Abstract
Objective: Calorie restriction and intermittent fasting are two dietary interventions that can improve aging. Religious fasting also suggested having similar benefit; however, such studies are still scarce. Thus, this study aimed to determine the effect of fasting calorie restriction (FCR) on metabolic parameters and DNA damage among healthy older adult men.
Methods: A randomized controlled study was done on men, aged 50–70 years in Klang Valley, Malaysia. Subjects were divided into two groups; FCR (reduction of 300–500 kcal/d combined with 2 days/week of Muslim Sunnah Fasting) and control. Assessment was ascertained at three time point; baseline, weeks 6 and 12. Blood samples were analyzed for lipid profile, DNA damage and malondialdehyde (MDA).
Results: The FCR group reduced their energy intake for approximately 18% upon completion of the study. A significant interaction effect was found in body weight, body mass index, fat percentage, fat mass, blood pressure, total cholesterol, low-density lipoprotein cholesterol and the ratio of total cholesterol/high-density lipoprotein cholesterol (p < 0.05). A significant improvement (p < 0.001) in total DNA rejoining cells and MDA (p < 0.05) was also observed in the FCR group.
Conclusion: FCR improved metabolic parameters and DNA damage in healthy older adult men. Therefore, there is a need to further examine the mechanism of FCR.
Introduction
The number of people older than 65 years is expected to increase by more than 250% in many Asian countries such as Malaysia, Singapore, India, Bangladesh and Philippines [Citation1]. Following this trend, a higher prevalence of chronic diseases and cancers was expected [Citation2].
Aging in men is one of the biggest concerns in Asian countries, and the life expectancy in men is shorter than women in most regions of the world [Citation3]. In Malaysia, the life expectancy for men was about 71.9 years as compared to 77.0 years in women [Citation4]. Malaysian men’s health status was also reported to be poor [Citation5]. A study on aging men in Malaysia [Citation6] revealed that 66% of men were overweight and 70% of them were smokers. In agreement with previous studies, we believe that these problems were due to the physical and social environment factors that influence health behavior among men [Citation7–9].
Whilst there are growing numbers of health studies in men, the intervention that is aimed at promoting general well being is still scarce. Majority of the studies were focused on prostate cancer screening [Citation10]. Thus, there is a need to formulate an interventional study that is feasible to improve men’s health.
Fasting calorie restriction (FCR) is a new nutrition intervention model, aimed to promote a feasible way of controlling eating. The regime was derived from the idea of Comprehensive Assessment of Long Term Effect of Reducing Intake of Energy and Alternate Day Fasting (ADF) studies. calorie restriction (CR) has been shown to improve the biomarkers of longevity [Citation11] and produce numerous health benefits. On the other hand, ADF; the alternative way of practicing CR was also suggested having similar effects [Citation12].
Acknowledging the difficulties of practicing CR and ADF in free living people, we develop a regime, which is feasible to be conducted in Malaysia’s Muslim population. We combined both CR and two days of Muslim Sunnah (the practice of Prophet Muhammad) fasting in a week for 3 months. The pilot study [Citation13] suggested that FCR is feasible and may improve nutritional and quality of life. In this study, we hypothesized that FCR may also improve metabolic parameters and DNA damage among aging men.
Materials and methods
Subjects
Subjects participated in this study were recruited among Malay men residing in Klang Valley, Malaysia. The criteria of inclusion were healthy (non-diabetic and no history of cardiovascular disease) Malay man aged 50–70 years had a body mass index (BMI) of 23.0–29.9 kg/m2 with no history of mental or physical disabilities. Subjects should also not be practicing Muslim Sunnah fasting or had changed their dietary pattern three months before the study. Eligible subjects were approached to participate. Only those who agreed to participate were explained of all the information pertaining to this study and were consented. This study was approved by Universiti Kebangsaan Malaysia, Medical Centre research board.
Study design
A randomized controlled study was carried out to determine the efficacy of FCR in metabolic parameters among healthy older Malay adults. Subjects were randomly assigned into two groups; FCR and control (CO) group. Those who were assigned to the FCR group needed to adhere to the FCR dietary regime, which consisted of two days of Muslim Sunnah fasting combined with a reduction of 300–500 kcal/d from the habitual energy intake for a three-month intervention period. During fasting day, subjects needed to take a light meal before sunrise (Sahur), no food and drink on the day was allowed (approximately for 13 h) and a complete meal after sunset (Iftar). During fasting day, smoking was also forbidden. On the other days, subjects must reduce their dietary intake by 500 kcal/d. Subjects were also provided with seven-day food menu guidelines. Those who were assigned to the CO group need to maintain their present lifestyle. Analysis was carried out at three time points: baseline, week 6 and week 12.
