
ABSTRACT
Purpose: Evidence shows that effective self-management behaviors have the potential to improve health outcomes, quality of life, self-efficacy and reduce morbidity, emergency visits and costs of care. A better understanding of self-management interventions (i.e. programs that help with managing symptoms, treatment, physical and psychological consequences) is needed to achieve a positive impact on health because most children with a disability now live well into adulthood. Method: A systematic review of self-management interventions for school age youth with physical disabilities was undertaken to assess their effectiveness. Comprehensive electronic searches using international web-based reference libraries were conducted for peer-reviewed and gray literature published between 1980 and January 2012. Eligible studies examined the effectiveness of self-management interventions for children and youth between 6 and 18 years of age with congenital or acquired physical disabilities. Studies needed to include a comparison group (e.g. single group pre/post-test design) and at least one quantifiable health-related outcome. Results: Of the 2184 studies identified, six met the inclusion criteria; two involved youth with spina bifida and four with juvenile arthritis. The majority of the interventions ran several sessions for at least 3 months by a trained interventionist or clinician, had one-to-one sessions and meetings, homework activities and parental involvement. Although outcomes varied between the studies, all of the interventions reported at least one significant improvement in either overall self-management skills or a specific health behavior. Conclusions: While self-management interventions have the potential to improve health behaviors, there were relatively few rigorously designed studies identified. More studies are needed to document the outcomes of self-management interventions, especially their most effective characteristics for children and youth with physical disabilities.
There is some evidence to suggest that self-management interventions for children and youth with spina bifida and arthritis can improve self-management behaviors and health outcomes.
Parents’ involvement should be considered in encouraging self-management behaviors at different stages of their child’s development.
Much work is needed to explore the longer term implications of self-management interventions for youth with physical disabilities as well as the impact on health care utilization.
Implications for Rehabilitation
Introduction
With the prevalence of chronic conditions in childhood and reduced mortality rates [Citation1–4] there is an increasing need for young people to learn how to effectively manage their health condition [Citation5,Citation6]. Recent estimates indicate a doubling of the rate of chronic conditions among children and youth within the past two decades where approximately 15–20% of children have a chronic condition (i.e. lasting more than 3 months) [Citation7,Citation8] and over 200 000 Canadian and approximately 450 000 American children have an associated physical disability [Citation9,Citation10]. Childhood disability can negatively influence quality of life because disease courses are often unpredictable and many children’s symptoms result in social and physical restrictions [Citation8,Citation11]. Given that most children with a disability now live well into adulthood, a better understanding of the potential of self-management interventions is needed. Reducing the risk of secondary conditions and morbidity [Citation8] while increasing self-efficacy [Citation12] should improve the likelihood that young people will function independently throughout their lifespan [Citation13,Citation14].
Self-managing a health condition refers to an individual’s “ability to manage the symptoms, treatment, physical and psychological consequences and lifestyle changes inherent in living with a chronic illness” [Citation15]. Chronic condition self-management interventions emphasize the role of patient education in preventive and therapeutic health care activities [Citation15–20]. Typically, they involve organized learning experiences (e.g. information-based education or behavioral strategies) to facilitate the adoption of health promoting behaviors [Citation15,Citation21,Citation22]. Chronic disease self-management programs are based on the premise that people with chronic conditions share many commonalities in managing their condition including medication adherence, pain management, dealing with fatigue, stress, depression, healthy eating, exercise, self-efficacy and mobilizing social support [Citation18,Citation19]. Evidence from systematic reviews of the effectiveness of self-management shows that adult interventions can augment medical treatments, improve health outcomes, quality of life, self-efficacy and reduce morbidity, emergency visits and costs of care for those with obstructive pulmonary disease, asthma, diabetes, epilepsy, heart failure and other chronic conditions [Citation15,Citation19,Citation23–27].
While much can be gleaned from this evidence, most adult self-management interventions do not address the issues associated with life-long self-management for physical disabilities or chronic illnesses diagnosed in childhood [Citation28] or the impact of developmental stages on self-care abilities [Citation21].
Special consideration of the unique needs of children and youth’s self-management behaviors is critical. Children and youth experience multiple periods of significant developmental, emotional, social, physical and cognitive changes [Citation29] and major life-related transitions [Citation5,Citation6]. Unlike adults, the responsibility for self-management must be negotiated with parents and health care professionals who are ultimately responsible for a child’s health and well-being. According to the shared management model [Citation30,Citation31], as children mature they should increasingly take on developmentally appropriate responsibility for self-management. This responsibility transfer is especially important since health care services have largely shifted from institutions to homes [Citation2,Citation30,Citation32,Citation33] placing greater burden on children and their parents to manage complex treatment regimens. Negative health-related outcomes associated with poor health care transition to adult services further demonstrate the need for well-established self-management skills prior to adulthood [Citation34–36]. While children and youth are expected to assume greater responsibility for the self-management of their conditions [Citation34–37], their disease awareness and adherence to disease management activities are often less than optimal [Citation11]. This is a significant problem because inappropriate or inadequate self-management behaviors may reduce the benefits of treatment and positive health outcomes and increase the risk of secondary health outcomes [Citation7,Citation38]. Thus an early intervention approach is justified.
