
Abstract
Patients on sick leave due to work-related stress often complain about impaired concentration and memory. However, it is undetermined how widespread these impairments are, and which cognitive domains are most long-term stress sensitive. Previous studies show inconsistent results and are difficult to synthesize. The primary aim of this study was to examine whether patients with work-related stress complaints have cognitive impairments compared to a matched control group without stress. Our secondary aim was to examine whether the level of self-reported perceived stress is associated with neuropsychological test performance. We used a broad neuropsychological test battery to assess 59 outpatients with work-related stress complaints (without major depression) and 59 healthy controls. We matched the patients and controls pairwise by sex, age and educational level. Compared to controls, patients generally showed mildly reduced performance across all the measured domains of the neuropsychological test battery. However, only three comparisons reached statistical significance (p < 0.05). Effect sizes (Cohen's d) were generally small to medium. The most pronounced differences between patients and controls were seen on tests of prospective memory, speed and complex working memory. There were no statistical significant associations between self-reported perceived stress level and neuropsychological test performance. In conclusion, we recommend that cognitive functions should be considered when evaluating patients with work-related stress complaints, especially when given advice regarding return to work. Since this study had a cross-sectional design, it is still uncertain whether the impairments are permanent. Further study is required to establish causal links between work-related stress and cognitive deficits.
Introduction
Job demands of contemporary workers have changed dramatically during the past 30 years, going from being primarily physical to primarily cognitive. The modern workplace requires skills in communication, information processing, decision making and administering complex assignments (Kompier, Citation2006). Therefore, an efficient workplace requires that the workers have a high level of cognitive functioning.
Inspired by Lazarus & Folkman (Citation1984), this study defined work-related stress as a process in which an individual perceives the threats or demands associated with work as being more than the individual can handle, thereby negatively affecting the psychological and/or physiological state of the individual. The symptoms of work-related stress can include sleep difficulties, fatigue, tension, complaints of physical pain, anxiety and feelings of sadness. Chronic work-related stress can lead to conditions like depression, exhaustion disorder or burnout (Bonde, Citation2008; Grynderup et al., Citation2013; Hasselberg et al., Citation2014; Maslach et al., Citation2001; Yu et al., Citation2014). Often, individuals suffering from work-related stress also complain about cognitive impairments, including impaired concentration and memory skills. However, it remains uncertain whether these complaints mirror an actual reduction in cognitive functions (that can be measured by neuropsychological testing) or are entirely subjective perceptions. If individuals suffering from work-related stress indeed suffer from cognitive impairments, it would be important to consider this issue in evaluation and treatment.
To date, several researchers have used neuropsychological testing in an attempt to discover whether patients with chronic work-related stress have cognitive impairments that are objectively measurable (e.g. Jonsdottir et al., Citation2013; Österberg et al., Citation2009; Sandström et al., Citation2005; van Dam et al., Citation2011). The majority of these studies indicate that people with severe chronic stress, exhaustion disorder or burnout exhibit reduced performance on a number of neuropsychological tests covering multiple cognitive domains relative to healthy controls. However, the results are relatively inconsistent, perhaps due to low power and inadequate matching of patients and controls (as discussed by Österberg et al. (Citation2012)). In addition, most of the studies include patients with psychiatric disorders that are known to cause cognitive problems (such as major depression) (Austin et al., Citation2001), which may bias studies examining consequences of chronic stress.
The aim of this study was to examine whether a group of outpatients with perceived work-related stress without major depression have cognitive impairments relative to healthy control subjects. We intended to overcome the shortcomings of the previous studies by including a relatively large sample of patients without comorbid psychiatric disorders and by using a paired design with carefully matched healthy controls.
Our primary hypothesis in this study was that the patient group would perform worse on the comprehensive neuropsychological test battery compared to the control group. Our secondary hypothesis was that the level of perceived stress would be inversely related to neuropsychological test performance.