In order to ensure good compliance, FCR subjects were contacted once a week via telephone calls. Family members, especially the spouse, were also interviewed to obtain information regarding subjects’ dietary intake. Fasting log book and food diaries were provided to the subjects during each assessment meeting. Subjects were given detailed instruction verbally and a reference guide on how to fill the food diaries. Individual and group counseling were provided before and during the intervention period. Study design and development of the regime has been discussed previously (Teng et al. 2011).
Body composition
Height was measured using SECA-213 portable stadiometer (SECA, Hamburg, Germany). Body composition was measured using TANITA BC-418, body composition analyzer (TANITA Corp. Tokyo, Japan). All measurements were made in the morning at subjects’ fasted state. This instrument was calibrated each time before measurement. Data from this instrument including body weight, BMI, body fat percentage, fat mass, fat free mass and total body water.
Biochemical markers
A total of 20 ml venous blood was collected following eight hours of fasting in the morning for measurement of lipid profile, oxidative stress (plasma malondialdehyde) and DNA damage. Lipid profile was analyzed using chemiluminescent immunoassay with Siemens Advia 2400 (Japan).
Plasma malondialdehyde (MDA) was used to determine oxidative stress using high-performance liquid chromatography (HPLC), based on derivatization of MDA with 2,4-dinitrophenylhydrazine (DNPH) (Sigma-Aldrich, St Louis, MO) as described by Pilz et al. [Citation14] with slight modifications.
The sample was prepared by mixing with 200 µl of 1.3 M sodium hydroxide in the Eppendorf tube. The sample mixture was then incubated in a water bath at 60 °C for 60 min. After being cooled on ice for 5 min, the sample was acidified with 100 µl perchloric acid 35% (v/v) and centrifuged for 10 min at 10 000 g at 4 °C. Finally, 300 µl supernatant was transferred to a new tube and derivatized with 12.5 µl of 5 mM DNPH for 30 min at room temperature. This derivatized sample was protected from light. The HPLC analytical test was performed on a Shimadzu chromatographic system (Japan).
Mobile phase was prepared by mixing 380 ml acetonitrile with 620 ml MiliQ water and acidified with 0.2% acetic acid. The calibration curve prepared by acidic hydrolysis of 1 mM 1,1,3,3-tetraethoxypropane (Sigma-Aldrich) was referred as standard. All organic solvent used were of HPLC grade.
DNA damage was determined using the alkaline comet assay as previously described by Chin et al. [Citation15]. The assay was performed under dim light to prevent further DNA damage. Briefly, the slide was precoated with normal melting point agarose, covered and chilled on ice-cold flat tray. Then, 5 µl whole blood was mixed with 70 µl 0.6% low melting point agarose. Coverslip was removed carefully, and the suspension was pipetted onto the first agarose layer. Then, a new coverslip was applied on the slide and allowed to solidify. Coverslip was then removed and the slide was immersed in a cold lysing solution (2.5 M NaCl, 100 mM ethylene-diaminetetra-acetic acid, 10 mM Tris at pH 10, 1% Triton X-100, 1% sodium N-lauroyl sarcocinate, 10% dimethyl sulfoxide) at 4 °C for 1 h. Electrophoresis was performed in the freshly prepared and cooled (1–10 °C) electrophoresis buffer (0.3 M NaOH and 1 mM ethylene-diaminetetra-acetic acid) to a depth of approximately 0.25 cm for unwinding of the DNA. It was conducted for 20 min using 25 V and 300 mA. The slide was washed three times for 5 min each with a neutralizing solution (0.4 M Tris, pH 7.5). Staining was done with 20 µl/mL of ethidium bromide, and each slide was covered with a new coverslip. The slide was then stored in a humidified air-tight container in a refrigerator to prevent the drying of the gel.
Analysis of DNA damage was also performed using the protocol carried out by Chin et al. [Citation15], at a 200 × magnification using a fluorescence microscope. A total of 500 randomly non-overlapping cells on each slide were analyzed microscopically by categorizing cells as undamaged cells without tail (Type 0), cells with tiny tail (Type 1), cells with dim tail (Type 2), cells with a clear tail (Type 3) and only tail (Type 4) were analyzed. Type 0 and 1 cells represented the undamaged cell, whilst Type 2, 3 and 4 were characterized as cells with damaged DNA. A total damage score for each slide were calculated using the arbitrary formula by Heaton et al. (2002) [Citation16]:
Statistical analysis
SPSS version 17.0 (SPSS Inc., Chicago, IL) was used for statistical analysis. Data were presented as mean ± SD. Independent sample T test was used to determine differences between two variables. A repeated measure analysis of variance was used to calculate changes at baseline, 6 weeks and 12 weeks for all variables.
