectacles to reduce the impact of visual stress on reading is controversial and some in the scientific community remain highly sceptical about whether they really help at all [Citation27]. Although anecdotal evidence of the benefits is compelling, with individuals reporting that the effects are “life changing” [Citation28], the scientific community requires rigorously conducted research trials as evidence. Key studies have tended to be small placebo controlled trials of individually prescribed coloured filters. Wilkins et al. [Citation18] found a small decrease in visual symptoms in 36 children wearing their chosen coloured filters compared with a different hue as placebo. In only seven were these improvements statistically significant; and more than half the subjects ceased wearing the filters. Mitchell et al. [Citation29] carried out a similar study in 49 children with similar modest results. Robinson & Foreman [Citation30] found that blue improved reading as much as any individually prescribed colours. Using individually prescribed coloured overlays, Bouldoukian et al. [Citation31] improved 33 such children’s reading speed by an average of 4% compared with a standard pale yellow overlay. In 2005, Ray et al. [Citation16] carried out a double blind, placebo controlled trial and found that yellow filters improved reading significantly more than placebo in selected children. They improved reading by almost three standard points; this was equivalent to an increase in reading age of 7 months in 3 months (i.e. 2.3 months per month). Wearing the yellow filters also improved the children’s motion sensitivity, convergence and accommodation control.
In an open study of people with reading difficulties the effect on reading rate of ChromaGen contact filters was compared with the Wilkins MRC “intuitive” filters [Citation32]. The ChromaGen filters were found to increase reading speed by 1.3 standard deviations, whereas the MRC filters only increased it by 0.9 sds. Thus, this trial suggested that ChromaGen filters were superior to the MRC filters, although the findings were not published in a peer reviewed journal. In a subsequent double blind, randomised control study, Harris & MacRow-Hill [Citation33] found that the ChromaGen filters were also greatly superior to placebo plano filters. Harris has since developed Harris Foundation filters. In summary although some studies have failed to show a significant effect of coloured filters [Citation34,Citation35] on reading the majority have shown that several different filter systems achieved small positive effects compared with placebo [Citation16,Citation18,Citation21,Citation32,Citation36].
There has yet to be a trial comparing the effect of Harris Foundation filters [Citation26] with DRT filters [Citation24] on measures of single word reading and spelling skills. Following a request from the Bath & NE Somerset Director of Education to trial some contemporary filter systems, this study aimed to compare the latest Harris Foundation filters with the DRT blue and yellow filters on reading and spelling ability in a sample of poorly reading UK primary school children.
Methods
Design
The study design was a pre-test, post-test, randomised trial which involved a “head-to-head” comparison of the efficacy of two-coloured filter systems on a single word reading and spelling and the reading of irregular and non-words in primary school children. No untreated control group was judged necessary as each system had previously demonstrated efficacy in its own right and it was ethically unjustified to use a placebo intervention when it had been previously shown to have no benefit to children. Ethics approval was gained from Oxford Research Ethics Committee (01.02).
Participants
A power calculation demonstrated that 30 participants would be required for each group to demonstrate a statistically significant effect of intervention. This also matched successfully conducted trials, which have included between 30 and 50 children.
Inclusion criteria: children in main stream state primary schools were chosen to provide a sample which would represent the typical academic range of primary school children in the UK. In order to include children who were potentially experiencing visual stress, children with a significant impairment in reading capacity, whom the school identified as at least 18 months behind that expected for their age, were selected. Specific additional conditions such as dyslexia were not of relevance, as visual stress is not exclusive to any such condition. Children who normally used spectacles for reading were also included; the prescription was either put into tinted lenses or they wore both sets of spectacles together, one on top of the other. Children between the ages of 7 and 10 were chosen as they were old enough to manage to wear the glasses but young enough that their reading capacity was still developing.
Exclusion criteria: children whose first language was not English were excluded, as this would have added the compounding variable of cultural issues of language acquisition.
