
Abstract
Hyperlipidemia is a prevailing risk factor that leads to development and progression of atherosclerosis and consequently cardiovascular diseases. Several antihyperlipidemic drugs are having various disadvantages such as low water solubility and poor bioavailabilty due to presystemic gastrointestinal clearance. Thus, there is a considerable need for the development of efficient delivery methods and carriers. This review focuses on the importance and role of various nanoparticulate systems as carrier for antihyperlipidemic drugs in the treatment of hyperlipidemia. Some nanoparticle technology-based products are approved by FDA for effective treatment of hyperlipidemia, namely Tricor® by Abbott Laboratories (Chicago, IL, USA) and Triglide® by Skye Pharma (London, UK). Efforts to address each of these issues are going on, and should remain the focus on the future studies and look forward to many more clinical products in the future.
Introduction
Hyperlipidemia is a general disorder of lipid metabolism qualified by raised levels of total cholesterol and triglycerides. It is commonly characterized by an increased flow of free fatty acids (FFAs), increased triglycerides, low-density lipoprotein (LDL)-cholesterol and apolipoprotein B (apoB) levels, and abridged plasma high-density lipoprotein (HDL)-cholesterol concentration (Kolovou et al., Citation2005), which is the key risk factor for atherosclerosis or cardiovascular diseases (CDVs) including coronary heart diseases and several other disorders and has been described as the most common cause of death in developed as well as developing countries (Simons, Citation2002; Reiner & Tedeschi-Reiner, Citation2006) ().
Primary hyperlipidemia is probably genetically based, but the genetic defects are predictable for only a minority of patients.
Secondary hyperlipidemia can result from some diseases such as diabetes, liver disorders renal disorders, thyroid disease, Cushing’s syndrome, thyroid disease and, as well as obesity, estrogen administration, alcohol consumption and other drug-associated alterations in lipid metabolism.
Table 1. Normal adult blood cholesterol level (Brahm & Hegele, Citation2013).
Some factors can influence lipoprotein or cholesterol levels (van Lennep et al., Citation2002):
Total cholesterol and triglycerides level can be raised by using some diuretics.
Menstrual period can lead to decrease in LDL level and increase in HDL level in women.
During pregnancy, total cholesterol level can increase and remain elevated for up to 20 weeks after delivery.
Total cholesterol levels are lowest in the summer and highest in the winter.
Estrogen replacement therapy leads to lower total cholesterol and LDL, and higher HDL.
Causes of hyperlipidemia
An elevation in plasma lipids may be caused by a primary genetic defect or secondary to diet, drugs or diseases. Hyperlipidemia can commonly be assigned to one of four main categories, with inherited disorders of lipid metabolism, hypercholesterolemia caused by diet, diseases inducing secondary hyperlipidemia and drug effects (Slack, Citation1969).
The majority of cholesterol is synthesized endogenously. The rate-limiting enzyme for the synthesis of endogenous cholesterol is 3-hydroxy-3-methylglutaryl coenzyme A (HMG CoA) reductase, blockade of which provides an important prospect for pharmacologic therapy. Cholesterol and triglycerides which are endogenously synthesized are packaged into soluble particles by liver. Soluble particles consist of cholesterol ester and triglycerides-rich core which is surrounded by phospholipid membrane that comprises of various apolipoproteins. Various properties of apolipoproteins include purvey of recognition sites for various receptors which help specific metabolism of these particles by lipoprotein lipase with metabolism of triglycerides in the circulation. Initially, liver produced very low-density lipoproteins (VLDL) which is rich in triglycerides. These particles become smaller in size forming LDLs or LDL/oxidized LDL by degradation with the help of enzyme lipoprotein lipase. These circulating LDL can be taken up by macrophages or reuptaken by the liver by specific receptors and clearance from the circulation. Cholesterol-rich particles called HDL, having antioxidant properties, initiate reverse cholesterol transport which gives it properties that aids in resistance to atherosclerosis. Chylomicrons consist of very large particles of dietary fat absorbed in the intestine which is influenced by lipoprotein lipase, and ultimately, the ends of these particles are taken up by the living cells (McCrindle et al., Citation2003). discusses the various causes of hyperlipidemia.
Table 2. Causes of hyperlipidemia (Starc, Citation2001).
Hyperlipidemia is cholesterol and high fat in the blood due to other conditions or medications. The measurement of cholesterol and triglycerides is the most practical means of detecting hyperlipidemia and provides some information based on the type of hyperlipidemia. It is classified according to the Fredrickson classification which is dependent on the pattern of lipoproteins on ultracentrifugation or electrophoresis. Later on, it was adopted by the World Health Organization (WHO) ().
Table 3. Classification of hyperlipidemia (WHO/Modified Fredrickson) (Hegele, Citation2009).
These HLP types are distinct by the particular classes of TG-rich lipoprotein particles that accumulate in plasma, including VLDL, chylomicrons or intermediate-density lipoprotein (IDL). Simple HTG, namely HLP type 4, is specified by elevated VLDL concentrations. But, the other HLP types have more composite lipoprotein disturbances. For example, HLP type 5 is characterized by increase in both VLDL concentrations and chylomicron. HLP type 3 is qualified by elevated IDL concentrations. HLP type 2 is determined by elevated VLDL and LDL concentrations. Furthermore, reduced HDL cholesterol is usually seen among patients with all types of HTG (Hegele et al., Citation2009).
Classification of current conventional marketed formulations for hyperlipidemia with their mechanism of action
Drugs used for the treatment of hyperlipidemia are found to be of different classes that are HMG CoA reductase inhibitors, fibrates, cholesterol absorption inhibitors, nicotinic acid group, bile acid sequestrants and have various different mechanisms of actions for management of hyperlipidemia. discusses the classification of current conventional-marketed formulations for hyperlipidemia.
Table 4. Classification of current conventional marketed formulations for hyperlipidemia.
Mechanism of action of different antihyperlipidemic agents
HMG CoA reductase inhibitors (statins)
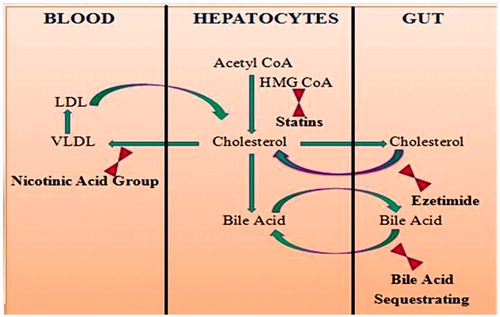
The HMG CoA reductase inhibitors, or statins, are commonly used in the treatment of hyperlipidemia and have led to the significant reductions in cardiovascular and all-cause fatality in the setting of both primary and secondary prevention of atherosclerotic CDV. The statins work by inhibiting the rate-limiting enzyme, HMG CoA reductase, in the endogenous synthesis of cholesterol (). HMG CoA converts to mevalonate in the presence of HMG CoA and mevalonate aids to further synthesis of cholesterol. Therefore, statins works by inhibiting HMG CoA which further leads to decrease in cholesterol level and prevention of dyslipidemia (Kwiterovich, Citation1998).
Figure 1. Mechanism of action of different antihyperlipidemic agents: HMG CoA reductase inhibitors (statins), cholesterol absorption inhibitors, nicotinic acid group and bile acid sequestrants.
Fibrates
These are acts by stimulating the peroxisome proliferator activated receptor alfa (PRAP)-α which controls expression of gene products that mediates the effect of HDL and TG. As a result, synthesis of folic acid, triglycerides and VLDLs is reduced which helps in reducing cholesterol level (Staels et al., Citation1998).
Cholesterol absorption inhibitors
Ezetamide is the only currently synthesized drug acts by inhibition of Niemann–Pick C1-like 1 (NPC1L 1) protein which helps in blockade of dietary cholesterol absorption without altering the absorption of triglycerides, fat-soluble vitamins and bile acids. In general, cholesterol absorption inhibitors prevents the uptake of cholesterol from intestine to blood circulation (), leads to compensatory upregulation of LDL receptors on the cell surface and increases LDL cholesterol uptake into cells which ultimately decreases blood LDL cholesterol content (Kontush & Chapman, Citation2006; Rozman & Monostory, Citation2010).
Nicotinic acid group
Nicotinic acid group is to decrease hepatic production and the release of VLDL. Its lipid-lowering effect ensues lowering of triglycerides and LDL with increase in HDL. In pharmacological doses (in grams), niacin decreases peripheral FA release (by inhibiting lipolysis in adipose tissue) into the circulation which the liver uses for TG synthesis. This TG is necessary for VLDL synthesis in the liver. Also, LDL is derived from VLDL in the plasma. Therefore, a reduction in the VLDL production contributes to reduce LDL levels (). The result therefore is decreased TC and TG, whereas HDL is increased (Colletti et al., Citation1993).