Results
Subjects characteristics
A total of 158 participants were involved in the screening phase (). However, 37 participants did not meet the BMI criteria, whilst 65 of them were not interested to participate in the study. A total of 56 participated and were consented. Subjects were randomized into two groups: FCR and CO. Each group consisted of 28 subjects. As shown in , the baseline characteristics of health status, body composition, blood pressure, glucose, total cholesterol, triglyceride and high-density lipoprotein (HDL) cholesterol were similar in both groups (p > 0.05). Only smoking status was significantly (p < 0.05) different between the two groups.
Figure 1. Recruitment process of the study.
Table 1. Baseline characteristics of the subject.
Food intake
There was a significant interaction effect (p < 0.01) and significant group effect (p < 0.001) in energy intake as the result of intervention. Energy intake in FCR group decreased from 1707 ± 267 kcal at baseline to 1402 ± 164 kcal at three months; whilst among CO group, energy intake increased from 1755 ± 335 kcal at baseline to 1816 ± 394 kcal at three months. Overall, there was 17.9% reduction in energy intake of the FCR group throughout the intervention period. A statistically significant intervention (p < 0.001) and group (p < 0.001) effects were also found in fat intake. Fat intake decreased in the FCR group (fat intake at baseline was 68.8 ± 25.4 g, fat intake at three months was 48.3 ± 12.9 g) but increased in the CO group (fat intake at baseline was 62.7 ± 17.1 g, fat intake at three months was 71.1 ± 12.6 g) ().
Table 2. Changes in energy and macronutrient intake.
Body composition
A significant interaction effect was found for body weight (p < 0.001), BMI (p < 0.01), fat percentage (p < 0.001) and fat mass (p < 0.05) (). All these variables decreased in the FCR group but maintained or increased in the CO group over the three months of intervention (). The maximum body weight reduction in the FCR group was 6.7 kg, with an average of 2.8 kg after three months of intervention.
Table 3. Changes in body composition.
Blood pressure and glucose
Both systolic (p < 0.05) and diastolic blood pressure (p < 0.05) improved significantly in the FCR group. No significant change was observed in fasting blood glucose level ().
Table 4. Changes in blood pressure and fasting blood glucose.
Lipid profile
There was a significant interaction effect in total cholesterol (p < 0.001), low-density lipoprotein (LDL) cholesterol (p < 0.05) and total cholesterol (TC)/HDL (p < 0.05) ratio values after the intervention. All of the variables improved in FCR group as compared to CO group. No significant effect was obtained in triglyceride and HDL cholesterol, despite triglyceride was decreased in FCR group after the intervention ().
Table 5. Changes in lipid profile.
DNA damage and lipid peroxidation level
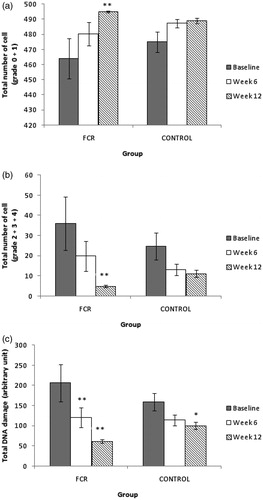
shows the result of total rejoining of DNA cells, which significantly increased (p < 0.001) in the FCR group following 12 weeks of intervention, while no significant change was observed in the CO group. There was also a significant decrease () (p < 0.001) in the total damage of DNA cells in the FCR group after 12 weeks of intervention. Overall (), total DNA damage scored using arbitrary unit was significantly decreased in both groups after 12 weeks; however, the change was prominent in the FCR group. A decrease in DNA damage scores was observed as soon as six weeks (p < 0.01) in the FCR group, and it remained low at 12 week (p < 0.001). In the CO group, a significant change was only observed in 12 week (p < 0.05).