Recruitment
The Local Education Authority for the Bath area gave permission for primary schools to provide a population sufficient to recruit the sample of 70 children. Following Head teacher’s permission, data was collected on delayed readers and 87 children who met the inclusion criteria were identified. The parents of these 87 children were invited to give written informed consent for their child to join the study. All consented but one parent later withdrew consent leaving a total of 86 participants for the study.
Materials and procedure
Baseline testing
In order to ensure that intervention groups were comparable at baseline, many visual and psychometric measures were taken.
The children’s convergence, accommodation and visual acuity were tested. Visual acuity was tested using the Snellen chart, and the nearpoints for convergence and accommodation were tested using the RAF Binocular guage [Citation37]. From this data, an orthopist identified 14 children with reduced visual acuity. They were referred for an optometric assessment to ensure that this issue was addressed prior to the study. All 14 children were included in the study.
General academic ability was tested using subtests of the British Abilities Scales (BAS II): similarities, matrices, recall of digits, reading and spelling. The BAS II subtests are valid and reliable for this population and have been standardised in the UK using very large number of children to determine the normal distribution of scores at a given age.
The children were also tested for processing skills within reading, pre and post intervention. In order to test irregular and non-word reading skills the Castles and Coltheart’s irregular and non-word lists were used [Citation38]. Irregular words like “yacht”, the correct pronunciation of which cannot be worked out using normal letter to sound rules, but require memory of the visual “orthographic” form of the word. Non-words, are invented words, for example “tegwop”, that can only be read if a child is proficient in using the English letter to sound conversion rules. The children were timed whilst they read the 30 words in each of the two lists. In keeping with the published test procedures they were instructed to move on quickly if they could not read a word. As accuracy in reading ability needs to be combined with reading speed to represent reading capacity, time per correct word was used to measure irregular and non-word reading capacity.
Some children had to be excluded from participation at the start of the study or from the analysis at the post-test stage following testing with the word lists. During the word list tests, if they were only able to read the first word and then struggled on the second and subsequent ones, they would have artificially elevated the time per correct word score. If they read only one word correctly and then looked ahead at the remaining words and said that they would not be able to read any more they would have achieved an artificially short time per correct word.
Age was the final baseline variable collected
As seen in , those receiving Harris filters were by chance younger (p < 0.01) than those receiving the DRT blue or yellow filters. Although the baseline data of the Harris children suggested they were slightly more intelligent and slightly better readers than the other group, these differences were not significant. The general academic capacity of both groups was within normal limits, but at the 30th percentile it was lower than the population mean. As expected their reading and spelling were much worse, being 1.3 SD behind the population mean (10th percentile).
Table 1. Summary statistics*.
Dependent variables
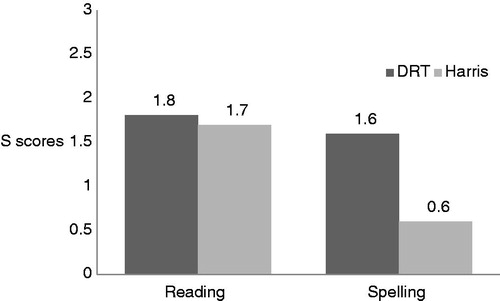
The primary dependent variables of single word reading and spelling were measured before and after wearing the filters. The s scores from the BAS II reading and spelling scales were used to measure reading and spelling skills and the Castles and Coltheart’s lists [Citation38] were used when measuring the number of accurate irregular and non-word words read per second were measured (). Spelling was included because this is thought to give a more accurate reflection of children’s visual word memory.
Figure 1. Increase in reading and spelling BAS II “s” scores after 3 months use of DRT or Harris filters.
Intervention
DRT filters
To decide whether the blue or yellow filter might help a child most, each child was shown both a paragraph of N8 sized text and a sheet covered with randomly grouped letters and symbols. They were then asked to look through the blue and yellow filters to see if either made the material any easier to see. The DRT blue filter had a transmission spectrum equivalent to Kodak Wratten filter no. 47b and the yellow, Wratten 15. If the child said that one of the coloured filters made the letters look clearer, they were asked to use that colour in spectacles for the next 3 months, only for reading and writing work. This process took less than 5 min per child.