Bile acid sequestrants
These are anion exchange resins that bind to bile acids and bile salts which are negatively charged. This complex is excreted in feces and therefore the reabsorption of bile acids to liver through the enterohepatic circulation is prevented (). As a result, the liver increases de novo synthesis of bile acids from hepatic cholesterol. The resultant decrease in hepatic cholesterol helps in upregulation of LDL receptor activity and decrease in LDL in similar manner to statins (Shepherd, Citation1989).
Nanoparticle carrier system
The use of advanced nanoparticle carrier systems is a strategy to design pharmaceutical dosage forms with better therapeutic benefits. Nanoparticles are one of the most widely investigated carriers, in particular, to improve the therapeutics of potent drugs. They can be used to ascertain the retention of entrapped drugs in the presence of biological fluids and improved vesicle uptake by target cells. Nanoparticle-based dosage forms are administered through many routes: oral, parenteral, ocular, intranasal, dermal/transdermal and vaginal. However, oral remains the ideal route because it is non-incursive, less expensive and has fewer tendencies for side effects, such as reactions on injection site. It is also the easiest and the most commodious means of drug delivery for chronic therapies (Peer et al., Citation2007; Davis & Shin, Citation2008).
Nanoparticle research is presently a field of strong scientific research due to a wide variety of possible applications in biomedical, optical and electronic subjects (). Nanoparticles form an effectual bridge between bulk materials and atomic or molecular structures. The attributes of materials change as their size approaches the nanoscale and as the percentage of atoms on the surface of a material becomes significant.
Table 5. Work done of different nanoparticles with hyperlipidemia.
Nanoparticles have a very high surface area to volume ratio which provides a tremendous driving force for diffusion especially at elevated temperatures. Large surface area to volume ratio also reduces the initial melting temperatures of nanoparticles.
NIH determined the application of nanotechnology for treatment, monitoring, diagnosis and control of biological systems as nanomedicine. Among the approaches for exploiting nanotechnology developments in medicine, several nanoparticulates offer certain unique advantages as pharmaceutical delivery systems and image enhancement agents (West & Halas, Citation2000; LaVan et al., Citation2002). Varieties of nanoparticles (Sahoo & Labhasetwar, Citation2003) such as different polymeric and liposomes, metal nanoparticles, micelles, quantum dots, microcapsules, dendrimers, cells, cell ghosts, lipoproteins and many different nanoassemblies are available. All these nanoparticles can play a main role in diagnosis and therapy.
Toxicity associated with nanoparticles
Humans have been disclosed to nanoparticles all through their evolutionary phases; but, this exposure has been increased to a high level in the past century because of the industrial revolution. Nanoparticles comprise a part of particulate matter (PM).
Pollution with airborne PM deriving from combustion sources such as motor vehicle and industrial emissions leads to respiratory and cardiovascular morbidity and mortality. A distinctive ambient PM is a highly complex mix of particles with median diameter size ranging from nm to 100 mm. Only the part of these particles with a mass median diameter of 2.5 mm or less is capable of depositing deep in the lung. The majority of the ambient particles are submicron in size because they are created from combustion of fossil fuels or are formed by reactions from gases generated by such incinerations. An emblematic urban atmosphere contains ∼107 particles/cm3 of air that is less than 300 nm in diameter. Carbon in elemental form is a key component of these particles and the size of these particles is a determinant of their power to cause systemic cardiovascular effects (Brook et al., Citation2004).
Therefore, any intrinsic toxicity of the particle surface will be increased. The respiratory system, blood, central nervous system, gastrointestinal tract and skin have been proven to be targeted by nanoparticles.
Nanoparticles suggest significant advantages over free therapeutic agents. Some of the important technological advantages of nanoparticles used as drug carriers are follows:
High stability and high carrier capacity.
Possibility of incorporation of both hydrophilic and hydrophobic active substances.
Possibility of varying administrating routes for drug delivery, including oral application and inhalation.
Nanoparticles may also be designed to permit-controlled (sustained) drug release from the matrix.
These attributes of nanoparticles enable improvement of drug bioavailability and reduction of the dosing frequency. Some therapeutic nanoparticles are typically in the size of 10–200 nm and consist of peptides, proteins, nucleic acids or therapeutic active ingredients, in association with a carrier molecule, and existing clinical problems are overcome by the great potentials in their capacities (Peer et al., Citation2007; Cho et al., Citation2008; Davis & Shin, Citation2008). It is now well known that the intrinsic physical and chemical properties of nanoparticles (shape, size, surface characteristics) as well as its contact with environment can dictate a nanoparticles degree of biocompatibility. Thus, with deference to other colloidal drug delivery systems (like liposomes, noisome or microemulsions) have better kinetic stability and rigid morphology (Kreuter, Citation1994; Dobrovolskaia et al., Citation2008; Aggarwal et al., Citation2009).
Importance of nanoparticles in treatment of hyperlipidemia
Improvement of safety and efficacy of drug
As a lipid lowering agent, atorvastatin calcium (AC) is a second-generation 3-hydroxy-3-methylglutaryl-CoA reductase inhibitor accepted for clinical use associated with its serious adverse effects after chronic administration like rhabdomyolysis and poor oral bioavailability. To amend the safety and efficacy of AC, biodegradable nanoparticulate approach was introduced. Using a co-solvent approach by emulsion–diffusion–evaporation method, poly lactide-co-glycolic acid (PLGA) nanoparticles were prepared with the help of two stabilizers, i.e. vitamin E tocopheryl polyethylene glycol 1000 succinate (Vit E–TPGS) and didodecyl dimethyl ammonium bromide.
High-fat diet-fed (hyperlipidemic) rats were used for the evaluation of safety and efficacy parameters of the prepared nanoparticles against marketed formulation. In comparison to Lipicure®, AC nanoparticles were evenly effective at a 66% reduced dose in treating the hyperlipidemia specified by changes in PTC, LDL-C, VLDL-C, HDL-C, PTG and PGL in the high-fat diet-fed rats (Meena et al., Citation2008).
Potential use of drug with reduced toxicity
Hyperlipidemia is a main risk factor that leads to the progression and development of most serious diseases in humans, i.e. atherosclerosis and subsequent CDV (Prasad & Kalra, Citation1993; Deepa & Varalakshmi, Citation2005; Zhang et al., Citation2011). Recently, numerous approaches have intended on how to reduce plasma lipid concentrations and the absorption of fat in the intestinal tract to cut down diet-related chronic disease. Dietary fibers, e.g. psyllium, pectin and chitosan, show some effective hypolipidemic effect (Zhang et al., Citation2008).
Hypolipidemic effects of chitosan nanoparticles (CTS-NPs) prepared with rotary evaporation, ionotropic gelation and spray-drying technique were examined. Male SD (Sprague–Dawley) rats were separated into five groups: a normal control diet group, a high-fat emulsion group, CTS control group and CTS-NP groups treated with two different doses of CTS-NP. Results proposed that spray-drying was a suitable method for the preparation of CTS-NP. Furthermore, CTS-NP was effective in lowering body weight gain and serum lipid levels in rats fed with high-fat emulsions. Acute toxicity showed that the CTS-NPs were non-toxic. All of these results provide greater approach on the potential use of CTS-NP in humans.
Digestion of bad cholesterol (LDL)
Hyperlipidemia, a condition related with atherosclerosis, can build up because of the deficiency of LDL receptors in hepatocytes. LDL-absorbing nanoparticles possibly enhanced the LDL delivery to the liver, as injected polymeric nanoparticles are rapidly taken up by Kupffer cells of liver. Mouse macrophage cell line study was performed using a model for liver Kupffer cells to determine the intake of the antibody–nanoparticle–LDL complexes by cells. It was found that macrophages can rapidly take up antibody–nanoparticle–LDL complexes and digest them within 24 h (Maximov et al., Citation2010).
Enhance effectiveness of drug
Chitosan, a deacetylated product of chitin, has been manifested to lower cholesterol in animals and humans. In addition, reactivity of water-soluble chitosan (WSC) is higher when compared with chitosan. The present study was intended to elucidate the effects of WSC and WSC nanoparticles (WSC-NPs) on hypercholesterolemia induced by feeding a high-fat diet in male Sprague–Dawley rats (Tao et al., Citation2011).