Figure 2. (a) Total number of DNA rejoining cells as sum of grade 0 + 1 cells. The number of rejoining cells was increased significantly in FCR group (p < 0.001). No significant change was observed in the control group. (b) Total number of DNA damaged cells as sum of grade 2 + 3 + 4 cells. The number of damaged cells was decreased significantly in FCR group (p < 0.001). No significant change was observed in control group. (c) Total DNA damage, calculated using arbitrary unit. DNA damage was reduced significantly at week 6 (p < 0.01) and remained significant at week 12 (p < 0.001). Total DNA damage was also found decreased significantly in the control group (p < 0.05). Data expressed as mean ± SEM. Statistical test used was Wilcoxon Signed Rank Test. Significant level at *p < 0.05, **p < 0.01.
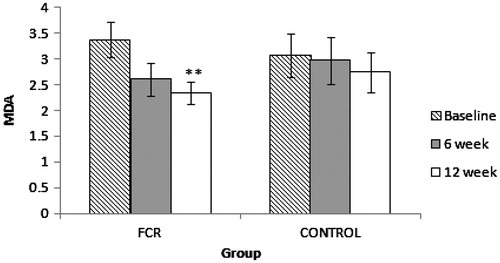
shows that the level of MDA, as an indicator of lipid peroxidation, was reduced significantly (p < 0.01) in the FCR group after 12 weeks. No significant change was observed in the CO group.
Figure 3. Malondialdehyde (MDA) as measured with HPLC. MDA was reduced significantly (p < 0.01) after three months of the study in FCR group. Data expressed as mean ± SEM. Statistical test used was Wilcoxon Signed Rank Test. Significant level at **p < 0.01.
Discussion
Nutrition plays a big impact in human aging, which may alter the regulation of aging process in the body through various mechanism [Citation17]. Our study indicates that FCR subjects were able to reduce their energy intake by approximately 18% after three months of the study. Although the reduction is lower than other CR studies [Citation11,Citation18,Citation19], the reduction is parallel with our aim to reduce 300–500 kcal/d from baseline energy intake. Reduction in fat intake was the biggest contribution in the change of total energy intake as the fat intake in the FCR group was reduced by 22.4%. If we compared with Ramadan fasting studies, there were conflicting results regarding the intake of fat [Citation20–23]. This intervention may benefit the Malaysian population, where the prevalence of obesity becomes epidemic following high fat consumption [Citation24–26].
The improvement in body composition is expected following FCR intervention. However, it may not be the best indicator of energy intake [Citation19,Citation27]. Therefore, biochemical parameters are also necessary to strengthen the result which might provide a better understanding on the underlying mechanism of FCR. In this study, FCR subjects reduced their body weight by approximately 3.4% and reduced fat mass by approximately 7.7%. This is in line with the recommendation of losing half to 1 lb/week following 300–500 kcal/d of energy intake reduction [Citation28]
As reported in the previous studies [Citation29,Citation30], we also found an improvement in FCR subjects’ blood pressure. Weight loss is always recommended for those overweight and obese hypertensive subjects, and it can be achieved by practicing CR [Citation31]. In addition, FCR also improved lipid profile of our intervention subjects. Decreased in total cholesterol and LDL-cholesterol may help to reduce the risk of cardiovascular mortality [Citation32]. The ratio of TC/HDL cholesterol was also improved in this study. This ratio was proved to be the strongest predictor of cardiovascular disease risk as compared to individual lipoprotein value [Citation33]. However, we did not find any improvement in HDL cholesterol in both groups. This may suggest a lack of physical activity among subjects as previously reported, which may contribute to the sedentary behaviors of the subject during fasting [Citation34,Citation35].
Genetic factors, lifestyle and age may as well affect the oxidative stress markers. It has been suggested earlier [Citation36,Citation37] that CR can reduce oxidative stress in many species due to reduction in the production of reactive oxygen species [Citation36–38]. However, study on fasting and oxidative stress is still lacking. An earlier study by Ibrahim et al. [Citation39] concluded that Ramadan fasting may not alter oxidative stress markers, which is conflicting with another study [Citation40] that showed an improvement in urinary MDA following short-term fasting program.
We tested the effect of FCR on DNA damage using alkaline comet assay and MDA, a common biomarker of lipid peroxidation as an indicator of oxidative stress. Our results indicate that FCR may improve both of these values following intervention, suggesting a protecting effect by limiting calorie intake. Reduction of DNA damage was observed as soon as 6 weeks of FCR intervention and remained low at 12 weeks. In fact, the rejoining of those breaks was observed following the intervention period. This is interesting as FCR may have beneficial effects to repair DNA damage in elderly population. We also found some improvement in total DNA damage in our CO group. However, the changes were not as highly significant as observed in the FCR group. With respect to MDA, the reduction was significant at 12 weeks. As there was evidence that DNA damage [Citation41–43] and MDA [Citation42,Citation44,Citation45] will increase with age, we believe that FCR is among those interventions that can help improve oxidative stress among the elderly.