Evidence accrued from systematic reviews of the effects of self-management education programs based on a child-centered model similarly demonstrates improved health knowledge, increased self-management behaviors, and reduced hospitalization and emergency visits for children with diabetes [Citation39–44], asthma [Citation45–50] and chronic conditions broadly [Citation51,Citation52]. Overall, these reviews reflect the preponderance of adult self-management evidence [Citation38,Citation53–56] and disproportionately represent a very narrow range of pediatric chronic conditions.
There are several notable gaps in existing systematic reviews exploring the influence of self-management interventions on children’s health behaviors. First, most syntheses on children’s self-management interventions have focused on a specific chronic disease (e.g. diabetes, asthma and cystic fibrosis) while there has been no synthesis of other important long-term conditions especially physical disability (e.g. spina bifida, cerebral palsy, muscular dystrophy, mobility disorders, spinal cord injury, congenital disorder) [Citation57–60]. Although the literature on self-management among children with physical disabilities has been growing, there have been few efforts to synthesize the knowledge of common self-management strategies (i.e. what works and for whom). This systematic review aims to answer the following questions: (i) how do self-management programs for children and youth with physical disabilities influence health behaviors? and (ii) what are the common components of effective self-management interventions for children and youth with physical disabilities?
Methods
A systematic review was undertaken to critically appraise the evidence of self-management interventions for children and youth with physical disabilities and provide an unbiased summary of current best practice. Guidelines outlined in the Preferred Reporting Items for Systematic reviews and Meta-analyses statement were followed to ensure transparent and complete reporting [Citation61,Citation62].
Search strategy and data sources
The search strategy and database selection was developed through consultation with, and facilitated by, an experienced health research librarian and a specially constituted knowledge user Advisory Group, comprising pediatric rehabilitation professionals, parents and youth with physical disabilities. A series of electronic searches for peer-reviewed published and gray literature were conducted using major health-related databases MEDLINE (OVID) including “in process” and other “non-indexed citations”, Healthstar (OVID), CINAHL, EMBASE, Cochrane database, Cochrane Central Register of Controlled Trials (CENTRAL), PsycInfo, Science Citation Index, Scopus, Google scholar, GreyNet and conference proceedings (Conference Papers Index, BIOSIS, Dissertations/Theses). We also searched other Canadian and US information repositories, disability and health organization web sites, and specific children’s health care institution web sites. Reference lists from all identified appropriate papers were examined and hand searched for additional relevant studies.
Previously published condition-specific systematic reviews and meta-analyses [Citation39,Citation42,Citation45] were used to guide the development of the search strategy and identify pertinent publications. Self-management was defined as “an individual’s ability to manage the symptoms, treatment, physical and psychological consequences and lifestyle changes inherent in living with a chronic illness” [Citation15]. The subject headings and MeSH terms included terms related to self-management including “self-management”, “selfcare”, “disease manage*”, “disab*”, “physical disability” (including a broad list of common pediatric disabilities related to impairments in body structure and function [Citation63]: cerebral palsy, spina bifida, spinal cord injury, congenital disorder, mobility disorder, amputation, cerebral vascular accident/stroke, congenital anomalies, hydrocephalus, juvenile arthritis, muscular dystrophy, developmental co-ordination disorder and orthopedic conditions (scoliosis). This list was reviewed for relevance by a pediatrician with expert knowledge in childhood disabilities); and “intervention” as well as “health education”, “health knowledge” and “self-help techniques. Minor modifications to the search strategy were made as required within individual databases.
Study selection
To be included in the review articles needed to have: (1) at least 50% of sample with a physical disability, defined as a physical functional limitation (in instances where samples may have a variety of chronic conditions); (2) school-age children and youth with the majority of the sample or average age between 6 and 18 years of age; (3) an intentional, structured self-management intervention for youth, or parents and youth; (4) a statistically evaluated quantifiable health outcome; (5) levels I–III of American Academy of Neurology’s (AAN) classification of evidence for therapeutic intervention (where class I refers to rigorous randomized controlled trials (RCTs), class II refers to matched prospective cohort studies or RCTs in a representative population lacking one of the criteria in class I and class III all other controlled trials) [Citation64]; (6) a sample size greater than or equal to 5 and (7) published article or gray literature between 1980 and January 2012. There were no language restrictions. Exclusion criteria involved: (1) exclusive reports on satisfaction about health care services; (2) focus on preschool age children or adults; (3) focus on diabetes, asthma or cystic fibrosis (because reviews already exist on these particular conditions and they are not covered in our definition of physical disability); (4) opinion articles; (5) sample size less than 5 and (6) other chronic conditions that are not considered to be a physical disability.