WSC-NPs were prepared by the ionic gelation method and the spray-drying technique. Chitosan is a natural cationic polysaccharide consisting of (1-4)-2-amino-2-deoxy-d-glucopyranosyl units. Its slow decomposition leads to harmless products (amino sugars), which are entirely absorbed by the human body (Ostanina et al., Citation2008). Numerous studies have shown that chitosan has cholesterol-lowering attributes both in animals and humans (Ausar et al., Citation2003; Zhang et al., Citation2008).
WSC is water soluble due to its lower viscosity. Later on, it seems to be readily absorbed in vivo. And, WSC has been described to have the health welfares such as liver protection, antitumor, immunity regulation, blood lipids lowering, and antioxidant and antidiabetic properties (Cho et al., Citation2008; Dobrovolskaia et al., Citation2008). In particular, previous studies exposed that in comparison with chitosan, WSC was effective at lowering lipid level (Aggarwal et al., Citation2009). Therefore, this study examined the effects of WSC and WSC-NPs on hypercholesterolemia induced by feeding a high-fat diet in rats. In conclusion, the data generated by this study verified that WSC-NPs not only lower plasma viscosity and serum lipids levels, but also increased serum SOD activities. Moreover, the hypercholesterolemia is even more affected by WSC-NPs than the WSC.
Types of nanoparticulate carrier systems with their role in treatment of hyperlipidemia
Polymers nanoparticles
Solvent evaporation method was used for the preparation of atorvastatin-loaded chitosan nanoparticles for sustained release. An extensive high first-pass effect leads to low oral bioavailability of AC (14%) and makes it a major target for oral-sustained drug delivery.
Solvent evaporation methods were used for the preparation of atorvastatin-loaded chitosan nanoparticles in four different ratios: 1:1, 1:2, 1:3 and 1:4. According to entrapment and efficiency of yield, 1:4 ratios demonstrated better yield when compared to the other three ratios. Size of the nanoparticles increased with increase in the amount of polymer. It was observed that the higher the Zeta potential; less will be the particle aggregation and hence more will be the stability of nanoparticles (Bathool et al., Citation2012).
Estradiol-encapsulated PLGA nanoparticles were prepared by emulsion–diffusion–evaporation method and evaluated in estrogen-deficient (ovariectomized) high-fat diet-induced hyperlipidemic rat model. The results indicated that estradiol nanoparticles were equally/more effective in treatment of estrogen-deficient hyperlipidemic conditions at three times reduced frequency and dose in comparison with that of drug suspension administered orally. Together, these results revealed the ability of nanoparticles in improving oral efficacy or bioavailability of estradiol (Mittal et al., Citation2009).
Supercritical antisolvent (SAS) process was used for successful preparation of amorphous AC nanoparticles, with ∼152–863 nm in mean particle size, using methanol. The absorption of AC after oral administration of amorphous AC nanoparticles to rats was markedly increased due to enhanced dissolution and supersaturation properties.
Therefore, preliminary results from this study recommended that the preparation of amorphous AC nanoparticles using SAS process could be a promising approach to improve dissolution, supersaturation and absorption properties of atorvastatin. The absorption of AC after oral administration of amorphous AC nanoparticles to rats was markedly increased (Kim et al., Citation2008).
Lipidic nanoparticles
Nanoparticle-based technologies improved certain properties of this poorly water-soluble drug, lovastatin, namely, stability, drug loading efficiency, effective first-pass uptake into hepatic cells, faster excretion, less toxicity, maximum plasma concentration and bioavailability. The nano-aided drug delivery system is a suitable choice for poorly soluble lipophilic drugs (Seenivasan et al., Citation2011).
Homogenization followed by ultrasonication method is suitable to produce solid–lipid nanoparticle (SLN) of 50–125 nm size ranges. Lipophilic drugs like atorvastatin (ATRS) can be successfully loaded with triglycerides, non-toxic surfactants like Phosphatidlycholine and Poloxamer 188. The entrapment efficiency and the drug release profile were found to depend on the concentration of lipid and surfactant mixture employed. As the surfactant concentration was decreased from 1.5% to 0.75%, there was decrease in controlled release properties of the SLN formulations. Stability studies show that after 40 days of storage at different temperatures, the mean diameters of SLNs remain practically the same, which emphasizes the stability of lipid particles. These data collectively support that SLNs are the promising delivery systems for poorly water-soluble drugs such as ATRS (Kumar et al., Citation2012b).
Solid–lipid nanoparticles are another carrier system utilized to load the drug for targeting, to ameliorate the bioavailability by increasing its permeability and solubility and to protect the drug from presystemic metabolism.
Abdul Hasan Sathali et al. have developed and characterized rosuvastatin calcium-loaded SLNs, because of its low solubility, low permeability and poor oral bioavailability. Furthermore, it could be established that with nanometer size range particles, bioavailability must be enhanced. Hence, we can conclude that SLNs improved the bioavailability of poor water-soluble and low lipophilic drug like rosuvastatin calcium as a drug delivery system (Sathali et al., Citation2013).
Nanostructured lipid carriers (NLCs) made from mixtures of Precirol and Squalene were prepared to examine whether the bioavailability of lovastatin can be enhanced by oral delivery. The principle of this study was to evaluate the possibility of using NLCs to enhance the oral absorption of lovastatin. An oral pharmacokinetic study was carried out in rats, and the results described that when compared to free solution, NLCs produced a significant enhancement in the bioavailability. The types of emulsifier had an essential influence on the oral absorption of lovastatin.
Lovastatin administration from myverol-containing NLCs contributes to plasma concentrations which were less variable, greater and more prolonged when compared to the drug that was given in the free form. Changes in pharmacokinetic parameters with NLCs can improve the clinical efficacy of lovastatin (Chen et al., Citation2010). Simvastatin (SV) is a cholesterol-lowering agent which is commonly used in the treatment of dyslipidemia, hypercholesterolemia and coronary heart disease. But, SV expressing poor aqueous solubility and extensive metabolism by cytochrome-3A system in intestinal guts and liver leads to its low-oral bioavailability.
The SLNs manifested nanometer range spherical structure characterized by laser light scattering. The absorption of SLNs in rat intestine was greatly improved when compared with free SV. These results proposed that lipid nanoparticles could be a talented delivery system to enhance the oral bioavailability of simvastatin (Zhang et al., Citation2010).
Mechanisms of diverse systems in hyperlipidemia
Pathways involved chylomicrons synthesis by the intestine and VLDL synthesis by the liver, and mechanisms of various systems like self-microemulsifiying drug delivery systems and pulsatile drug delivery system in hyperlipidemia are discussed below.
Pathways involved chylomicrons synthesis by the intestine and VLDL synthesis by the liver
The liver is centre to the regulation of cholesterol levels in the body. It does not synthesize cholesterol for exporting to other cells; however, it also removes cholesterol from the body by converting it into bile salts and putting down into the bile, where it can be eliminated in the feces. Lipids are transported in the circulation packaged in lipoproteins. Lipoproteins can be distinguished on the basis of their density, but also by the types of apolipoprotiens. The amount of lipid in a lipoprotein affects its density – the lower the density of a lipoprotein, the more the lipids it contains when compared with protein. Four major types of lipoproteins are chylomicrons, VLDL, LDL and HDL.
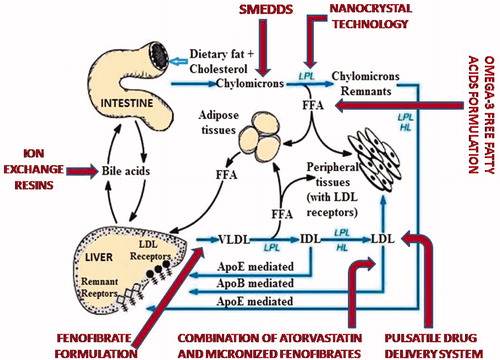
Two types of lipoproteins are triglyceride-rich: chylomicrons and VLDL. Enterocytes are the site for synthesis of chylomicrons from lipids absorbed in the small intestine. VLDL is synthesized in the liver (). Surplus cholesterol is eliminated from the body through liver, which secretes cholesterol in bile or converts it into bile salts. LDL and other lipoproteins are also removed from the circulation by liver through receptor-mediated endocytosis.