Methods
Participants
The participants in this study were outpatients referred by their general practitioner to the Department of Occupational Medicine, the Regional Hospital West Jutland, Denmark. The general practitioner refers a patient to the department if (s)he considers the mental health problems of the patient to be work-related, if the patient needs help to return to work and/or if the illness should be reported to the National Board of Industrial Injuries.
Before arrival at the Department of Occupational Medicine, all patients filled out a standard questionnaire, including the three subscales depression, anxiety and somatization from the Symptom Checklist (SCL-90-R) (Derogatis, Citation1977). Afterwards, an occupational psychologist interviewed the patients regarding work-related stressors, other kinds of stressors, previous mental history, symptom development, etc. In case of depressive symptomatology, the six-item Hamilton Depression Scale was used to rate the severity of depressive symptoms (Bech et al., Citation1975; Hamilton, Citation1960; Videbech et al., Citation2007).
Inclusion criteria were as follows:
Duration of stress symptoms at least one month.
The patient and the occupational psychologist both consider it likely that the mental health symptoms were a reaction primarily to work-related strain. However, other kinds of stressors could also be present (e.g. family conflicts).
Patient symptom severity correspond to a T-score of at least 63 on one or more of the SCL-90-R subscales – depression, anxiety and somatization. A T-score of 63 was recommended to identify a “case” in the Danish manual (Olsen et al., Citation2007).
The exclusion criteria were as follows:
Current or previous psychiatric disorder (within the past two years). However, mild depressive symptoms were allowed (defined as a score lower than 9 on the six-item Hamilton Depression Scale).
Physical illness causing cognitive impairment.
Alcohol or substance abuse.
Native language other than Danish.
Learning disabilities.
Psychoactive drug use other than contemporary antidepressants.
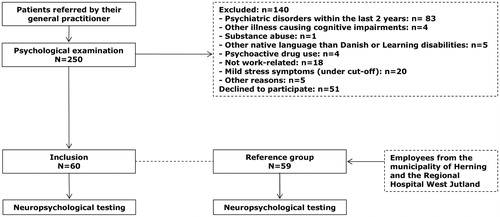
To match each patient, we recruited a healthy control subject. We matched the patients and controls pairwise on sex, age and educational level to eliminate the effects of possible confounding. The controls were employed at the Regional Hospital West Jutland or in the municipality of Herning. For each patient, we identified five potential controls, all of whom met the matching criteria, and sent out a letter with an offer to take part in this study. The controls did not receive any remuneration but had a chance of winning a gift voucher for a wellness stay. The first person who contacted the department was screened by the second author (an experienced clinical psychologist) with regard to the above-mentioned exclusion criteria. In addition, controls were excluded if they had a T-score of 60 or more (1 SD above the mean of the Danish population) on one or more of the SCL-90-R subscales (depression, anxiety or somatization). If the first person was excluded as a control, the next in line was screened. If not, a single person of the five potential controls responded, we sent out letters to five new individuals. The procedures of this study are illustrated in .
Figure 1. Flowchart of this study.
Materials
Self-report
After the participants were included and about one week before the neuropsychological testing, a link to a questionnaire was sent to their e-mail address. The questionnaires referred to the last month and encompassed the following scales.
Perceived stress was measured by the 10-item Perceived Stress Scale (PSS10) (Cohen et al., Citation1983). The PSS10 is a global stress measure developed to assess the extent to which individuals find their lives to be unpredictable, uncontrollable and overloaded. Each item was scored on a five-point scale ranging from 0 (never) to 4 (very often). The total score (range 0–40) was calculated as the sum of item scores after converting item 4, 5, 7 and 8, which were positive formulated questions.
Mental health complaints were measured by three subscales from the SCL-90-R, which contains 90 items and nine subscales measuring different facets of mental distress including somatization. Each item was scored on a five-point scale ranging from 0 (not at all distressed) to 4 (very much distressed). We used the three subscales measuring symptoms of anxiety, depression and somatization. The total scores (range 0–4) of each subscale were calculated as the mean of all the item scores. Normative data and findings supporting the reliability and validity of the Danish SCL-90-R have previously been published (Olsen et al., Citation2007).