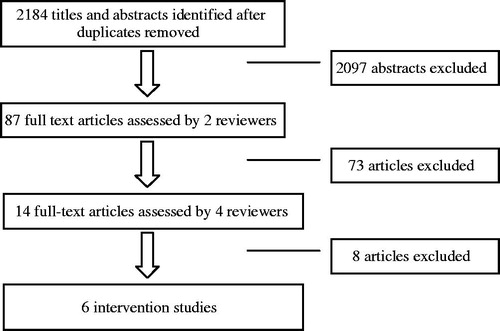
Retrieved records were imported into RefWorks©. The search process identified 2184 studies whereby two people independently reviewed the titles and abstracts of these articles (). Most of the articles (2097) were eliminated based on title or abstract not being related to the search. Seventy-three potentially relevant studies were independently reviewed in full by two investigators (the first author and a research assistant). After applying the inclusion criteria and removing the duplicates, 14 remained, which were read by four members of the research team. After careful consideration of the inclusion criteria and discussion amongst the research team, six articles remained in the final analysis.
Figure 1. Flow of studies through the systematic review process.
Data abstraction and synthesis
Data from included studies were extracted and compiled, and independently verified using a structured abstraction form, developed based on previously completed systematic reviews in the area of self-management [Citation20,Citation24,Citation25,Citation45]. As part of an audit trail, a journal was maintained to bring forward key points; discrepancies were resolved through discussion. Because of heterogeneity in the study populations, interventions used and outcome measures applied, it was neither feasible nor appropriate to conduct a meta-analysis. Findings were synthesized according to the guidelines for narrative synthesis [Citation65]. As part of a structured interrogation and summary, studies were organized into logical categories (aided by our data abstraction form and informed by our self-management knowledge user Advisory Group) to guide the analysis ( and ). A list of key components of interventions was developed and a constant comparison method was used to facilitate the analysis. After the initial analysis was complete, all authors reviewed common elements of the interventions and minor adjustments were made until consensus was reached. Applying this method is consistent with the use of varied data from diverse methodologies [Citation66]. Our analysis and conclusions regarding the effectiveness of self-management programs were based on the extracted data and involved discussion and consensus amongst the research team.
Table 1. Characteristics and overview of studies.
Table 2. Results of studies.
Studies were classified according to the AAN classification of evidence for therapeutic intervention [Citation64] independently by two investigators. Recommendations for the effectiveness of interventions to improve self-management behaviors were based on the overall strength of the evidence.
Results
The key characteristics and findings from each study are outlined in . First, we provide an overview of the study descriptions and characteristics of each intervention. Next, we outline the effectiveness of interventions followed by the common components of each intervention.
Study descriptions
Two of the studies had samples of adolescents with spina bifida [Citation67,Citation68], two had juvenile rheumatoid arthritis (JRA) and two had juvenile idiopathic arthritis (JIA) [Citation69–72]. Four of the studies were conducted in the US, one in the UK and one in Canada. Four studies were published in peer-reviewed journals [Citation69–72] while two studies were gray literature [Citation67,Citation68]. Two of the studies [Citation69,Citation71] used an RCT design while the remaining four used a before and after design [Citation67,Citation68,Citation70,Citation72]. Sample sizes ranged from 10 to 308 and the ages of the samples ranged from 2 to 18. In four studies, the majority of the sample was Caucasian and female while the remainder studies did not specify.
Characteristics of interventions
The interventions varied greatly in content and delivery (). Greenley [Citation67] explored the feasibility and acceptability of an individualized family self-management, hospital-based intervention for youth with spina bifida. Key components of the program involved providing education about spina bifida, teaching problem solving skills, homework and goal setting. Their intervention was conducted in two 60–90 min sessions over the span of 3 months.
A second hospital-based self-management intervention focused on self-management of youth with JRA. Lavigne et al. [Citation70] explored the utility of a psychological treatment for youth with high levels of pain related to JRA. Their standardized self-management intervention, which took place over the course of six, 60–90 min sessions, included muscle relaxation (taught to both the parent and child), relaxation training, biofeedback and homework.
McDonagh and Southwood Shaw [Citation72] conducted their intervention with youth with JIA in 10 pediatric rheumatology centers to determine whether quality of life could be improved. Their intervention included transition plans and developmentally appropriate informational resources for each youth and parent to reflect on the development and components of the transition program in terms of health, home and school. It involved a minimum of three sessions over the course of 12 months. The intervention was standardized but elements were adapted to youth/family situations.
O’Mahar’s [Citation68] self-management intervention for youth with spina bifida aimed to evaluate its impact on youth’s autonomy. Their intervention involved standardized components such as psycho-education training including group discussion and role-play, as well as individualized elements such as goal setting, coaching and other activities related to self-managing their condition. This intervention took place over the course of one week in a summer camp environment. The psycho-educational sessions were held daily (five days) for 90 min. Parents were involved in pre-camp goal setting and were given brief handouts at the start and end of camp.