Conclusion
To our best knowledge, this is the first study introducing a model of healthy eating, which comprise of religious practice in scientific experiment. Our data revealed that a combination of CR and Muslim Sunnah fasting improved body composition, energy and macronutrient intake, blood pressure, lipid profile and oxidative stress markers among healthy older adult. These observations need further research in molecular mechanism involved in the effects of FCR.
Declaration of interest
The authors declare no conflict of interest. This study was sponsored by UKM Arus Perdana research grant, UKM-AP-TKP-09/2009.
Acknowledgements
We would like to thank the fieldworkers and health staff who participated during the data collection.
References
- Kinsella K, He W. An aging world: 2008. USA: US Census Bureau, International Population Reports; 2009
- WHO. The World Health Report 2008. Geneva: WHO; 2008
- Mathers CD, Sadana R, Salomon JA, et al. Healthy life expectancy in 191 countries, 1999. Lancet 2001;357:1685–91
- WHO. 2009. Data from the Global Health Observatory. Available from: <http://www.who.int/countries/mys/en/> [last accessed 18 Oct 2012]
- IPH. The Third National Health and Morbidities Survey. Kuala Lumpur: IPH; 2008
- Mariappan P, Chong WL. Prevalence and correlations of lower urinary tract symptoms, erectile dysfunction and incontinence in men from a multiethnic Asian population: results of a regional population-based survey and comparison with industrialized nation. BJU International 2006;98:1264–8
- Courtenay WH. Constructions of masculinity and their influence on men’s well-being: a theory of gender and health. Soc Sci Med 2000;50:1385–401
- Kraemer S. The fragile male. BMJ 2000;321:1609–12
- Macdonald JJ. Shifting paradigms: a social-determinants approach to solving problems in men's health policy and practice. Med J Aust 2006;185:456–8
- Robertson LM, Douglas F, Ludbrook A, et al. What works with men? A systematic review of health promoting interventions targeting men. BMC Health Serv Res 2008;8:141
- Heilbronn LK, de Jonge L, Frisard MI, et al. Effect of 6-month calorie restriction on biomarkers of longevity, metabolic adaptation, and oxidative stress in overweight individuals: a randomized controlled trial. JAMA 2006;295:1539–48
- Trepanowski JF, Bloomer RJ. The impact of religious fasting on human health. Nutr J 2010;9:57
- Teng NI, Shahar S, Manaf ZA, et al. Efficacy of fasting calorie restriction on quality of life among aging men. Physiol Behav 2011;104:1059–64
- Pilz J, Meineke I, Gleiter CH. Measurement of free and bound malondialdehyde in plasma by high-performance liquid chromatography as the 2,4-dinitrophenylhydrazine derivative. J Chromatogr B Biomed Sci Appl 2000;742:315–25
- Chin SF, Hamid NA, Latiff AA, et al. Reduction of DNA damage in older healthy adults by Tri E Tocotrienol supplementation. Nutrition 2008;24:1–10
- Heaton PR, Ransley R, Charlton CJ, et al. Application of single-cell gel electrophoresis (comet) assay for assessing levels of DNA damage in canine and feline leukocytes. The American Society for Nutritional Science. J Nutr 2002;132:1598S–603S
- Roberts SB, Rosenberg I. Nutrition and aging: changes in the regulation of energy metabolism with aging. Physiol Rev 2006;86:651–67
- Witte AV, Fobker M, Gellner R, et al. Caloric restriction improves memory in elderly humans. Proc Natl Acad Sci U S A 2009;106:1255–60
- Racette SB, Weiss EP, Villareal DT, et al. One year of caloric restriction in humans: feasibility and effects on body composition and abdominal adipose tissue. J Gerontol A Biol Sci Med Sci 2006;61:943–50
- Bouhlel E, Zaouali M, Miled A, et al. Ramadan fasting and the GH/IGF-1 axis of trained men during submaximal exercise. Ann Nutr Metab 2008;52:261–6
- el Ati J, Beji C, Danguir J. Increased fat oxidation during Ramadan fasting in healthy women: an adaptative mechanism for body-weight maintenance. Am J Clin Nutr 1995;62:302–7