Harris filters
The Harris Foundation system requires assessors to help children to select the optimal colour; each child is helped to choose a colour that helps reading, and not just a colour they like. A diagnostic set of 13 different colours ranging from red, through yellow to blue are offered through the assessment. Harris had found that the greatest improvements in reading speed, came when different colours were selected for each eye using a haploscopic technique. This method was therefore followed. First the child was given a small telescope and asked to look through it; as they would choose their preferred eye, the examiner could determine which the dominant eye was. They were then helped to select the best filter first for the non-dominant eye, then for the dominant eye according to the filter developer procedures the second filter was always different. This process took 15–30 min per child.
General intervention procedures
The seven children with reduced visual acuity, who were allocated Harris lenses, saw an optometrist who provided the prescription and pupillary distance for reading, so that the Harris Foundation lens makers could make the necessary corrective lenses, with appropriate tints. Seven children with reduced visual acuity, who were allocated DRT filters, had to wear two spectacle frames at the same time when they read; their prescription lenses in one set; the appropriate DRT tinted lenses in the other set. All the children were given the same instructions, and all teachers and Special Educational Needs co-ordinators were asked to work with the children in the same manner. Otherwise the children received no special help and were taught in the standard way for that school. Compliance was ascertained through individual teacher report.
Group allocation
The schools’ data including examination results provided by the Local Education Authority were used to form two comparable groups of nine schools, each group thereby containing a similar profile of social background and school exam achievement.
Randomisation
Using a table of random numbers, an independent researcher then assigned the Harris filters to one group of schools providing 44 participants and the DRT filters to the other providing 42 participants; the allocations were held in sealed envelopes which were not opened until after baseline testing had occurred. Once baseline tests had been carried out, children were then offered the filter system assigned to that school. The children then went through either the Harris Foundation or DRT procedure for selecting the appropriate colours. If they found the filter made the letters look clearer, they were asked to wear the appropriate spectacles for all reading and writing work for 3 months. Of the 86 children, 73 (85% of those seen) said that a filter helped them during the filter assessment and agreed to wear the filtered spectacles for all reading and writing for the three-month period. In total, 37 children wore the DRT and 36 children the Harris Foundation filters.
Post testing procedure
After 3 months, the children were retested without filters by a different researcher to those involved in the initial filter assessment selection. The children were asked not to bring their filters or to say which filters they had been wearing. Thus, this researcher was blind to the type of filter that had been used, and she was not given any of the baseline data. To measure effect on single word reading, spelling and irregular and non-word skills she retested the children’s BAS II reading and spelling and time per correct word on the Castles and Coltheart’s lists. At the post-test stage, of the 73 who had participated in the study, five children from the DRT group and four from the Harris Foundation group had to be excluded as they only read one word during the Castles and Coltheart’s irregular and non-word lists, leaving 32 in both. The children did not know which filter might help them and were not told about the differences between DRT and Harris filters.
Results
Reading and spelling
Reading and spelling scores were approximately normally distributed. At their baseline testing the two groups did not differ significantly in BAS II reading or spelling s scores (for reading t = 1.3, p = 0.3; for spelling t = 1.7, p = 0.09). The p values varied due to differences in variance. But, as shown in , after wearing for 3 months either kind of filter both the DRT and the Harris Foundation filter groups had improved with DRT filters improving reading s scores by 1.8 and Harris by 1.7: together these scores had improved, by an average of 1.8 score points; this is equivalent to 4.5 months increase in reading age over the 3 months, i.e. 1.5 months more than you would expect for an average child’s progress. Overall, 40% of the children improved their reading age by 6 months or more during the 3 month trial (t = −8.4, p < 0.01). The increase in s score were statistically significant for both the DRT filters: t = 3.0, p < 0.05, and for the Harris Foundation filters: t = 2.6, p < 0.05; average effect size: d = 0.17.