Rapoff’s et al. [Citation71] intervention, run out of a medical centre, aimed to prevent an anticipated drop in medication adherence among newly diagnosed patients with JRA. The standardized intervention involved one 30-min session and 14 phone calls over the course of 12 months. Key components of the intervention included educational and behavioral strategies for enhancing adherence for both youth and parents (disease information, monitoring, positive reinforcement and discipline).
Stinson et al.’s [Citation69] Teens taking charge program examined the feasibility of a 12-week Internet-based self-management program that was developed by a pediatric center. There were 12 modules for youth that took approximately 20–30 min to complete. Modules included topics such as: learning about different types of arthritis, diagnosis, medications, managing symptoms, managing stress, relaxation, distraction, self-monitoring and supports and transitional issues. A trained coach provided weekly telephone support. There were two modules for parents.
Components of the interventions
Although the interventions varied in length, duration and number of sessions all of the self-management interventions involved multiple components over several sessions. The number and length of sessions varied across the studies. One intervention took place under less than one week [Citation68], three of the studies lasted 3 months [Citation67,Citation69,Citation70] and two of the studies ran for 12 months [Citation71,Citation72]. The number and length of sessions varied, ranging from one, 30-min face-to-face session [Citation71] to six, 90-min sessions [Citation70].
Four studies were conducted in a pediatric hospital or medical clinic [Citation67,Citation70–72], one at a summer camp [Citation68] and one online [Citation69] (). In regard to delivery of the program, three involved a trained interventionist [Citation67–69], two were clinician-led [Citation70,Citation71] and one by a program co-ordinator [Citation72]. Two interventions had telephone support for participants [Citation69,Citation71].
Table 3. Intervention components.
Five of the interventions offered one-to-one sessions while one intervention [Citation68] offered a group format. Five out of the six interventions involved meetings [Citation67,Citation68,Citation70–72]. Two of the interventions involved phone contact and support [Citation69,Citation71]. All of the interventions involved parents in some capacity. One online study had specific modules for parents [Citation69]; in four studies the parents were asked to complete the sessions together with the youth [Citation67,Citation70–72] while in O’Mahar’s study [Citation68] the parents were asked to participate in goal setting (pre-camp) and outcome evaluation (post-camp). Five of the interventions included a clearly described practice component (i.e. homework) [Citation67–71].
All of the interventions addressed medical management tasks such as symptom management. Three interventions included education and discussion of life roles (e.g. school, work, relationships) [Citation68,Citation69,Citation72]. Only one study included elements related to management of emotions that might be associated with living with a disability [Citation69]. Two interventions [Citation67,Citation68] educated youth about skills that are associated with successful self-management such as problem-solving and goal-setting.
Four of the studies were based on a theoretical model. For example, Greenley [Citation67] used a problem solving approach to build self-management skills. Lavigne et al.’s [Citation70] model involved a biofeedback and cognitive behavior training, while O’Mahar [Citation68] had an empowerment perspective. Finally, Rapoff et al. [Citation71] used an applied behavior analytic theory to inform their model. Although it is important to have theoretically informed interventions, we did not notice any differences in outcomes for the interventions that had a theoretically driven model and those that did not.
Effectiveness of the interventions
The outcome measures varied across the studies () and included self-management behaviors, mastery of self-care tasks, self-reported pain, health-related quality of life, independent health behaviors, disease activity and functional status, adherence to medication and disease-related knowledge. Secondary measures included: social goals, parent’s beliefs in youth readiness, sharing responsibility for health, satisfaction with the intervention and self-concept.
All of the studies found at least one positive effect on health behaviors. Outcomes included: a decrease in perceived family stress associated with condition management [Citation67]; improved medication adherence [Citation71]; decreased pain [Citation69,Citation70]; increased juvenile arthritis quality of life (parents and youth) [Citation72]; higher levels of disease knowledge [Citation68,Citation69,Citation72] and sharing responsibility of spina bifida management [Citation68].
It is important to note that there were several outcomes that were explored but were not significant. These included: youth self-management and parent/youth beliefs of readiness for future roles [Citation67]; youth responsibility for medications and independent attendance at consultation visits [Citation72]; health-related quality of life, perceived stress, self-efficacy [Citation69]; self-concept and depressive symptoms [Citation68]. Rapoff et al. [Citation71] also looked for an impact of improved medication adherence on disease activity and functional status but found no significant effects.
In terms of the rigor of these interventions, only two studies had control groups with an RCT design and had a level I on the quality rating () [Citation69 Citation71]. The remainder of the studies had a level III quality rating.