Subjective cognitive impairment was measured by the Cognitive Failure Questionnaire (CFQ) (Broadbent et al., Citation1982). This questionnaire contains 25 items and is designed to measure the frequency of lapses in perception, memory and action. Each item was scored on a five-point scale ranging from 0 (never) to 4 (very often). The total score (0–100) was calculated as the sum of all item scores.
The neuropsychological test battery
The neuropsychological test battery encompassed the indexes of processing speed (Wechsler Adult Intelligence Scale, WAIS III; Wechsler, Citation1997a), working memory, immediate memory and general memory (Wechsler Memory Scale, WMS III; Wechsler, Citation1997b; for further descriptions, see ). The index scores are based on two or more test scores and transformed into a standardized total score.
Table 1. Description of the indexes in the neuropsychological test battery.
In addition to the indexes, we selected four single tests – the subtest Vocabulary from WAIS-III, the Rey Complex Figure Test (RCFT) (Meyers & Meyers, Citation1995), The Paced Auditory Serial Addition Test (PASAT) (Gronwall & Sampson, Citation1974; Tombaugh, Citation2006) and a self-made test of prospective memory. The Vocabulary was used to estimate premorbid verbal intelligence, and the patients and controls were expected to perform equally well on this test. The single tests are described in detail in .
Table 2. Descriptions of the single tests in the neuropsychological test battery.
All participants were tested in a separate visit to the Department of Occupational Medicine by the same experienced clinical psychologist (the first author). The status of the participants as either patient or control was unknown to the psychologist. The test session lasted for about one-and-a-half hours and was initialized with the instructions for the prospective memory test. The sequence of the rest of the test battery was the same for all participants: (a) Digit Symbol Coding, (b) Symbol Search, (c) Vocabulary, (d) RCFT – copy, (e) Letter-Number Sequencing, (f) RCFT – immediate recall, (g) Logical Memory I, (h) Faces I, (i) Verbal Paired Associates I, (j) Family Pictures I, (k) RCFT – delayed recall, (l) Spatial Span, (m) Logical Memory II, (n) Faces II, (o) Verbal Paired Associates II, (p) Family Pictures II and (q) the PASAT.
Statistical analysis
We performed all statistical analyses in STATA, version 12 (StataCorp LP, College Station, TX).
Regarding hypothesis 1
We transformed the raw scores on the WAIS III and WMS III tests into index scores on the basis of the age of the patients and the norm materials published in the manuals of WAIS III and WMS III. Likewise, we transformed the raw scores on RCFT into T-scores, which are demographically corrected normative scores like the index scores. T-scores have been constructed to have a mean of 50 and a standard deviation (SD) of 10 (Meyers & Meyers, Citation1995), while the index scores have a mean of 100 and a SD of 15.
In addition, effect sizes (Cohen's d) of differences between groups on the neuropsychological tests were calculated by the following formula, . We considered an effect size of 0.2 to be small, 0.5 to be medium and 0.8 to be large (Cohen, Citation1988).
Since the patients and controls were matched pairwise, we applied two-tailed paired Student t tests to examine differences in neuropsychological test performance between the patients and controls. The assumptions were checked by plotting each difference between pairs against the average score (Bland–Altman plot) and by a Q–Q plot of the difference.
We examined if sex, age and educational level were moderating the relation between stress and neuropsychological test performance by conducting multiple regression analyses with the differences on neuropsychological test performance between patients and controls as the dependent variable and sex, age and educational level as the independent variables.
Regarding hypothesis 2
To examine if neuropsychological test performance could be predicted by the level of self-reported perceived stress (PSS10), we conducted several linear regression analyses with PSS10 as the independent variable and results from each neuropsychological test as the dependent variable. We conducted the analyses separately for patients and controls. The models were checked by diagnostic plots of the residuals.