- Adlouni A, Ghalim N, Benslimane A, et al. Fasting during Ramadan induces a marked increase in high-density lipoprotein cholesterol and decrease in low-density lipoprotein cholesterol. Ann Nutr Metab 1997;41:242–9
- Lamine F, Bouguerra R, Jabrane J, et al. Food intake and high density lipoprotein cholesterol levels changes during ramadan fasting in healthy young subjects. Tunis Med 2006;84:647–50
- Ismail MN, Chee SS, Nawawi H, et al. Obesity in Malaysia. Obes Rev 2002;3:203–8
- Khambalia AZ, Seen LS. Trends in overweight and obese adults in Malaysia (1996-2009): a systematic review. Obes Rev 2010;11:403–12
- Mohamud WN, Musa KI, Khir AS, et al. Prevalence of overweight and obesity among adult Malaysians: an update. Asia Pac J Clin Nutr 2011;20:35–41
- Schoeller DA. The energy balance equation: looking back and looking forward are two very different views. Nutr Rev 2009;67:249–54
- NHLBI. Expert Panel on the Identification, Evaluation, and Treatment of Overweight in Adults. Clinical guidelines on the identification, evaluation, and treatment of overweight and obesity in adults: executive summary. Am J Clin Nutr 1998;68:899–917
- Mattson MP, Wan R. Beneficial effects of intermittent fasting and caloric restriction on the cardiovascular and cerebrovascular systems. J Nutr Biochem 2005;16:129–37
- Fontana L, Meyer TE, Klein S, Holloszy JO. Long-term calorie restriction is highly effective in reducing the risk for atherosclerosis in humans. Proc Natl Acad Sci U S A 2004;101:6659–63
- Mertens IL, Van Gaal LF. Overweight, obesity, and blood pressure: the effects of modest weight reduction. Obes Res 2000;8:270–8
- Haffner S. Rationale for new American Diabetes Association Guidelines: are national cholesterol education program goals adequate for the patient with diabetes mellitus? Am J Cardiol 2005;96:33E–6E
- Ridker PM, Stampfer MJ, Rifai N. Novel risk factors for systemic atherosclerosis: a comparison of C-reactive protein, fibrinogen, homocysteine, lipoprotein(a), and standard cholesterol screening as predictors of peripheral arterial disease. JAMA 2001;285:2481–5
- Ziaee V, Razaei M, Ahmadinejad Z, et al. The changes of metabolic profile and weight during Ramadan fasting. Singapore Med J 2006;47:409–14
- Roky R, Houti I, Moussamih S, et al. Physiological and chronobiological changes during Ramadan intermittent fasting. Ann Nutr Metab 2004;48:296–303
- Sohal RS, Allen RG. Relationship between metabolic rate, free radicals, differentiation and aging: a unified theory. Basic Life Sci 1985;35:75–104
- Heilbronn LK, Ravussin E. Calorie restriction and aging: review of the literature and implications for studies in humans. Am J Clin Nutr 2003;78:361–9
- Sohal RS, Weindruch R. Oxidative stress, caloric restriction, and aging. Science 1996;273:59–63
- Ibrahim WH, Habib HM, Jarrar AH, Al Baz SA. Effect of Ramadan fasting on markers of oxidative stress and serum biochemical markers of cellular damage in healthy subjects. Ann Nutr Metab 2008;53:175–81
- Lee KH, Bartsch H, Nair J, et al. Effect of short-term fasting on urinary excretion of primary lipid peroxidation products and on markers of oxidative DNA damage in healthy women. Carcinogenesis 2006;27:1398–403
- Mendoza-Nunez VM, Sanchez-Rodriguez MA, Retana-Ugalde R, et al. Total antioxidant levels, gender, and age as risk factors for DNA damage in lymphocytes of the elderly. Mech Ageing Dev 2001;122:835–47
- Mutlu-Turkoglu U, Ilhan E, Oztezcan S, et al. Age-related increases in plasma malondialdehyde and protein carbonyl levels and lymphocyte DNA damage in elderly subjects. Clin Biochem 2003;36:397–400
- Singh NP, Danner DB, Tice RR, et al. Basal DNA damage in individual human lymphocytes with age. Mutat Res 1991;256:1–6
- Balkan J, Kanbagli O, Mehmetcik G, et al. Increased lipid peroxidation in serum and low-density lipoproteins associated with aging in humans. Int J Vitam Nutr Res 2002;72:315–20
- Kasapoglu M, Ozben T. Alterations of antioxidant enzymes and oxidative stress markers in aging. Exp Gerontol 2001;36:209–20