Discussion
This study critically appraised the research evidence on the effectiveness of self-management interventions for youth with physical disabilities. Over a 30-year period, only six empirical studies of distinct programs for self-management interventions for children and youth with physical disabilities were identified. Our review demonstrates possible evidence that self-management interventions are effective at influencing health knowledge and behaviors for youth with spina bifida and arthritis. While each of the studies assessed a self-management intervention, the details of the interventions and the outcome measures used differed widely. Findings of significant effects also varied. Although all of the interventions reported at least one significant improvement in either overall self-management skills or a specific health behavior (e.g. adherence to treatment, improved self-reported pain), non-significant findings were noted. Given that a meta-analysis was not feasible, these significant findings should be treated with caution.
Broad reviews of health conditions have found moderate to strong evidence for their effectiveness [Citation73,Citation74]. For example, past systematic reviews on self-management interventions for youth with chronic conditions (i.e. diabetes, asthma, cystic fibrosis) have found moderate effectiveness (i.e. not all outcomes were positive). Evidence of the effects of self-management education programs based on a child-centered model for children with diabetes and asthma demonstrate improved health knowledge, increased self-management behaviors, and reduced hospitalization and emergency visits for children with diabetes [Citation41–46]. Similarly educational self-management asthma interventions for children and adolescents have been found to improve lung function and feelings of self-control, reduce absenteeism from school and number of visits to an emergency department [Citation51]. Others report that there is limited evidence that self-management education can positively influence health behaviors among youth [Citation75]. A systematic review of asthma interventions for children found limited evidence to suggest that interventions currently available are effective for significantly improving health-related quality of life amongst asthmatic children, adolescents and their families [Citation76]. The mixed findings could be a result of the variety of outcome measures that are used, and components of the various interventions, as was the case in this review.
Although there was no single consistent self-management strategy that improved health outcomes, the following components of self-management interventions were common amongst the majority of included studies: they ran several sessions for at least 3 months led by a trained interventionist or clinician, had one-to-one sessions with face-to-face meetings, homework activities and parental involvement. These components are consistent with previous research on youth showing that issues such as knowledge about their condition, medication adherence, psycho-social factors (e.g. self-efficacy) and parental involvement (shared management) are important components in maintaining health [Citation5,Citation6,Citation30,Citation32]. However, evidence shows that parental involvement can be a potential stressor or barrier to self-managing a chronic condition [Citation6]. Interestingly, none of the articles examined readiness to take ownership for their own care or the extent to which parents were involved. Future research should carefully examine the role that parents play in a shared management model and/or how they encourage independence in their child.
Beyond client- and family-based outcomes, none of the studies examined health care utilization or cost-effectiveness of the interventions. These are two outcomes commonly explored in self-management programs. This is an important area to consider because many countries encourage patients to actively self-manage their condition in the hopes that it will not only help to improve individual health and well-being but help reduce health costs [Citation77]. More research is needed to explore this area further amongst children and youth with physical disabilities.
Within the small number of empirical studies identified, it was disconcerting to note that there was little variation in participant demographics with samples mainly drawing on Caucasian females. Very little is known about socio-economic status, race, ethnicity, geographic location, level of severity of disease, presence of co-morbidities and duration of disease. These are all important factors that can influence the ability and motivation to self-manage a chronic condition [Citation38]. A common criticism of self-management interventions is that they tend to have a “one size fits all” approach [Citation78] and neglect to reach those who could arguably benefit most from the program (such as those from lower socio-economic backgrounds and members of ethnic minority groups) [Citation77,Citation79,Citation80]. Past evidence with adults has shown that self-management of chronic illness is strongly linked with social class where those with higher incomes often have a better locus of control and are more actively involved in the care of their illness [Citation38,Citation80]. Of potentially greater concern is the finding that only two physical disability groups were represented. For example, our review did not find a self-management intervention for cerebral palsy, which is a huge gap in the literature given its prevalence. Effective self-management is a crucial life skill with significant implications for a young person’s capacity to achieve their life goals.
The objective of this review was to identify empirical studies examining the effectiveness of self-management interventions for school-age children and youth with physical disabilities. We are confident through the engagement of key stakeholders, comprehensive search strategy inclusive of published and gray literature, independent screening and rigorous data extraction processes that we have identified the studies meeting the outlined criteria. Despite these efforts, the lack of available evidence and heterogeneity of the studies identified makes it difficult to compare and contrast the effective components of programs. A limitation of this study is that we focused on intentional self-management interventions and we may not have captured studies that focused on one specific aspect of improving children’s health (such as the benefits of stretching or yoga). However, our aim was to focus on the whole person and overall health and well-being.
Despite the potential of self-management interventions, the current findings suggest they are failing to reach those most in need, such as children [Citation38,Citation81]. Possible barriers to comprehensive disease education linked with self-management therapy include accessibility difficulties, limited availability of trained professionals, lack of social support, discrimination, financial constraints and lack of information and targeted educational interventions [Citation6,Citation7,Citation16,Citation82,Citation83]. The absence of policy-driven self-care and condition awareness promotion within pediatric health care is problematic because failure to make a smooth transition toward independent self-management can negatively influence health outcomes and meaningful participation in life domains [Citation35]. Much work is needed to address the current gap in empirical literature to inform evidence-based self-management interventions for young people with physical disabilities.