Ethics
All participants gave written informed consent to participate in this study. This study was approved by the Danish Data Protection Agency, and all procedures were carried out in accordance with the Helsinki Declaration. This study did not involve any treatment or biological material and was therefore classified by the regional Health Research Ethics Committee as a survey and consequently it should not be reported to the Committee.
Results
Demographic and clinical characteristics of patients and controls
Sixty patients were recruited. It was not possible to find a match to one patient and, therefore, he was excluded. Demographic and clinical data of the participants are listed in . Patients and controls were similar regarding sex, age and educational level, and the clinical scores of patients were well above the scores of the healthy controls. Patients reported having several cognitive complaints as well as high levels of perceived stress, depressive symptoms, anxiety and somatization. Four patients and one control were medicated with antidepressant medication.
Table 3. Demographic and clinical characteristics of patients and controls.
Hypothesis 1
Patients and healthy controls scored very similar on the vocabulary test. On all outcome measures from the test battery, the performance of patients were lower than that of the healthy controls, but only three comparisons reached statistical significance, including processing speed (mean difference = 8.22 [95% CI: 3.88–12.57], p < 0.001), the PASAT (mean difference = 4.46 [95% CI: 1.52–7.40], p < 0.01) and prospective memory (mean difference = 3.69 [95% CI: 2.35–5.04], p < 0.001; see for more details). These tests also showed the largest effect sizes (Cohen's d > 0.4) between patients and controls ().
Figure 2. Differences in cognitive performance between patients and controls. *p < 0.01, **p < 0.001. The error bars reflect 95% CI.
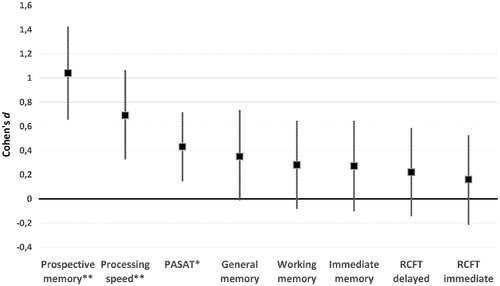
Table 4. Neuropsychological test results from patients (n = 59) and controls (n = 59).
Results on possible moderating effects of sex, age and educational level are listed in . Regarding the effect of educational level and sex, the confidence intervals were very wide, and the only statistical significant difference was an effect of sex on working memory (β = –11.16 [–22.17 to –0.15], p < 0.05). The difference between patients and controls was larger in males compared to females.
Table 5. Multiple regression analyses with differences on neuropsychological test performance between patients and controls as dependent variables and sex, age and educational level as independent variables.
Regarding the effect of age, we found a statistically significant negative association with processing speed, with the difference being larger between younger patients and controls compared to older patients and controls (β = −0.61 [−1.06 to −0.17], p < 0.01). There were no other statistically significant associations.
Hypothesis 2
lists the results of the linear regression analyses between perceived stress and neuropsychological test performance in patients and in controls. We found no statistically significant associations.
Table 6. Associations between perceived stress (PSS10) and neuropsychological test performance.
Discussion
While patients performed worse on all of the neuropsychological outcome measures, all mean index- and T-scores were still within 1 SD from the population mean. In addition, the confidence intervals were relatively wide, and only three comparisons between the groups reached statistical significance. The remaining differences (general memory, immediate memory and the RCFT) could, therefore, be interpreted as chance findings. These differences were small and, as the confidence intervals suggest, may either be considerably reduced or amplified in the general population of patients with chronic work-related stress. We chose not to correct for multiple comparisons because of the risk of making a type II error. However, post hoc analysis revealed that the differences on prospective memory, processing speed and the PASAT remained statistical significant after Bonferroni correction (αBonferroni = 0.05/8 = 0.006), attesting to the robustness of these observations. Overall, our results suggest that patients with work-related stress show mildly impaired neuropsychological test performance.