Figure 2. Pathways involved chylomicrons synthesis by the intestine and VLDL synthesis by the liver and mechanisms of diverse systems in hyperlipidemia. Abbreviations: LDL, IDL and VLDL – level inhibition of chylomicrons, FFA – free fatty acids, LPL – lipoprotein lipase, LDL – low-density lipoproteins, IDL – intermediate density lipoproteins, VLDL – very low-density lipoproteins, LPL – lipoprotein lipase, ![]()
Individuals with this disorder have several-fold higher levels of circulating LDL due to a defect in the function of their LDL receptors. With no functioning of LDL receptors, this LDL is not cleared from the circulation. Additionally, as cholesterol cannot get into cells efficiently, no negative feedback suppression of cholesterol synthesis in the liver is observed. Dyslipidemia is the term that is used if lipid levels are outside the normal range. High levels of LDL cholesterol (the so-called “bad cholesterol”) heavily increase the risk for atherosclerosis because LDL particles contribute to the formation of atherosclerotic plaques. Low-HDL levels (“good cholesterol”) are an independent risk factor, as reverse cholesterol transport works to prevent plaque formation, or still causing regression of plaques once they have formed. Fasting triglyceride levels are used to estimate the level of VLDL.
The most important mechanisms used to decrease cholesterol level by decreasing the level of chylomicrons, VLDL and LDL are as follows.
Mechanisms of diverse systems in hyperlipidemia
Self-microemulsifiying drug delivery systems
This work aims to examine the effect of different amount of oil or surfactant incorporated in self-microemulsifying drug delivery systems on the intestinal lymphatic transport of sirolimus using the single-pass intestinal perfusion (SPIP) technique, and a chylomicron flow blocking approach () leads to inhibition of cholesterol synthesis (Sun et al., Citation2011).
Nanocrystal technology
Fenofibric acid is a metabolic product of fenofibrate which activates the PPARα (peroxisome proliferator-activated receptor α). Fenofibrate increases the lipolyses and the elimination of triglycerides-rich particles from the plasma by activating the lipoprotein lipase and reducing the production of apoprotein C-III, which is an inhibitor () of the lipoprotein lipase activity (Witztum, Citation1996; Ehnholm et al., Citation2001).
Omega-3 FFA formulation
This study was designed to evaluate the efficacy of adding OM3-FFA (2 or 4 g/day) to statin therapy for lowering non-HDL-C and TG levels in subjects with persistent hypertriglyceridemia and at high risk for CDV. OM3-FFA was well-tolerated and lowered non-HDL-C and TG levels at both 2 and 4 g/day dosages in patients with persistent hypertriglyceridemia taking a statin, along with the 4 -g/day dosage providing incremental improvements compared with 2 g/day (Maki et al., Citation2013).
Pulsatile drug delivery system
Development of pulsatile drug delivery system depends on an insoluble capsule body filled with simvastatin microspheres and sealed with HPMCK4M plug is carried out in present study. Simvastatin is a water-insoluble drug and its absorption is dissolution rate limited. Therefore, simvastatin microspheres were prepared by quasi emulsion solvent diffusion method of the spherical crystallization technique (Sukanya & Kishore, Citation2012).
Combination of atorvastatin and micronized fenofibrate
Administration of micronized fenofibrate reduced serum triglycerides (p < 0.01) and total cholesterol and LDL cholesterol (p < 0.05 for both parameters), as it evoked a significant increase in serum HDL cholesterol levels (p < 0.05). Monotherapy of atorvastatin induced a marked decrease of total and LDL cholesterol. During the combination therapy, decrease in triglycerides was greater than that found with fenofibrate alone, while the decrease in LDL cholesterol () was more pronounced than that observed with atorvastatin alone Kiortsis et al. (2000).
Fenofibrate formulation
Fenofibrate lowered triglyceride (TG) by 58% and increased HDL-C by 18%. NMR analysis exposed that VLDL, particularly large VLDL (), intermediate density lipoprotein (IDL) and small LDL, were considerably decreased, and LDL distribution shifted towards the larger particles (Ikewaki et al., Citation2003).
Ion exchange resins
Cholestyramine resin USP, used as an active ingredient, binds bile acids. This leads to replacement of bile acids () through increased metabolism of serum cholesterol resulting in lowered serum cholesterol levels (Pande et al., Citation2011).
Other common approaches for hyperlipidemia
The keystone of treatment for hyperlipidemia is dietary and lifestyle alteration, pursued by drug therapy, as requisite. Hyperlipidemia should not be conceived refractory to dietary treatment if the therapeutic treatment included animal products or more than minimal amounts of vegetable oils. These diets do not lower LDL cholesterol concentrations as effectively as high-fiber, low-fat diets that keep out animal products. depicts various common approaches for the management of hyperlipidemia.
Figure 3. Common approaches for hyperlipidemia.

Veritable exercise can improve lipid concentrations. Physical activities such as walking lower triglyceride concentrations by an average of 10 mg/dl, even as raising HDL by 5 mg/dl. More arduous activity may have greater effects (Hata & Nakajima, Citation1999). Patients with familial hypercholesterolemia usually require medication starting in early childhood.
More changes in significant diet appear to produce better results. Vegetarian (particularly vegan) diets that are free of cholesterol and very low in saturated fat reduce LDL cholesterol by 17–40%, with the strongest effects seen when the diet is combined with exercise (Ornish et al., Citation1998; Barnard et al., Citation2000). Reducing saturated fat, total fat and cholesterol ingestion also lowers triglyceride levels by ∼20% (Pelkman et al., Citation2004).
There are a lot of medications available to help lower elevated levels of triglycerides and LDL cholesterol, but for increasing HDL cholesterol is only a few are demonstrated. Each category of medication targets a specific lipid and varies in how the medication works, how effective it is for treatment, and how much costs of this. Your healthcare provider will recommend a medication or combination of medications based on blood lipid levels and other individual factors. To increase the lipid lowering activities of these medications, various approaches are carried out that increased metabolism of serum cholesterol, improved the solubility of the drug, increased HDL cholesterol level and improved drug delivery, effective in sustaining cholesterol lowering effect for extended periods at lower dose.
Ion exchange resins
Ion exchange resins are water-insoluble, cross-linked, polymer-carrying, ionizable functional groups. They contain acidic or basic functional groups and have the power to exchange counter-ions within aqueous solutions surrounding them (Srikanth et al., Citation2010). Drugs can be loaded onto the resins by an exchanging reaction. Therefore, a drug–resin complex (drug resinate) is formed.
Cholestyramine resin USP used as an active ingredient binds with bile acids contributes to replacement of bile acids through increased metabolism of serum cholesterol leading to lowered serum cholesterol levels (Pande et al., Citation2011).
Coencapsulated antioxidant nanoparticles
Obesity is common risk factor for type 2 diabetes with hyperlipidemia as one of its complications and in such conditions antioxidants were found to be beneficial. Ratnam et al. examined improvement in bioavailabilty and reduction of dose by co-encasulating combination of antioxidants, ellagic acid and coenzyme Q10 into nanoparticles and study the synergism effect in improving hyperlipidemia in high-fat diet-fed rats. The co-encapsulated particles at 10% (w/w of polymer) loading of ellagic acid and coenzyme Q10 have particle size of 260 nm. The high-fat diet-induced hyperlipidemic rats treated with antioxidant combination administered as oral suspension or nanoparticles found to improve the hyperlipidemic conditions and nanoparticles were determined to be equally/more effective in sustaining cholesterol lowering effect for extended periods at three times lower dose, improving endothelial functioning and in lowering glucose and triglycerides, demonstrating the ability of the nanoparticles in improving efficacy of the combination (Ratnam et al., Citation2009).
Reduction in cell adhesion
Diabetes mellitus is associated with high plasma triglyceride levels and reduction in HDL cholesterol, and a high frequency of CDV. HMG–coenzymeA reductase inhibitors and fibrates are mostly used in the treatment of diabetic dyslipidemia.
Jean-Charles Hogue et al. compared the effects of atorvastatin and fenofibrate on the cell adhesion, inflammation and oxidation markers in type 2 diabetes mellitus subjects with hypertriglyceridemia. Atorvastatin leads to reduction in TG, apo B, total C and LDL-C and to increase HDL-C whereas fenofibrate reduced plasma levels of apo B, total C and TG but was associated with a significant increase in LDL-C in these patients. In addition to the predictable changes in lipid values, the present study demonstrated that atorvastatin was potent to reduce cell adhesion, inflammation and oxidation markers, whereas fenofibrate having little effects on these markers (Hogue et al., Citation2008).
Mucoadhesive microparticles
An ideal oral-controlled drug delivery system delivers the drug at a predetermined rate, systematically or locally for a determined period of time (Kumar et al., Citation2012a). Simvastatin (SV) is a cholesterol-lowering agent that is synthetically derivated from a fermentation product of Aspergillus terreus and is extensively used to treat hypercholesterolemia. Microcapsules of simvastatin were prepared by complexation, and thus included this complex in the polymeric matrix by the use of orifice gelation technique resulted in more improved drug delivery in hypercholesterolemia (Bal et al., Citation2012).