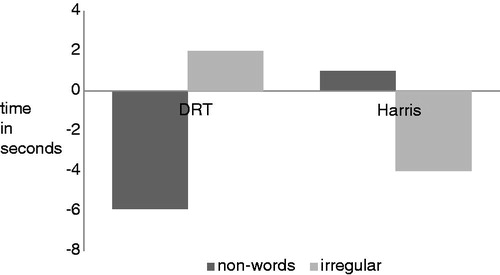
Figure 2. Change in non-word and irregular word reading time (s).
The children’s spelling did not improve quite so much; those allocated the DRT filters improved by 1.6 score points (equivalent to spelling age improvement of five months); this was still statistically significant (t = 2.1, p = 0.05); but the spelling of the children who received the Harris Foundation filters t’s improved by only 0.6 points which was not statistically significant (t = 0.8, p = 0.4).
We compared the standard scores before and after the DRT and Harris Foundation filters using a mixed design ANOVA; this showed that there were no statistically significant differences between the DRT and Harris Foundation children’s improvements on BAS II reading (f = 0.001, p = 0.9) or spelling (f = 0.9, p = 0.3). Because of the difference between the groups’ ages we also controlled for age as a covariate. But this made no statistically significant difference to the effects.
At the first testing session, there were no significant differences between the groups’ irregular and non-word reading capacity (for irregular words: t = 0.2, p > 0.9; for non-words: t = 1.1, p = 0.1). But, as shown in , after wearing the DRT filters for 3 months, the children’s non-word reading had improved. They took 5.9 s less to read the non-words. However, after wearing the Harris Foundation filters, the children were 1 s slower at reading the non-words. Thus, the DRT filter wearers improved the children’s non-word reading time significantly more than the Harris Foundation filter wearers did (f = 4.7, p < 0.05). This significant advantage of the DRT filters remained even after age had been controlled for (f = 4.3, p < 0.05). But neither the DRT nor the Harris Foundation filters had a statistically significant effect on irregular word reading (mixed design repeated measures ANOVA: f = 0.5, p = 0.5).
Discussion
We compared the reading, spelling and irregular and non-word reading capacity of children with significant reading delay before and after wearing either Harris Foundation or DRT filters to see how Harris Foundation filters compared with the DRT ones.
Given the more thorough and lengthy assessment process for Harris filters and the wider range of colours on offer, it might have been expected that the Harris Foundation system would be more effective than the DRT system. However, it transpired that the DRT filters improved literacy in some tests at least as much as, and in others significantly more than, the Harris Foundation filters did. Both Harris Foundation and DRT filters helped children to improve their BAS II reading scores by similar amounts. But the DRT filters improved spelling more than the Harris Foundation filters did. Furthermore the DRT filters improved non-word reading significantly more than the Harris Foundation filters did, although neither type improved irregular word reading significantly. These improvements are not only statistically but also clinically significant. Without treatment poor readers tend to fall further and further behind their classmates [Citation39]. Reading improvements of 4.5 months in 3 months mean that the children have begun to catch up with their peers.
The results support that of the Ray et al. study [Citation16], which showed in a double blind, randomised control, trial that deep yellow filters were significantly more effective than a placebo in improving single word reading and spelling in some children. These effects were expected as yellow increases input to the magnocellular system by selectively stimulating both the L- and M-cones that provide the main input to magnocells. This suggests that the DRT filters work by affecting basic visual processing via the retinogeniculate magnocellular pathway that deals with motion information and controls visual attention and eye movements [Citation15,Citation40–42].
The DRT filters improved non-word reading significantly more than the Harris Foundation filters did, though neither improved irregular word reading significantly. This may seem surprising since non-word reading is thought of as more of a phonological than visual task; whereas irregular word reading is thought to be more visual. But Cestnick & Coltheart [Citation43] showed that a magnocellular test, the Ternus task, predicted non-word reading better than irregular word reading. Their explanation was that non-word reading requires serial left-to-right allocation of covert attention and eye movements across the letter string being read. Since the magnocellular system is known to control this attentional process [Citation42], our finding adds further support to the magnocellular theory, suggesting that one of its important roles in reading is to help sequence the visual focus of attention, and reading eye movements [Citation35].