Conclusion
In conclusion, there was limited high-quality evidence of self-management interventions designed for youth with physical disabilities to suggest that self-management interventions have potential for improving self-management knowledge and health behaviors among youth. Clinicians, youth and families should be cautious when considering applying any of these particular self-management strategies. Further interventions using rigorous methods are recommended.
There are several directions for further research. First, more research using rigorous designs is needed to evaluate the effectiveness of self-management interventions on health behaviors of youth with physical disabilities. Second, more research is needed to compare different lengths, formats and types of interventions, delivery formats and contexts. Further examination of what works (i.e. self-determination strategies and medication management) best for whom (e.g. socio-demographic characteristics, particularly more effort to involve males and a variety of ethno-cultural groups), and in what context is needed. Exploring the social, contextual and environmental factors that influence a person’s ability to manage their condition would be beneficial. Third, more exploration of the cost-effectiveness of different methods of delivery of self-management interventions would be worthwhile. Fourth, more consistent use of standardized measures would be beneficial to compare interventions. Fifth, further work is needed to explore the longer term implications of such interventions as well as the impact on health care utilization.
Declaration of interest
This research was funded by the Canadian Institutes for Health Research.
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of this article.
Acknowledgements
We would like to thank Diane Savage, C.J. Curran, Pui Ying Wong, Meghann Proulx, Leila Amin and the members of the Self-Management Advisory Group for their guidance throughout this project.
References
- American Academy of Pediatrics. A consensus statement on health care transitions for young adults with special health care needs. Pediatrics 2002;110:1304–36
- Strauss D, Shavelle R, Anderson T. Long-term survival of children and adolescents after traumatic brain injury. Arch Phys Med Rehabil 1998;79:1095–110
- Strauss D, Brook J, Rosenbloom L, Shavelle R. Life expectancy in cerebral palsy: an update. Dev Med Child Neurol 2008;50:487–93
- Newacheck P, McManus M, Fox H, et al. Access to health care for children with special health care needs. Pediatrics 2000;105:760–6
- Kingsnorth S, Healy H, Macarthur C. Preparing for adulthood: a systematic review of life skill programs for youth with disabilities. J Adoles Health 2007;41:323–32
- Lindsay S, Kingsnorth S, Hamdani Y. Barriers and facilitators of chronic illness self-management among adolescents: a review and future directions. J Nurs Chronic Illness Health Care 2011;3:186–208
- Stinson J, Wilson R, Gill N, et al. A systematic review of internet-based self-management interventions for youth with health conditions. J Pediatr Psychol 2009;34:495–510
- Newacheck P, Strickland B, Shonkoff J, et al. An epidemiologic profile of children with special health care needs. Pediatrics 1998;102:117–23
- Statistics Canada. 2008 Participation and activity limitation survey. Ottawa
- Government Census [Internet]. Disability Status 2000 Census Brief 2003. Available from: www.census.gov/prod/2003pubs/c2kb-17.pdf [last accessed 5 Sep 2012]
- Yeo M, Sawyer S. Chronic illness and disability. Br Med J 2005;330:721–3
- Sawin K, Bellin M, Roux G, et al. The experience of self-management in adolescent women with spina bifida. Rehabil Nurs 2009;34:26–38
- King G, Baldwin P, Currie M, Evans J. Planning successful transitions from school to adult roles for youth with disabilities. Child Health Care 2005;34:193–216
- Law M, Petrenchik T. Participation of children with complex needs. In Final report for the Ontario Ministry of Children and Youth Services; 2005
- Barlow J, Wright C, Sheasby J, et al. Self-management for people with chronic conditions: a review. Patient Educ Counsel 2002;48:177–87
- Barlow J, Ellard D. Psycho-educational interventions for children with chronic disease, parents and siblings: an overview of the research evidence base. Child: Care Health Dev 2004;30:637–45
- Fredericks E, Dore-Stites D. Adherence to immonosuppressants: how can it be improved in adolescent organ transplant recipients? Curr Opin in Organ Transplant 2010;15:614–20
- Lorig K, Ritter P, Stewart A, et al. Chronic disease self-management program: 2-year health status and health utilization outcomes. Medical Care 2001;39:1217–23
- Lorig K, Ritter P, Laurent D, Plant K. Internet-based chronic disease self-management: a randomized trial. Med Care 2006;44:864–971