Therapeutic gene targeting
Cardiovascular diseases are the principal cause of morbidity and mortality worldwide. So, new therapeutic approaches are still demanded. In the gene therapy field, RNA interference (RNAi) and regulation of microRNAs (miRNAs) have presumed a lot of attention in addition to traditional overexpression-based schemes. Here, recent determinations in therapeutic gene silencing and modulation of small RNA expression connected to atherogenesis and dyslipidemia are resumed. Novel gene therapy approaches for the treatment of hyperlipidemia have been directed. New therapies for lowering lipid levels are now being tested in clinical trials, and both RNAi-based and antisense oligonucleotide therapies have revealed promising results in lower in cholesterol levels (Mäkinen & Ylä-Herttuala, Citation2013).
Nanosponge
Resveratrol is a polyphenolic phytoalexin that is found in free and conjugated form. Extracts of plants namely grape juice, mulberries and peanuts are found to have its high concentration (Lamuela-Raventos et al., Citation1995; Romero-Pérez et al., Citation1999). From a very long time, these extracts are used in the treatment of several diseases like inflammation, CDVs, gonorrhea, dermatitis, fever and hyperlipidemia (Haunstetter & Izumo, Citation1998; Bertacche et al., Citation2006). Ansari et al. concluded that resveratrol-loaded NS are of suitable particle size obtained by conventional inclusion complexation techniques. All characterization results shows that the drug is encapsulated within the matrix in the cyclodextrin chains. This nanosponge-based formulation exhibited significantly better permeation, stability. This means it is possible to administer resveratrol NS complex as buccal delivery and topical application (Ansari et al., Citation2011).
Self-emulsifying drug delivery system
Granules after self-emulsification were formulated with the objective of improving the bioavailability of the ezetimibe and simvastatin when administered together. Optimization of self-nanoemulsifying system (SNS) was done by using different composition of a variety of modified oils, surfactant and cosurfactant mixtures. Self-nanoemulsifying granules accomplished considerable increase in dissolution of the drugs as compared with pure powder of drugs. In vivo evaluation in rats expressed major decrease in the triglyceride levels and total cholesterol levels in rats (Dixit & Nagarsenker, Citation2008).
Suppress cellular uptake
This study demonstrated that monocytes freshly isolated from human blood take up Ox-LDL during their differentiation into macrophages at regular increasing rate, and this process is extensively enhanced in hypercholesterolemic patients. Therapy of atorvastatin in hypercholesterolemic patients for 1 month inhibits the enhanced upregulation of Ox-LDL uptake by differentiating monocytes, down to levels noticed in control subjects, and this was linked with reduced gene expression of the CD36, SRA-I and SRA-II scavenger receptors (Fuhrman et al., Citation2002). In accordance with these data, enhanced scavenger receptor mRNA expression in monocytes during their differentiation into macrophages was confirmed in dialysis patients (Ando et al., Citation1996) and increased gene expression of scavenger receptor A type I was found in hyperlipidemic patients (Villanova et al., Citation1996). Atorvastatin therapy in hypercholesterolemic patients inhibits the upregulation in scavenger receptors CD36, SRA-I and SRA-II expression and function that occurs during monocytes differentiation into macrophages, in equivalent to its hypocholesterolemic and antioxidative effect.
Oxidatively modified LDLs
The elevated level of plasma LDL in hyperlipidemic patients is a major cause for the production of atherosclerosis. Plasma LDL must be modified before it can produce damage of endothelium-dependent relaxation in aortic rings or enhancement of uptake by macrophages. The remarkable increase in lysophosphatidylcholine (IysoPC) content in oxidatively modified LDL has been detected as an important biochemical factor for the impairment of endothelium dependent relaxation. This study was designed to examine the effect of oxidatively modified LDL from normal and hyperlipidemic patients on endothelium-dependent relaxation. It was predicted that high levels of total cholesterol, LDL cholesterol and triglyceride were detected in the plasma of hyperlipidemic patients. It is practical to conclude that the higher level of the long-chain moiety found in these patients is responsible for its enhanced ability to impair endothelium-dependent relaxation of the vascular preparation. Chen et al. proposed that the high level of LDL found in the plasma of hyperlipidemic patients, linked with the enhanced ability to generate long-chain species of lysoPC during oxidative modification, and are important factors that contribute to the development of atherosclerosis in these patients (Chen et al., Citation1997).
Solid dispersion
Solid dispersions have been extensively used to improve the solubility, dissolution rate, absorption as well as bioavailability of poor water-soluble drugs. Fenofibrate compound are practically insoluble in water due to their high lipophilicity, and thus the dissolution rate of fenofibrate is omened to limit its absorption from the gastrointestinal tract. The solid dispersion of the fenofibrate were prepared by spray-drying technique using Poloxamer 188 as carrier and tocopheryl polyethylene glycol succinate (TPGS) as surfactant expressed maximum solubility enhancement of fenofibrate (Bhise, Citation2011). Solid dispersion has been used to enhance the dissolution of Ezetimibe along with an adsorption technique that employed a water-soluble adsorbent for low-soluble drug, which leads to combined effect of hydrophilic carriers and increased surface area (Parmar et al., Citation2011).
Nanosuspension
Nanosuspension is a submicron colloidal dispersion of drug particles that are stabilized by surfactants and are produced by suitable methods. The reduction of drug particles into the sub-micron range adds to a major increase in the dissolution rate and therefore enhances bioavailability (Chingunpituk, Citation2011). A pharmaceutical nanosuspension can be defined as the nano-sized (usually lies between 200 and 600 nm) drug particle which is finely dispersed in an aqueous vehicle for either oral and topical use or pulmonary and parenteral administration. Fenofibrate is a nanosuspension presently marketed in the name of Tricor® (Abbott Laboratories, Chicago, IL, USA) (Malakar, Citation2012). Nanosuspensions utilize some techniques to minimize the particle size to the nano level which help to improve the solubility of the drug due to small particle size.
Reduce intestinal cholesterol absorption
It was concluded that 2 weeks of treatment with ezetimibe at 10 mg/day produced a 54% inhibition of cholesterol absorption in hypercholesterolemic subjects. This was related with increase in endogenous cholesterol synthesis and reductions in total cholesterol, LDL and plant sterol concentrations.
The effect of ezetimibe (10 mg/day) on cholesterol synthesis and absorption, sterol excretion and plasma concentrations of cholesterol and non-cholesterol sterols were inquired in randomized, double-blinded, placebo-controlled, crossover study in 18 patients with mild to moderate hypercholesterolemia (Sudhop et al., Citation2002).
Injection
Danhong injection (DHI), a Chinese medical product extracted from Radix et Rhizoma Salviae Miltiorrhizae has been reported to have anti-inflammatory, anti-oxidative and anti-fibrinolytic properties and is widely used for the clinical treatment of CDV. This study aimed to investigate the preventive and therapeutic effects of DHI on hyperlipidemia. Rats treated with DHI had significantly reduced TG, TC, LDL-C and arteriosclerosis index (AI) (Chen et al., Citation2014).
N-acyl-1-amino-2-alcohols
An alkaloidal amide, i.e. Aegeline (V) isolated from the leaves of Aegle marmelos as a dual acting agent (antihyperlipidemic and antihyperglycemic). In continuation of this program, Sarkar et al. synthesized new N-acyl-1-amino-2-alcohols (N-acrylated-1-amino-2-phenylethanol and N-acylated-1-amino-3-aryloxypropanols) via Ritter reaction and screened for their in vivo antihyperlipdemic activity in Triton-induced hyperlipidemia model, LDL oxidation and antioxidant activity. New N-acyl-1-amino-2-alcohols were synthesized and evaluated their antihyperlipdemic, LDL oxidation and antioxidant activity (Sarkar et al., Citation2014).
Polymorphism
The microsomal triglyceride transfer protein (MTP) is involved in hepatic and intestinal apoB secretion. Klop et al. studied the effect of the functional MTP−493G/T polymorphism on fasting and postprandial lipoproteins in patients with familial combined hyperlipidemia (FCH) before and after treatment with atorvastatin. Atorvastatin decreases postprandial TG in T-allele carriers with FCH (Klop et al., Citation2013).