The average improvements in reading which we report here are not large. This is probably because the general intelligence of the present sample was lower than 100. It could be hypothesized that improvements would be more impressive for those with higher intelligence as, once facilitated to read, their potential for reading development would be greater. Whilst we believe that filters should be made available to all children, we expect that those whose reading and spelling are well behind higher other abilities, will probably benefit most.
There are differences in the costs and training requirements for the two systems. The DRT filters can be obtained at a much lower cost than the Harris Foundation filters and do not require the use of expensive equipment or the training of assessors. Assessment time is also shorter.
Conclusion
Thus, the simple blue or yellow DRT filters, with short assessment times and low material cost, seem to be at least as, or more, effective than the individually selected Harris Foundation hues. This research will help to support the use of coloured filters for visual reading capacity but further more rigorous research is being planned. A large randomised controlled trial will be conducted in the coming years and the key researchers in the field are collaborating to develop a consensus for an exemplary research protocol for this study.
All those professionals who are involved in the needs of children with reading delay, such as primary school teachers, SENCOs, educational psychologists and occupational therapists may like to consider the benefits that coloured filters can afford children with visual reading problems.
Declaration of interest
One of the authors developed one of the filter systems tested in this research study, however the author makes no financial profit from the sale of these filters as they are distributed through a non-profit organisation. Every measure has been taken in the study design and execution to ensure that the study has been conducted without risk of bias.
Acknowledgements
The authors would like to thank all the children, parents and education staff who supported or participated in this study.
References
- McHale K, Cermak S. Fine motor activities in elementary school: preliminary findings and provisional implications for children with fine motor problems. Am J Occup Ther 1992;46:898–903
- Titcomb RE, Okoye R, Schiff S. Introduction to the dynamic process of vision. In: Gentile M, ed. Functional visual behavior: a therapist’s guide to evaluation and treatment options. Bethesada (MD): American Occupational Therapy Association; 1997:3–39
- Gentile M. Functional visual behavior in adults: an occupational therapy guide to evaluation and treatment options. Bethesada (MD): American Occupational Therapy Association; 2005
- Gentile M. Functional visual behavior in children: an occupational therapy guide to evaluation and treatment options. Bethesada (MD): American Occupational Therapy Association; 2005
- Warren M, Barstow E. Occupational therapy interventions for adults with low vision. Bethesada (MD): American Occupational Therapy Association; 2011
- Singleton C, Henderson LM. Computerized screening for visual stress in children with dyslexia. Dyslexia 2007;13:130–51
- Irlen H. Reading by the colors. New York: Berkeley; 2005
- Wilkins AJ. Visual stress. Oxford, UK: OUP; 2005
- British Dyslexia Association. British dyslexia association: eyes and dyslexia. Available from: http://www.bdadyslexia.org.uk/about-dyslexia/further-information/eyes-and-dyslexia.html [last accessed 22 Feb 2012]
- Wilkins AJ. Reading through colour. Chichester: John Wiley and Sons; 2003
- Meares O. Figure/ground brightness contrast and reading disabilities. Visible Language 1980;14:13–29
- Birnbaum MH. Behavioral optometry: a historical perspective. J Am Optom Assoc 1994;65:225–64
- Northway N. Good schools guide: visual stress. Available from: http://www.goodschoolsguide.co.uk/help-and-advice/special-needs-advice/types-of-sen/sensory-difficulties/201/visual-stress [last accessed 1 Dec 2012]
- Fowler MS, Mason AJ, Richardson A, Stein JF. Yellow spectacles to improve vision in children with binocular amblyopia. Lancet 1991;338:1109–10