The most pronounced differences on neuropsychological test performance between patients and controls were seen on prospective memory and processing speed as well as on the PASAT, which measures aspects of working memory, sustained attention, speed and arithmetic ability. These differences were of medium to large effect sizes. Our results regarding processing speed are in line with the results from previous studies (Jonsdottir et al., Citation2013; Öhman et al., Citation2007; Österberg et al., Citation2009), which report results on performance on the digit symbol that is part of the processing speed index of this study.
In the light of knowledge from clinical practice, where patients complain about problems regarding everyday memory, it is not surprising that their test scores of prospective memory are impaired. The remaining memory tests in our test battery are organized in a manner so that the participants are prompted when to initiate a search of memory. In the prospective memory test, however, the participants do not get a direct prompt but have to recall the intention by themselves. In this way, the test demands executive skills of monitoring or searching for the right cue and recalling the intention to act appropriately (McDaniel et al., Citation1999). Thus, it is possible that the lower performance of patients is due to impairments in executive function rather than to memory dysfunctions per se. This is in line with the results of Jonsdottir et al. (Citation2013), who found that the most pronounced differences between patients with stress-related exhaustion and healthy controls were seen on a test of mental control and tracking (the PaSMO).
Regarding the tests of working memory, it was the most demanding test, the PASAT, which showed the largest difference between patients and controls. The WMS III index of working memory, based on the scores from the letter number sequencing and the spatial span, revealed only a small difference. The PASAT demands that the respondent remembers verbally presented numbers and letters while sequencing the numbers and the letters in accordance with the alphabet. This process requires executive function and resembles the PaSMO test from the above-mentioned study of Jonsdottir et al. The raw scores from the letter number sequencing test showed an effect size of 0.4, while the spatial span, which is a simpler task of remembering and replicating a spatial act, showed an effect size below 0.1. In sum, it was the most complex tests of working memory, which showed the largest differences between patients and controls.
Taken together, the largest impairments found were related to executive function and therefore it seems plausible that the impairments are related to dysfunctions in the prefrontal cortex, which are in agreement with findings from previous studies of psychosocial stress related to an upcoming exam (Liston et al., Citation2009) and in patients on long-term sick-leave due to work-related stress (Sandström et al., Citation2012). Declarative and spatial memory, which are primarily related to temporal lobe structures including the hippocampus, seem to be less affected in our sample of patients.
The relatively small differences on measures of memory could be explained by exclusion of patients with diagnosed psychiatric disorders, such as major depression. The symptoms of our group of patients were probably less severe than the symptoms of patients in previous studies with diagnoses of exhaustion disorder or burnout with comorbid major depression. In addition, not all of the patients in our study were on sick-leave. In post hoc analyses, we excluded the 13 patients who had not been on sick-leave in the last three months before inclusion. We found that the differences between patient and controls became larger without these “healthier” patients in the analyses, and the difference on the index of general memory became statistically significant (p < 0.05, data not shown). Therefore, it seems as if our somewhat heterogeneous group of patients has diminished the effect sizes of the study. Furthermore, 51 patients declined to participate in this study, and many of them explained that they could not manage to cope with more activities in their present situation. It seems plausible that these patients were the ones with the most severe stress symptoms, and maybe this has contributed to the relatively small effect sizes found in our study compared to the larger effect sizes from the previous studies.
As previously mentioned, we checked for the moderating effects of the demographic variables sex, age and educational level. The only statistically significant findings were that the difference between patients and controls on working memory was associated with sex and the difference on processing speed were negatively associated to age. In other words, the difference on working memory was largest in males, and the difference on processing speed was largest in the youngest participants. We have no explanations for these findings and are inclined to interpret them as chance findings, since we did several regression analyses and the risk of chance findings are high.
Regarding our secondary hypothesis, we did not find any statistically significant associations between the level of perceived stress and neuropsychological test performance. To our knowledge, this is the first study to examine the association between level of perceived stress and neuropsychological test performance in a clinical sample of patients with work-related stress. However, Aggarwal et al. (Citation2014) found that higher levels of perceived stress were related to lower cognitive function as well as accelerated cognitive decline over nearly seven years of follow-up in a longitudinal population study of 6.207 older adults. It is possible that our negative results are a consequence of too little variability in perceived stress in this sample and therefore more studies with larger samples is needed to test this hypothesis further.