MicroRNA-30c
Hyperlipidemia is a risk factor for various cardiovascular and metabolic disorders. Soh et al. show that microRNA-30c (miR-30c) interacts with the 3′ untranslated region of MTP mRNA and induces its degradation, leading to reductions in MTP activity and in apoB secretion; miR-30c also reduces lipid synthesis independently of MTP. Hepatic overexpression of miR-30c reduced hyperlipidemia in Western diet-fed mice by decreasing lipid synthesis and the secretion of triglyceride-rich apoB-containing lipoproteins and decreased atherosclerosis in Apoe mice (Soh et al., Citation2013).
Dietary supplements
A new, fast-screening method for the identification of various pharmacologically active ingredients in cholesterol-lowering dietary supplements using direct injection mass spectrometry was developed. According to the obtained results, it is apparent that cholesterol-lowering dietary supplements are poorly standardized, as two samples did not contain active ingredients (monacolin K, monacolin K acid form and cynarin). Moreover, the application of the proposed direct injection method to quality control of cholesterol-lowering dietary supplements may be proposed for the routine analysis of a large number of samples in the laboratories of regulatory agencies (Sertić et al., Citation2014).
Applications of nanotechnology
In pharmaceuticals
In the last decade, engineered nanoparticles have become an imperative class of new materials with a number of properties that make them extremely attractive for commercial development. In fact, they have been more and more used for manufacturing various industrial items such as clothes or cosmetics and for infinite applications in aerospace, computer and electronics industry. Additionally, as the need for the development of new medicines is urging and given the underlying nanoscale functions of the biological components of living cells, nanotechnology has been utilized to different medical fields such as oncology and cardiovascular medicine. Really, nanotechnology is being used to improve discovery of molecular diagnostics, biomarkers, drug discovery and drug delivery, which could be appropriate to management of these patients (Jain, Citation2005).
In diagnosis, pharmacology and therapy
Nanotechnology is being employed to biomarker-based proteomics and genomics technologies. Nanoparticles can be applied for qualitative or quantitative in vivo or ex vivo diagnosis by focusing, amplifying and protecting a biomarker from degradation, in sort to provide more sensitive analysis (Geho et al., Citation2004).
Molecular diagnosis
Nowadays, imaging diagnosis is not only inadequate to a complete description of anatomic structures, but can also involve imaging of cellular signaling. Nanoparticles are presently being tested for molecular imaging in order to attain a more accurate diagnosis with high-quality images (Kraitchman et al., Citation2003).
Nanoparticle drug delivery systems
The use of pharmacological agents developed by classical strategies of pharmacological development is often limited by pharmacokinetics and pharmacodynamics problems such as low efficacy or lack of selectivity. discusses different applications of nanoparticles.
Table 6. Different applications of nanoparticles.
Conclusion
Nanoparticles-based technology surely enhanced the properties of less water-soluble drugs (BCS Class II), namely, drug loading efficiency; improve solubility and absorption of drugs, less toxicity, maximum concentration in plasma and also improvement of bioavailabilty.
Some of the characteristics for lipophilic drug, e.g. diffusion through membranes, release properties (sustained, controlled) and target specificity, must be improved by quantified selection of the lipidic material. SLNs and nanolipid carriers are some of the extensive carriers utilized in drug delivery system. Among these nanolipid carriers, “nanostructured lipid carriers” are currently used carrier system and have a variety of advantages over the other carriers, such as – eminent drug loading capacity, bettered release characteristics and multiple incorporation of drugs, thus it can be sure that nano-aided drug delivery system is an appropriate choice for poorly water-soluble lipophilic drugs.
However contempt the fast progress, there has been so far no nanoparticles therapeutics that is so developed to fulfill clinical standards. Every nanoplatform has its own promises and advantages, but meanwhile has its disadvantages to overcome. These include particles aggregation, physical handling is difficult in case of liquid and dry form, limited drug loading and toxic metabolites may form. Efforts of address each of these issues are going on, and should remain the focus on the future studies. The fundamental applications of nanoparticles in medicine are diagnosis and target therapy; however their wider use in still the future.
Future prospectives
Nanomedicines has shown enormous therapeutic potency to treat a variety of diseases for both research and clinical application, several nanoparticulate formulations, such as Tricor® by Abbott Laboratories (Chicago, IL, USA) is second nanoparticles technology-based product approved by FDA, an improved fenofibrate formulation (for hyperlipidemia) that reduced the fed-fast variability resulting in no dosing restriction that permits co-administration with other drugs used for treating lipid disorders.
Another product containing Fenofibrate nanoparticles is Triglide®, developed by Skype Pharma (London, UK) using their patented IDD-P® technology and marketed by Sciele Pharma Inc (Atlanta, GA, USA) (Till et al., Citation2005).
Nanoparticles are one of the novel drug delivery system, which can be of prospective use in targeting and controlling drug delivery as well as in paints and cosmetics textiles. Judging by the current concern and previous success, nanoparticulate drug delivery system seems to be viable and promising strategy for the biopharmaceutical industry.
Acknowledgements
Authors are thankful to Mr. Praveen Garg, Chairman, ISF College of Pharmacy, Moga, Punjab, for his continuous support and encouragement.
Declaration of interest
The authors have declared no conflict of interest.
References
- Aggarwal P, Hall JB, McLeland CB, et al. (2009). Nanoparticle interaction with plasma proteins as it relates to particle biodistribution, biocompatibility and therapeutic efficacy. Adv Drug Deliv Rev 61:428–37
- Agrawal A, Deo R, Wang GD, et al. (2008). Nanometer-scale mapping and single-molecule detection with color-coded nanoparticle probes. Proc Natl Acad Sci 105:3298–303
- Allen TM, Cullis PR. (2004). Drug delivery systems: entering the mainstream. Science 303:1818–22
- Ando M, Lundkvist I, Bergstrom J, Lindholm B. (1996). Enhanced scavenger receptor expression in monocyte-macrophages in dialysis patients. Kidney Int 49:773–80
- Ansari KA, Vavia PR, Trotta F, Cavalli R. (2011). Cyclodextrin-based nanosponges for delivery of resveratrol: in vitro characterisation, stability, cytotoxicity and permeation study. Aaps Pharmscitech 12:279–86
- Ausar S, Morcillo M, Leon A, et al. (2003). Improvement of HDL-and LDL-cholesterol levels in diabetic subjects by feeding bread containing chitosan. J Med Food 6:397–9
- Bal T, Murthy PN, Sengupta S. (2012). Preparation and evaluation of mucoadhesive simvastatin microcapsules using orifice gelation technique. Asian J Pharm 6:74–84
- Barnard ND, Scialli AR, Bertron P, et al. (2000). Effectiveness of a low-fat vegetarian diet in altering serum lipids in healthy premenopausal women. Am J Cardiol 85:969–72
- Bathool A, Vishakante GD, Khan MS, Shivakumar H. (2012). Development and characterization of atorvastatin calcium loaded chitosan nanoparticles for sustain drug delivery. Adv Mater Lett 3:466–70
- Bertacche V, Lorenzi N, Nava D, et al. (2006). Host–guest interaction study of resveratrol with natural and modified cyclodextrins. J Incl Phenom Macrocycl Chem 55:279–87