- Warsi A, Wang P, LaVelley M, et al. Self-management education programs in chronic disease: a systematic review and methodological critique of the literature. Arch Int Med 2004;164:1641–9
- Sawyer S, Aroni R. Self-management in adolescents with chronic illness. What does it mean and how can it be achieved? Med J Aust 2005;183:405–9
- Wagner E. Chronic disease management: what will it take to improve care for chronic illness. Effect Clin Pract 1998;1:2–4
- Drus B, Zhao L, von Esenwein S, et al. The health recovery peer (HARP) program for persons with serious mental illness. Schizophrenia Research 2010;118:264–70
- Du S, Yuan C. Evaluation of patient self-management outcomes in health care: a systematic review. Int Nurs Rev 2010;57:159–67
- Marks R, Allegrante J. A review and synthesis of evidence for self-efficacy enhancing interventions for reducing chronic disability: implications for health education practice. Health Promot Pract 2005;6:148–56
- Murray E, Burns J, See T, et al. Interactive health communication applications for people with chronic disease. Cochrane Database Syst Rev 2005;4:1–25
- Shaw E, Stokes T, Camosso-Stefinovic J, et al. Self-management education for adults with epilepsy. Cochrane Database Syst Rev 2007;18:CD004723
- Giarelli Bernhardt, B, Mack R, Pyeritz RE. Adolescents’ transition to self-management of a chronic genetic disorder. Qual Health Res 2008;18:441–57
- Sawyer S, Drew S, Duncan R. Adolescents with chronic disease – the double whammy. Aust Fam Phys 2007;36:622–7
- Kieckhefer G, Trahms C. Supporting development of children with chronic conditions: from compliance towards shared management. Pediatr Nurs 2000;26:354–63
- Gall C, Kingsnorth S, Healy H. Growing up ready: a shared management approach to transition. Phys Occup Therapy Pediatr 2006;38:47–62
- Antle B, Mills W, Steele C, et al. An exploratory study of parents’ approaches to health promotion in families of adolescents with physical disability. Child: Care Health Dev 2008;34:185–93
- Knafl K, Deatrick J. The challenge of normalization for families of children with chronic conditions. Pediatric Nurs 2002;28:48--53
- Dashiff C, Morrison S, Rowe J. Fathers of children and adolescents with diabetes: what do we know? J Pediatr Nurs 2008;23:101–19
- Kingsnorth S, Lindsay S, Maxwell J, et al. Implementation of the LIFEspan Model of transition care across pediatric and adult rehabilitation providers. Int J Child Adoles Health 2011;3:547–60
- Laster N, Holsey C, Shendell D, et al. Barriers to asthma management among urban families: caregiver and child perspectives. J Asthma 2009;46:731–9
- Barlow J, Shaw K, Harrison, K. Consulting the ‘experts’: children’s and parents’ perceptions of psycho-educational interventions in the context of juvenile chronic arthritis. Health Educ Res 1999;14:597–610
- Lindsay S. How and why the motivation and skill to self-manage chronic disease are socially unequal. Res Sociol Health Care 2008;26:17–39
- Anderson B, Svoren B, Laffel L. Initiatives to promote effective self-care skills in children and adolescents with diabetes mellitus. Dis Manage Health Outcomes 2007;15:101–8
- Boren A, Gunlock T, Krishna S, Kramer T. Computer-aided diabetes education: a synthesis of randomized controlled trials. AMIA Annu Symp 2006;51–5
- DeShazo J, Harris L, Pratt W. Effective intervention or child’s play? A review of video games for diabetes education. Diabetes Technol Therap 2010;12:815–22
- McBroom L, Enriquez M. Review of family-centred interventions to enhance the health outcomes of children with type 1 diabetes. Diabetes Educator 2009;35:428–38
- Russell-Minda E, Jutai J, Speechley M, et al. Health technologies for monitoring and managing diabetes: a systematic review. J Diabetes Sci Technol 2009;3:1460–71
- Spencer J, Cooper H, Milton B. Qualitative studies of type 1 diabetes in adolescence: a systematic literature review. Pediatr Diabetes 2010;11:364–75
- Bravata D, Gienger A, Holty J, et al. Quality improvement strategies for children with asthma: a systematic review. Arch Pediatr Adoles Med 2009;163:572–81
- Coffman J, Cabana M, Yelin E. Do school-based asthma education programs improve self-management and health outcomes? Pediatrics 2009;124:729–42
- Ducharme F, Bhogal S. The role of written action plans in childhood asthma. Curr Opin Allergy Clin Immunol 2008;8:177–88
- Li P, Guttmann A. Recent innovations to improve asthma outcomes in vulnerable children. Curr Opin Pediatr 2009;21:783–8
- Loffman J, Cabana M, Halpin H, Yehn E. Effects of asthma education on children’s use of acute care services: a meta-analysis. Pediatrics 2008;121:575–86
- Portnoy J, Jennings D. Utilization patterns in an asthma intervention. Ann Allergy Asthma Immunol 2006;97:S25–30
- Guevara J, Wolf F, Grum CM, Clark N. Effects of educational interventions for self-management in children and adolescents: systematic review and meta-analysis. Br Med J 2003;326:1308–9