This study has several strengths. First, we included 59 patients and 59 controls to have enough power to detect a medium difference (Cohen's d = 0.5) between the groups. Second, we took special care to match each patient with a healthy control with the same sex, age and educational level as the patient and found that the patient and control groups had the same level of verbal intelligence as measured by the vocabulary test from WAIS III. Third, we excluded patients with major depression to avoid the bias of cognitive impairments being a consequence of depression per se. Finally, we included a test of prospective memory, which resembles the challenges in daily life more than the rest of the test battery. To the best of our knowledge, this has only been done in one previous study (Öhman et al., Citation2007), which also found impairments in a group of patients with perceived stress. In addition, we calculated index scores that should be more robust than single tests scores, and the number of comparisons between patients and controls were therefore reduced, along with the risk of chance findings. Furthermore, the calculation of indexes facilitates the judgment of whether impairments are clinical significant due to the existence of well-validated norms.
There are also several limitations to this study. First, the study faced limitations regarding the inclusion of participants. As mentioned above, 51 patients declined to participate, and this fact limits the generalizability of this study. In addition, we sent out 848 letters to potential controls but could include only 59 controls. Thus, the sample of controls was a self-selected group. Unfortunately, we do not know what attributes may distinguish individuals who accepted the offer of participation from those who did not respond to our invitation, since we have no data on the latter population. Nonetheless, we attempted to minimize self-selection bias as much as possible, since we only sent out an invitation to five relevant individuals and wrote that we had selected him or her because we needed a healthy individual with exactly the same age, sex and educational level as a particular patient who was already included. In this way, we hoped to motivate individuals who would not otherwise have responded to an advertisement in a newspaper or in another public display.
A second important limitation of this study concerns the test of prospective memory. As mentioned earlier, this test was a self-made test and it has not previously been validated. Therefore, we cannot be certain that it measures what we believe it measures. To examine the construct validity, we made a linear regression analysis with the test scores from the prospective memory test as the independent variable and item number 16 from the CFQ (Broadbent et al., Citation1982) (How often do you forget appointments?) as the dependent variable. The prospective memory test explained 5% of the variance (p = 0.05) in the patient group, but there was no association in the control group. This could probably be explained by the low variability in the responses of controls to item 16 from the CFQ. The validity of our self-made test should be further tested in future studies.
Third, we attempted to blind the examiner for the participants' status as either patient or control, but occasionally, a participant disclosed their status by accident, and a few patients were obviously distressed during the test session. The examiner followed the manual stringently in instructions given and in the process of scoring the responses of the participants and, therefore, the risk of bias should be minimal. If anything, the examiner could unintentionally have been inclined to talk slower and be more supportive towards the participants who were obviously distressed by the tests and therefore, it would probably have made the differences between patients and controls smaller.
A fourth limitation of this study was that there were only nine men in both groups and, therefore, our results may not be generalizable to other men. However, a relatively recent study by Beck et al. (Citation2013) found that acute burnout was related to impaired executive function in a sample of male patients.
Finally, another important limitation is the cross-sectional design of this study. This makes it impossible to make conclusions regarding causality. Therefore, it might be possible that cognitive impairments were present already before the patient became ill and if so, such impairments might in fact have contributed to the development of the stress-related problems. In addition, it is still uncertain if the impairments found are permanent or reversible. Results from a few studies indicate that the cognitive impairments are partly reversible, but that neuropsychological test performance still remains below levels of healthy controls one to two years after acute burnout (Österberg et al., Citation2012, Citation2014; van Dam et al., Citation2012; Wahlberg et al., Citation2009). We are in the process of organizing another test session with both the patient and the control group from this study to examine whether the performances of patients change relative to the change in the control group. Findings from this study will be reported later.