- Bhise SD. (2011). Ternary solid dispersions of fenofibrate with Poloxamer 188 and TPGS for enhancement of solubility and bioavailability. Int J Res Pharm Biomed Sci 2:583–95
- Brahm A, Hegele RA. (2013). Hypertriglyceridemia. Nutrients 5:981–1001
- Brook RD, Franklin B, Cascio W, et al. (2004). Air pollution and cardiovascular disease A statement for healthcare professionals from the expert panel on population and prevention science of the American Heart Association. Circulation 109:2655–71
- Chan WC, Nie S. (1998). Quantum dot bioconjugates for ultrasensitive nonisotopic detection. Science 281:2016–18
- Chen C-C, Tsai T-H, Huang Z-R, Fang J-Y. (2010). Effects of lipophilic emulsifiers on the oral administration of lovastatin from nanostructured lipid carriers: physicochemical characterization and pharmacokinetics. Eur J Pharm Biopharm 74:474–82
- Chen J, Deng J, Zhang Y, et al. (2014). Lipid-lowering ef fects of Danhong injection on hyperl ipidemia rats. J Ethnopharmacol pii: S0378-8741(14)00298-0. doi: 10.1016/j.jep.2014.04.023
- Chen L, Liang B, Froese D, et al. (1997). Oxidative modification of low density lipoprotein in normal and hyperlipidemic patients: effect of lysophosphatidylcholine composition on vascular relaxation. J Lipid Res 38:546–53
- Chingunpituk J. (2011). Nanosuspension technology for drug delivery. Walailak J Sci Technol 4:139–53
- Cho K, Wang X, Nie S, Shin DM. (2008). Therapeutic nanoparticles for drug delivery in cancer. Clin Cancer Res 14:1310–16
- Colletti RB, Roff NK, Neufeld EJ, et al. (1993). Niacin treatment of hypercholesterolemia in children. Pediatrics 92:78–82
- Dailey L, Jekel N, Fink L, et al. (2006). Investigation of the proinflammatory potential of biodegradable nanoparticle drug delivery systems in the lung. Toxicol Appl Pharmacol 215:100–8
- Davis ME, Shin DM. (2008). Nanoparticle therapeutics: an emerging treatment modality for cancer. Nat Rev Drug Discov 7:771–82
- De La Isla A, Brostow W, Bujard B, et al. (2003). Nanohybrid scratch resistant coatings for teeth and bone viscoelasticity manifested in tribology. Mater Res Innov 7:110–14
- Deepa P, Varalakshmi P. (2005). Atheroprotective effect of exogenous heparin-derivative treatment on the aortic disturbances and lipoprotein oxidation in hypercholesterolemic diet fed rats. Clin Chim Acta 355:119–30
- Dixit RP, Nagarsenker M. (2008). Formulation and in vivo evaluation of self-nanoemulsifying granules for oral delivery of a combination of ezetimibe and simvastatin. Drug Dev Ind Pharm 34:1285–96
- Dobrovolskaia MA, Aggarwal P, Hall JB, McNeil SE. (2008). Preclinical studies to understand nanoparticle interaction with the immune system and its potential effects on nanoparticle biodistribution. Mol Pharm 5:487–95
- Edelstein R, Tamanaha C, Sheehan P, et al. (2000). The BARC biosensor applied to the detection of biological warfare agents. Biosens Bioelectron 14:805–13
- Ehnholm C, Investigators DAIS. (2001). Effect of fenofibrate on progression of coronary-artery disease in type 2 diabetes: the Diabetes Atherosclerosis Intervention Study, a randomised study. Lancet 357:905–10
- Emerich DF, Thanos CG. (2006). The pinpoint promise of nanoparticle-based drug delivery and molecular diagnosis. Biomol Eng 23:171–84
- Fuhrman B, Koren L, Volkova N, et al. (2002). Atorvastatin therapy in hypercholesterolemic patients suppresses cellular uptake of oxidized-LDL by differentiating monocytes. Atherosclerosis 164:179–85
- Gao X, Cui Y, Levenson RM, et al. (2004). In vivo cancer targeting and imaging with semiconductor quantum dots. Nat Biotechnol 22:969–76
- Geho DH, Lahar N, Ferrari M, et al. (2004). Opportunities for nanotechnology-based innovation in tissue proteomics. Biomed Microdev 6:231–9
- Giepmans BN, Deerinck TJ, Smarr BL, et al. (2005). Correlated light and electron microscopic imaging of multiple endogenous proteins using Quantum dots. Nat Methods 2:743–9
- Hata Y, Nakajima K. (1999). Life-style and serum lipids and lipoproteins. J Atheroscler Thromb 7:177–97
- Haunstetter A, Izumo S. (1998). Apoptosis basic mechanisms and implications for cardiovascular disease. Circ Res 82:1111–29
- Hegele RA. (2009). Plasma lipoproteins: genetic influences and clinical implications. Nat Rev Genet 10:109–21
- Hegele RA, Ban MR, Hsueh N, et al. (2009). A polygenic basis for four classical Fredrickson hyperlipoproteinemia phenotypes that are characterized by hypertriglyceridemia. Human Mol Genet 18:4189–94
- Hogue J-C, Lamarche B, Tremblay AJ, et al. (2008). Differential effect of atorvastatin and fenofibrate on plasma oxidized low-density lipoprotein, inflammation markers, and cell adhesion molecules in patients with type 2 diabetes mellitus. Metabolism 57:380–6
- Huang L, Peng Z, Guo Y, Porter AL. (2010). Identifying the emerging roles of nanoparticles in biosensors. J Bus Chem 7:15–30
- Ikewaki K, Tohyama J-I, Nakata Y, et al. (2003). Fenofibrate effectively reduces remnants, and small dense LDL, and increases HDL particle number in hypertriglyceridemic men – a nuclear magnetic resonance study. J Atheroscler Thromb 11:278–85
- Ito A, Shinkai M, Honda H, Kobayashi T. (2005). Medical application of functionalized magnetic nanoparticles. J Biosci Bioeng 100:1–11
- Jain K. (2005). Role of nanobiotechnology in developing personalized medicine for cancer. Technol Cancer Res Treat 4:645–50
- Joshi N, Grinstaff M. (2008). Applications of dendrimers in tissue engineering. Curr Top Med Chem 8:1225–36
- Kim M-S, Jin S-J, Kim J-S, et al. (2008). Preparation, characterization and in vivo evaluation of amorphous atorvastatin calcium nanoparticles using supercritical antisolvent (SAS) process. Eur J Pharm Biopharm 69:454–65
- Kiortsis D, Millionis H, Bairaktari E, Elisaf M. (2000). Efficacy of combination of atorvastatin and micronised fenofibrate in the treatment of severe mixed hyperlipidemia. Eur J Clin Pharmacol 56:631–5
- Klop B, Verseyden C, Ribalta J, et al. (2013). MTP gene polymorphisms and postprandial lipemia in familial combined hyperlipidemia: effects of treatment with atorvastatin. Clín Investig Arterioscler 26:49–57
- Kolovou GD, Anagnostopoulou K, Cokkinos DV. (2005). Pathophysiology of dyslipidemia in the metabolic syndrome. Postgrad Med J 81:358–66
- Kontush A, Chapman MJ. (2006). Functionally defective high-density lipoprotein: a new therapeutic target at the crossroads of dyslipidemia, inflammation, and atherosclerosis. Pharmacol Rev 58:342–74
- Kraitchman DL, Heldman AW, Atalar E, et al. (2003). In vivo magnetic resonance imaging of mesenchymal stem cells in myocardial infarction. Circulation 107:2290–3
- Kreuter J. (1994). Colloidal drug delivery systems. New York: CRC Press
- Kumar KS, Bhowmik D, Srivastava S, et al. (2012a). Sustained release drug delivery system potential. Pharm Innov 1:48–60
- Kumar PP, Gayatri P, Sunil R, et al. (2012b). Atorvastatin loaded solid lipid nanoparticles: formulation, optimization, and in vitro characterization. Int Organ Sci Res J Pharm 2:23–32
- Kwiterovich PO Jr. (1998). State-of-the-art update and review: clinical trials of lipid-lowering agents. Am J Cardiol 82:3U–17U
- Lamuela-Raventos RM, Romero-Perez AI, Waterhouse AL, De La Torre-Boronat MC. (1995). Direct HPLC analysis of cis-and trans-resveratrol and piceid isomers in Spanish red Vitis vinifera wines. J Agric Food Chem 43:281–3
- LaVan DA, Lynn DM, Langer R. (2002). Moving smaller in drug discovery and delivery. Nat Rev Drug Discov 1:77–84
- Mahtab R, Rogers JP, Murphy CJ. (1995). Protein-sized quantum dot luminescence can distinguish between “straight”, “bent”, and “kinked” oligonucleotides. J Am Chem Soc 117:9099–100
- Maki KC, Orloff DG, Nicholls SJ, et al. (2013). A highly bioavailable omega-3 free fatty acid formulation improves the cardiovascular risk profile in high-risk, statin-treated patients with residual hypertriglyceridemia (the ESPRIT trial). Clin Ther 35:1400–11. e1403
- Mäkinen PI, Ylä-Herttuala S. (2013). Therapeutic gene targeting approaches for the treatment of dyslipidemias and atherosclerosis. Curr Opin Lipidol 24:116–22