- Stein J, Walsh V. To see but not to read; the magnocellular theory of dyslexia. Trends-Neurosci 1997;20:147–52
- Ray NJ, Fowler S, Stein JF. Yellow filters can improve magnocellular function: motion sensitivity, convergence, accommodation, and reading. Ann N Y Acad Sci 2005;1039:283–93
- Harris D. Paper presentation. The City Univerity Course on Specific Learning difficulties. London: City University; 2002
- Wilkins AJ, Evans BJ, Brown JA, et al. Double-masked placebo-controlled trial of precision spectral filters in children who use coloured overlays. Ophthalmic Physiol Opt 1994;14:365–70
- Castillo R, Hilkey J. Assistive technology for individuals with learning disabilities. Am Occup Ther Assoc CEU 2004;1–8
- LoPresti EF, Mihalidis A, Kirsch N. Assistive technology for cognitive rehabilitation: state of the art. Neuropsycholog Rehabil 2004;14:5–39
- Irlen. Irlen syndrome treatment. Available from: http://www.irlenuk.com [last accessed 22 Feb 2012]
- Wilkins AJ, Nimmo-Smith I, Jansons JE. Colorimeter for the intuitive manipulation of hue and saturation and its role in the study of perceptual distortion. Ophthalmic Physiol Opt 1992;12:381–5
- MRC Intuitive Filters: intuitive colorimetry. Available from: http://www.ceriumoptical.com/vistech.aspx [last accessed 22 Feb 2012]
- Dyslexia Research Trust: about us. Available from: http://www.dyslexic.org.uk [last accessed 22 Feb 2012]
- Cantor and Nissel ChromaGen. Available from: http://www.dyslexia-help.co.uk [last accessed 22 Feb 2012]
- Harris Foundation. Available from: http://www.harrisdyslexia.com [last accessed 22 Feb 2012]
- Handler SM, Fierson WM, the Section on Ophthalmology and, Council on Children with Disabilities, American Academy of Ophthalmology, American Association for Pediatric Ophthalmology and Strabismus, American Association of Certified Orthoptists. Learning disabilities, dyslexia, and vision. Pediatrics 2011;127:818–56
- Tointon K. A very nice Essex girl goes bad. The Observer 29/1/2011 p.3
- Mitchell C, Mansfield D, Rautenbach S. Coloured filters and reading accuracy, comprehension and rate: a placebo-controlled study. Percept Mot Skills 2008;106:517–32
- Robinson GL, Foreman PJ. Scotopic sensitivity/Irlen syndrome and the use of coloured filters: a long-term placebo controlled and masked study of reading achievement and perception of ability. Percept Mot Skills 1999;89:83–113
- Bouldoukian J, Wilkins AJ, Evans BJ. Randomised controlled trial of the effect of coloured overlays on the rate of reading of people with specific learning difficulties. Ophthalmic Physiol Opt 2002;22:55–60
- Harris D, MacRow-Hill S. Interim report on the use of the ChromaGen contact lenses in patients with specific learning difficulties. Optometry Today 1998;38:15--17
- Harris D, MacRow-Hill SJ. Application of ChromaGen haploscopic lenses to patients with dyslexia: a double-masked, placebo-controlled trial. J Am Optom Assoc 1999;70:629–40
- Menaker SJ, Breton ME, Breton MI, et al. Do tinted lenses improve the reading performance of dyslexic children. A cohort study. Arch Opthalmol 1993;111:213–18
- Christeson GK, Griffin JR, Taylor M. Failure of blue-tinted lenses to change reading scores of dyslexic individuals. Optometry 2001;72:627–33
- Evans BJW. Dyslexia and vision. London: Whurr; 2001
- Haag-Street UK Ltd. Opthalmic Catalogue 2009;52. Available from: www.ootech.nl/images/uploads/1458_hs_catalogue.pdf [last accessed 25 Jan 2013]
- Castles A, Coltheart M. Varieties of developmental dyslexia. Cognition 1993;47:149–80
- Thompson ME. The effects of specialised teaching on dyslexic children. Appl Cogn Psychol 1988;2:19–31
- Stein JF. The magnocellular theory of developmental dyslexia. Dyslexia 2001;7:12–36
- Stein J, Fowler S. Treatment of visual problems in children with reading difficulties. Patoss Bulletin May 2005;15–22
- Vidyasagar TR. Attentional gating in primary visual cortex: a physiological basis for dyslexia. Perception 2005;34:903–11
- Cestnick L, Coltheart M. The relationship between language-processing and visual-processing deficits in developmental dyslexia. Cognition 1999;71:231–55