Conclusion
In conclusion, patients with work-related stress showed mild impairments in neuropsychological test performance relative to healthy controls. The most pronounced differences between patients and controls were seen on tests that are highly dependent upon executive function, namely prospective memory, processing speed and complex working memory. These impairments should, therefore, be considered when evaluating patients with work-related stress complaints, especially when given advice regarding return to work so that patients can seek the support they need and avoid too demanding tasks until their cognitive functions are normalized. Self-reported perceived stress was not statistically significant related to neuropsychological test performance.
The research field would benefit from future prospective studies, screening healthy workers with tests of prospective memory, processing speed and complex working memory and conducting several follow-ups to examine if the perception of chronic work-related stress causes cognitive impairments and/or if cognitive impairments are a risk factor of work-related stress.
Acknowledgements
The authors thank all the patients and controls participating in this study, Birthe B. Hjort for administrative work and David Glasscock, Claus Friche, Lotte Q. Michaelsen, Ole B. Knudsen and Kåre Spliid for all the psychological assessments.
Declaration of interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of this article.
This study was funded by The Danish Working Environment Research Fund, The Health Research Fund of Central Denmark Region, and The Danish Ramazzini Centre.
References
- Aggarwal NT, Wilson RS, Beck TL, Rajan KB, Mendes de Leon CF, Evans DA, Everson-Rose SA. (2014). Perceived stress and change in cognitive function among adults 65 years and older. Psychosom Med 76:80–5
- Austin M, Mitchell P, Goodwin G. (2001). Cognitive deficits in depression: possible implications for functional neuropathology. Br J Psychiatry 178:200–6
- Bech P, Gram LF, Dein E, Jacobsen O, Vitger J, Bolwig TG. (1975). Quantitative rating of depressive states. Acta Psychiatr Scand 51:161–70
- Beck J, Gerber M, Brand S, Pühse U, Holsboer-Trachsler E. (2013). Executive function performance is reduced during occupational burnout but can recover to the level of healthy controls. J Psychiatr Res 47:1824–30
- Bonde JP. (2008). Psychosocial factors at work and risk of depression: a systematic review of the epidemiological evidence. Occup Environ Med 65:438–45
- Broadbent D, Cooper P, FitzGerald P, Parker K. (1982). The Cognitive Failure Questionaire and its correlates. J Clin Psychol 21:1–16
- Cohen S, Kamarck T, Mermelstein R. (1983). A global measure of perceived stress. J Health Soc Behav 24:385–96
- Cohen J. (1988). Statistical power analysis for the behavioral sciences. 2nd ed. USA: Lawrence Erlbaum Associates
- Derogatis LR. (1977). SCL-90-R: Symptom Checklist-90-R. Administration, scoring and procedures manual. 1st ed. Minneapolis, MN: National Computer Systems
- Gronwall D, Sampson H. (1974). The psychological effects of concussion. Auckland, New Zealand: Auckland University Press
- Grynderup MB, Mors O, Hansen ÅM, Andersen JH, Bonde JP, Kærgaard A, Kærlev L, et al. (2013). Work-unit measures of organisational justice and risk of depression – a 2-year cohort study. Occup Environ Med 70:380–5
- Hamilton M. (1960). A rating scale for depression. J Neurol Neurosurg Psychiatry 23:56–62
- Hasselberg K, Jonsdottir IH, Ellbin S, Skagert K. (2014). Self-reported stressors among patients with exhaustion disorder: an exploratory study of patient records. BMC Psychiatry 14:66