- Malakar J. (2012). Nanosuspension: a nano-heterogeneous carrier for drug delivery system. Int J Pharm Biol Arch 3:4–13
- Maximov V, Reukov V, Barry J, et al. (2010). Protein–nanoparticle conjugates as potential therapeutic agents for the treatment of hyperlipidemia. Nanotechnology 21:265103. http://iopscience.iop.org/0957-4484/21/26/265103/pdf/0957-4484_21_26_265103.pdf
- McCrindle BW, Ose L, Marais AD. (2003). Efficacy and safety of atorvastatin in children and adolescents with familial hypercholesterolemia or severe hyperlipidemia: a multicenter, randomized, placebo-controlled trial. J Pediatr 143:74–80
- Meena A, Ratnam DV, Chandraiah G, et al. (2008). Oral nanoparticulate atorvastatin calcium is more efficient and safe in comparison to Lipicure® in treating hyperlipidemia. Lipids 43:231–41
- Mittal G, Chandraiah G, Ramarao P, Kumar MR. (2009). Pharmacodynamic evaluation of oral estradiol nanoparticles in estrogen deficient (ovariectomized) high-fat diet induced hyperlipidemic rat model. Pharm Res 26:218–23
- Nair R, Varghese SH, Nair BG, et al. (2010). Nanoparticulate material delivery to plants. Plant Sci 179:154–63
- Nam J-M, Thaxton CS, Mirkin CA. (2003). Nanoparticle-based bio-bar codes for the ultrasensitive detection of proteins. Science 301:1884–6
- Ohno K, Mori C, Akashi T, et al. (2013). Fabrication of contrast agents for magnetic resonance imaging from polymer-brush-afforded iron oxide magnetic nanoparticles prepared by surface-initiated living radical polymerization. Biomacromolecules 14:3453–62
- Ornish D, Scherwitz LW, Billings JH, et al. (1998). Intensive lifestyle changes for reversal of coronary heart disease. JAMA 280:2001–7
- Ostanina E, Varlamov V, Yakovlev G. (2008). Inhibition of lipase activity by low-molecular-weight chitosan. Appl Biochem Microbiol 44:32–7
- Pande S, Kshirsagar M, Chandewar A. (2011). Ion exchange resins pharmaceutical applications and recent advancement. Int J Adv Pharm Sci 2:8–16
- Pankhurst QA, Connolly J, Jones S, Dobson J. (2003). Applications of magnetic nanoparticles in biomedicine. J Phys D Appl Phys 36:R167–R181
- Parak WJ, Boudreau R, Le Gros M, et al. (2002). Cell motility and metastatic potential studies based on quantum dot imaging of phagokinetic tracks. Adv Mater 14:882–885
- Parmar KR, Shah SR, Sheth NR. (2011). Studies in dissolution enhancement of ezetimibe by solid dispersions in combination with a surface adsorbent. Dissolut Technol 18:55–61
- Peer D, Karp JM, Hong S, et al. (2007). Nanocarriers as an emerging platform for cancer therapy. Nat Nanotechnol 2:751–60
- Pelkman CL, Fishell VK, Maddox DH, et al. (2004). Effects of moderate-fat (from monounsaturated fat) and low-fat weight-loss diets on the serum lipid profile in overweight and obese men and women. Am J Clin Nutr 79:204–12
- Prasad K, Kalra J. (1993). Oxygen free radicals and hypercholesterolemic atherosclerosis: effect of vitamin E. Am Heart J 125:958–73
- Ratnam DV, Chandraiah G, Meena A, et al. (2009). The co-encapsulated antioxidant nanoparticles of ellagic acid and coenzyme Q 10 ameliorates hyperlipidemia in high fat diet fed rats. J Nanosci Nanotechnol 9:6741–6
- Reiner Z, Tedeschi-Reiner E. (2006). Th-W47: 2 Atherosclerosis – a paradox of Eastern European countries. Atheroscler Suppl 7:461. doi: 10.1016/S1567-5688(06)81854-4
- Romero-Pérez AI, Ibern-Gómez M, Lamuela-Raventós RM, de la Torre-Boronat MC. (1999). Piceid, the major resveratrol derivative in grape juices. J Agric Food Chem 47:1533–6
- Rozman D, Monostory K. (2010). Perspectives of the non-statin hypolipidemic agents. Pharmacol Ther 127:19–40
- Sahoo SK, Labhasetwar V. (2003). Nanotech approaches to drug delivery and imaging. Drug Discov Today 8:1112–20
- Sarkar S, Sonkar R, Bhatia G, Tadigoppula N. (2014). Synthesis of new N-acryl-1-amino-2-phenylethanol and N-acyl-1-amino-3-aryloxypropanols and evaluation of their antihyperlipidemic, LDL-oxidation and antioxidant activity. Eur J Med Chem 80:135–44
- Sathali H, Abdul A, Nisha N. (2013). Development of solid lipid nanoparticles of rosuvastatin calcium. J Pharm Res 6:536–48
- Seenivasan A, Panda T, Théodore T. (2011). Lovastatin nanoparticle synthesis and characterization for better drug delivery. Open Biotechnol J 5:28–32
- Sertić M, Mornar A, Nigović B. (2014). A rapid profiling of hypolipidemic agents in dietary supplements by direct injection tandem mass spectrometry. J Food Composit Anal 34:68–74
- Shepherd J. (1989). Mechanism of action of bile acid sequestrants and other lipid-lowering drugs. Cardiology 76:65–74
- Simons LA. (2002). Additive effect of plant sterol-ester margarine and cerivastatin in lowering low-density lipoprotein cholesterol in primary hypercholesterolemia. Am J Cardiol 90:737–40
- Singh I, Rehni A, Kalra R, et al. (2008). Dendrimers and their pharmaceutical applications a review. Die Pharm Int J Pharm Sci 63:491–6
- Slack J. (1969). Risks of ischaemic heart-disease in familial hyperlipoproteinaemic states. The Lancet 294:1380–2
- Soh J, Iqbal J, Queiroz J, et al. (2013). MicroRNA-30c reduces hyperlipidemia and atherosclerosis in mice by decreasing lipid synthesis and lipoprotein secretion. Nat Med 19:892–900
- Srikanth M, Sunil S, Rao N, et al. (2010). Ion-exchange resins as controlled drug delivery carriers. J Sci Res 2:597–611
- Staels B, Dallongeville J, Auwerx J, et al. (1998). Mechanism of action of fibrates on lipid and lipoprotein metabolism. Circulation 98:2088–93
- Starc TJ. (2001). Management of hyperlipidemia in children. Prog Pediatr Cardiol 12:205–13
- Sudhop T, Lütjohann D, Kodal A, et al. (2002). Inhibition of intestinal cholesterol absorption by ezetimibe in humans. Circulation 106:1943–8
- Sukanya M, Kishore VS. (2012). Design and development of chronopharmaceutical drug delivery of simvastatin. J Chem Pharm Res 4:3195–200
- Sun M, Zhai X, Xue K, et al. (2011). Intestinal absorption and intestinal lymphatic transport of sirolimus from self-microemulsifying drug delivery systems assessed using the single-pass intestinal perfusion (SPIP) technique and a chylomicron flow blocking approach: linear correlation with oral bioavailabilities in rats. Eur J Pharm Sci 43:132–40
- Tao Y, Zhang H, Gao B, et al. (2011). Water-soluble chitosan nanoparticles inhibit hypercholesterolemia induced by feeding a high-fat diet in male Sprague–Dawley rats. J Nanomater 2011:6
- Till MC, Simkin MM, Maebius S. (2005). Nanotech meets the FDA: a success story about the first nanoparticulate drugs approved by the FDA, HeinOnline. Gale Group, Farmington Hills, Michigan
- van Lennep JER, Westerveld HT, Erkelens DW, van der Wall EE. (2002). Risk factors for coronary heart disease: implications of gender. Cardiovasc Res 53:538–49
- Villanova JG, Diéuez Lucena JL, Arcás NF, Engel AR. (1996). Increased expression of scavenger receptor type I gene in human peripheral blood from hyperlipidemic patients determined by quantitative additive RT-PCR. Biochim Biophys Acta Lipids Lipid Metab 1300:135–41
- Wang S, Mamedova N, Kotov NA, et al. (2002). Antigen/antibody immunocomplex from CdTe nanoparticle bioconjugates. Nano Lett 2:817–22
- Weissleder R, Elizondo G, Wittenberg J, et al. (1990). Ultrasmall superparamagnetic iron oxide: characterization of a new class of contrast agents for MR imaging. Radiology 175:489–93
- West JL, Halas NJ. (2000). Applications of nanotechnology to biotechnology: commentary. Curr Opin Biotechnol 11:215–17
- Witztum J. (1996). Drugs used in the treatment of hyperdyslipidemias. The pharmacological basis of therapeutics. New York: McGraw-Hill, 875–97
- Zhang H-L, Tao Y, Guo J, et al. (2011). Hypolipidemic effects of chitosan nanoparticles in hyperlipidemia rats induced by high fat diet. Int Immunopharmacol 11:457–61
- Zhang J, Liu J, Li L, Xia W. (2008). Dietary chitosan improves hypercholesterolemia in rats fed high-fat diets. Nutr Res 28:383–90
- Zhang Z, Bu H, Gao Z, et al. (2010). The characteristics and mechanism of simvastatin loaded lipid nanoparticles to increase oral bioavailability in rats. Int J Pharm 394:147–53