- Stokes T, Shaw E, Camosso-Stefinovic J, et al. Withdrawn: self-management education for children with epilepsy. Cochrane Database Syst Rev 2007;2:CD004724
- Stokes T, Saw E, Camosso-Stefinovic J, et al. Self-management education for children with epilepsy. Cochrane Database Syst Rev 2010;10:CD004724
- Bradley P, Lindsay B. Care delivery and self-management strategies for adults with epilepsy. Cochrane Database Syst Rev 2008;1:CD006244
- Effing T, Monninkhof E, van der Valk P, et al. Self-management education for patients with chronic obstructive pulmonary disease. Cochrane Database Syst Rev 2007;17:CD002990
- Gibson P, Powell H, Wilson A, et al. Self-management education and regular practitioner review for adults with asthma. Cochrane Database Syst Rev 2003;1:CD001117
- Downs J, Roberts C, Blackmore A, et al. Benefits of an education programme on the self-management of aerosol and airway clearance treatments of children with cystic fibrosis. Chronic Res Dis 2006;3:19–27
- Hommel K, Odell S, Sander E, et al. Treatment adherence in pediatric inflammatory bowel disease: perceptions from adolescent patients and their families. Health Social Care Community 2011;19:80–8
- Stenekes S, Hughes A, Gregoire M, et al. Frequency and self-management of pain, dyspnea and cough in cystic fibrosis. J Pain Sympt Manage 2009;38:837–48
- Stinson J, Toomey P, Stevens B, et al. Asking the experts: exploring the self-management needs of adolescents with arthritis. Arthritis Rheumatol 2008;59:65–72
- Moher D, Liberati A, Tetzlaff J, Altman DG. The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA Statement. PloSMed 2008;6:e1000097
- Liberati A, Alman D, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. PloS Med 2009;6:e1000100
- World Health Organization. Towards a common language for functioning, disability, and health: ICF. Geneva, Switzerland: World Health Organization; 2001
- Edlund W, Gronseth G, So Y, Franklin G. Clinical practice guidelines process manual. St. Paul: American Academy of Neurology; 2004
- Petticrew M, Roberts H. Systematic reviews in social sciences: a practical guide. Victoria, Australia: Wiley Blackwell; 2005
- Whttemore R, Knafl K. The integrative review: updated methodology. J Adv Nurs 2005;52:546–53
- Greenley R. A family program to encourage independence in children with spina bifida. Presentation to the spina bifida Association; 2006
- O’Mahar K. A camp intervention targeting independence issues among children, adolescents and young adults. ProQuest Dissertations and Theses. Loyala University Chicago; 2009
- Stinson J, McGrath P, Hodnett E, et al. An internet-based self-management program with telephone support for adolescents with arthritis: a pilot randomized controlled trial. J Rheumatol 2010;37:1944–52
- Lavigne J, Ross C, Berry S, et al. Evaluation of a psychological package for treating pain in juvenile rheumatoid arthritis. JRA Treat 1992;5:101–10
- Rapoff M, Belmont J, Lindsley C, et al. Prevention of nonadherence to non-steroidal anti-inflammatory medications for newly diagnosed patients with juvenile rheumatoid arthritis. Health Psychol 1992;21:620–3
- McDonagh J, Southwood Shaw K. The impact of a coordinated transitional care programme on adolescents with juvenile idiopathic arthritis. Rheumatology 2007;46:161–8
- Bauman L, Drotar D, Leventhal J, et al. A review of psychosocial interventions for children with chronic health conditions. Pediatrics 1997;100:244–51
- Kibby M, Tyc V, Mulhern R. Effectiveness of psychological interventions for children and adolescents with chronic illness: a meta-analysis. Clin Psychol Rev 1998;18:103–17
- Savage E, Beirne P, Ni Chroinin M, et al. Self-management education for cystic fibrosis. Cochrane Database Syst Rev 2011;7:CD007641
- Clarke S, Calam R. The effectiveness of psychosocial interventions designed to improve health-related quality of life amongst asthmatic children and their families: a systematic review. Qual Life Res 2012;21:747–64
- Lindsay S, Vrijhoef H. A sociological focus on “expert patients”. Health Soc Rev 2009;18:139–44
- Kendall E, Rogers A. Extinguishing the social? State sponsored self-care policy and the chronic disease self-management program. Disabil Soc 2007;22:129–43
- Greenlaugh T. Chronic illness: beyond the expert patient. Br Med J 2009;338:629–31
- Lindsay S. The influence of childhood poverty on the self-management of chronic disease in later life. Res Sociol Health Care 2009;27:161–83
- Hanvey L. Children and youth with special needs: summary report of findings. Ottawa: Canadian Council on Social Development; 2001
- Jerant A, von Friederichs-Fitzwater, M, Moore M. Patients perceived barriers to active self-management of chronic conditions. Patient Educ Counsel 2006;57:300–7
- Nagelkerk J, Reick K, Meengs L. Perceived barriers and effective strategies to diabetes self-management. J Adv Nurs 2006;54:151–8