- Jonsdottir IH, Nordlund A, Ellbin S, Ljung T, Glise K, Währborg P, Wallin A. (2013). Cognitive impairment in patients with stress-related exhaustion. Stress 16:181–90
- Kompier M. (2006). New systems of work organization and workers' health. Scand J Work Environ Health 6:421–30
- Lazarus RS, Folkman S. (1984). Stress, appraisal, and coping. New York, NY: Springer
- Lezak MD, Howieson DB, Loring DW. (2004). Neuropsychological assessment, 4 ed. New York: Oxford University Press
- Liston C, McEwen BS, Casey BJ. (2009). Psychosocial stress reversibly disrupts prefrontal processing and attentional control. Proc Natl Acad Sci USA 106:912–17
- Maslach C, Schaufeli W, Leiter M. (2001). Job burnout. Annu Rev Psychol 52:397–422
- McDaniel MA, Einstein GO. (2007). Prospective memory. An overview and synthesis of an emerging field. Thousand Oaks, CA: Sage Publications
- McDaniel MA, Glisky EL, Guynn MJ, Routhieaux BC. (1999). Prospective memory: a neuropsychological study. Neuropsychology 13:103–10
- Meyers J, Meyers K. (1995). Rey Complex Figure Test and recognition trial. Professional manual. Odessa, FL: Psychological Assessment Resources Inc
- Öhman BA, Nordin S, Bergdahl J, Birgander LS, Neely AS. (2007). Cognitive functions in outpatients with perceived chronic stress. Scand J Work Environ Health 33:223–32
- Olsen LR, Mortensen EL, Bech P. (2007). Dokumentation for den danske udgave af SCL-90-R. In: Hartmann P. SCL-90-R Vejledning til administration og scoring. Dansk Psykologisk Forlag . p 51–71
- Österberg K, Karlson B, Hansen ÅM. (2009). Cognitive performance in patients with burnout in relation to diurnal salivary cortisol. Stress 12:70–81
- Österberg K, Skogsliden S, Karlson B. (2014). Neuropsychological sequelae of work-stress-related exhaustion. Stress 17:59–69
- Österberg K, Karlson B, Malmberg B, Hansen ÅM. (2012). A follow-up of cognitive performance and diurnal salivary cortisol changes in former burnout patients. Stress 15:589–600
- Sandström A, Rhodin IN, Lundberg M, Olsson T, Nyberg L. (2005). Impaired cognitive performance in patients with chronic burnout syndrome. Biol Psychol 69:271–9
- Sandström A, Sall R, Peterson J, Salami A, Larsson A, Olsson T, Nyberg L. (2012). Brain activation patterns in major depressive disorder and work stress-related long-term sick leave among Swedish females. Stress 15:503–13
- Tombaugh TN. (2006). A comprehensive review of the Paced Auditory Serial Addition Test (PASAT). Arch Clin Neuropsychol 21:53–76
- van Dam A, Keijsers GPJ, Eling PTAM, Becker ES. (2011). Testing whether reduced cognitive performance in burnout can be reversed by a motivational intervention. Work Stress 25:257–71
- van Dam A, Keijsers GPJ, Eling PATM, Becker ES. (2012). Impaired cognitive performance and responsiveness to reward in burnout patients: two years later. Work Stress 26:333–46
- Videbech P, Bonde A, Damsbo N, Deleuran A, Gormsen K, Holm M, Hvenegaard A, et al. (2007). Referenceprogram for unipolar depression hos voksne. Copenhagen: The Danish Health and Medicines Authority
- Wahlberg K, Ghatan PH, Modell S, Nygren Å, Ingvar M, Åsberg M, Heilig M. (2009). Suppressed neuroendocrine stress response in depressed women on job-stress-related long-term sick leave: a stable marker potentially suggestive of preexisting vulnerability. Biol Psychiatry 65:742–7
- Wechsler D. (1997a). Wechsler Adult Intelligence Scale (3rd ed.). San Antonio: The Psychological Corporation
- Wechsler D. (1997b). Wechsler Memory Scale. Third edition manual. San Antonio: The Psychological Corporation
- Yu X, Wang P, Zhai X, Dai H, Yang Q. (2014). The effect of work stress on job burnout among teachers: the mediating role of self-efficacy. Soc Indicat Res. [Epub ahead of print]. doi 10.1007/s11205-014-0716-5