Abstract
Objectives. Aquaporin-7 is a water-channel protein that controls tissue glycerol supply after ischemia. A burden of experimental studies suggests that Diazoxide, a mitochondrial KATP-channel opener, may decrease myocardial edema during coronary artery bypass grafting (CABG). We evaluated whether Diazoxide has an impact on atrial Aquaporin-7 expression during CABG. Design. Sixteen patients with a history of stable coronary artery disease were enrolled in the study. Eight patients were treated during cardiopulmonary bypass with Diazoxide, while the rest eight patients remained as Controls. Histopathology was evaluated from biopsies procured before and during CABG from the right atrium. From fresh atrial tissue biopsies, Aquaporin-7 was quantified by RT-PCR. Results. Histological differences were apparent between individual patients already before operation at base line reflecting differences in severity of myocardial ischemia. As compared with Fold Change values before operation, Aquaporin-7 expression after operation was positive in all but one Control, whereas Aquaporin-7 expression was positive in only two patients receiving Diazoxide. The relative Aquaporin-7 expression was significantly lower in patients treated with Diazoxide as compared with Controls (p < 0.05). Conclusions. Diazoxide may have an impact on myocardial water balance and glycerol energy supply by decreasing relative Aquaporin-7 expression during CABG.
Coronary artery bypass grafting (CABG) has evolved to a life-saving procedure due to its efficacy in salvaging ischemic myocardium. However, in addition to aortic clamping, CABG utilizes cardiopulmonary bypass (CPB), which renders the myocardium susceptible to water inbalance and subsequent edema as a consequence of decreased cardiac energy supply (Citation1). Edema in turn, may predispose to cardiac failure and arrhythmias such as atrial fibrillation. Edema also reflects the severity of ischemia due to the degree of the coronary artery disease itself. Clearly, myocardial edema is associated with the outcome of patients after CABG (Citation1).
Attempts to limit edema during CABG have led to a few experimental studies. Three different stress pathways have thence been described that induce edema: hyperkalemic cardioplegia, mild hyposmotic stress, and ischemic stress, all being targets for the mitochondrial adenosine triphosphate-sensitive potassium (KATP) channel opener Diazoxide (Citation2–4). Diazoxide mimics ischemic preconditioning in animal models (Citation5) and limits myocardial edema (Citation2). Clinical data is still scarce, but suggest for a protective role of Diazoxide (Citation6). Some studies claim that Diazoxide may also have an effect through activation of sarcolemma (Citation7), though others are against this (Citation8). Taken together, the mechanisms involved in decreasing edema after ischemia reperfusion after administration of Diazoxide remain controversial (Citation3,Citation6,Citation8).
Myocardial Aquaporins are involved in water trafficking during normal and pathological conditions. Aquaporin proteins form transmembrane channels that participate in water movement along osmotic gradients. Increased expression of Aquaporin-4 is associated with the formation of myocardial edema (Citation9). Its differential expression pattern is dependent on tissue destruction in cancer (Citation10). Aquaporin-7, on the other hand, is a cell-membrane receptor facilitating both glycerol and water trafficking from the cell to the interstitium thus controlling both edema and cardiac energy supply (Citation11). According to our previous experience, excessive Aquaporin-7 expression may be considered as an early marker of histological tissue damage after ischemia-reperfusion and edema (Citation12).
We hypothesized that the right atrium during CABG would be susceptible to edema and ischemic changes depending on cardiac energy distribution by glycerol as a substrate. The aim of this study was to evaluate, in a clinical set up, whether Diazoxide has an impact on Aquaporin-7 expression of the right atrium during CABG.
Material and methods
After institutional approval by Tampere University Hospital Ethics Committee, the protocol for this prospective randomized, double blind, placebo-controlled study was reviewed by National Agency for Medicines, Finland. All 16 patients gave their informed consent. The patients were scheduled for elective CABG using on pump cardiopulmonary bypass technique (CPB).
Patient selection was planned to result in homogenous study and Control groups. The inclusion criteria included stable myocardial coronary artery disease eligible for elective CABG, but with a history of a recent less than one month old myocardial infarction and detection of elevated Troponin T (TNT > 0.01 μg/l) or Creatinin kinase (CK-MB > 1U/l) release. The exclusion criteria were redo cardiac operation, preoperative diagnosis of asthma, chronic obstructive pulmonary disease (COPD), kidney function impairment, liver dysfunction, high TNT (>1 μg/l) and unstable myocardial coronary artery disease in need of emergency operation. Patients with poor left ventricular function (ejection fraction EF ≤ 30%), valvular disease, and those receiving corticosteroids were also not eligible.
Anesthesia, operative and perfusion techniques were carried on as previously described (Citation13). Briefly, anesthesia was induced with propofol (0.5–1.0 mg/kg), sufentanil (0.6–0.8 μg/kg) and cis-atracurium, and Sufentanil infusion was continued with a rate of 0.03–0.05 μg/kg/min. Sevoflurane was used as the main anesthetic agent throughout the operation, which included standardized surgical techniques in every case. Through a median sternotomy, CPB was established, and one internal thoracic artery together with one to four peripheral vein grafts were harvested to perform coronary artery bypasses.
Cardioplegia and Diazoxide administration
Patients were allocated into two groups. Eight patients received Diazoxide 50 μg/l injected into the aortic root at the onset of cross-clamping. Eight other patients served as Controls and received normal saline as placebo. All patients received routine blood cardioplegia delivered through antegrade route.
Tissue harvesting included two samples of right atrium that were procured from each patient. The first sample was obtained before aortic cross clamping. The second sample was taken from the same location before CPB was stopped. Half of the harvested myocardial tissue (5–10 × 3 mm) was immersed in phosphate buffered saline and immediately frozen in liquid nitrogen for RNA analysis. The other half of the sample was immersed in formalin and embedded in paraffin for histological studies.
Sample collection and hemodynamic measurements
Hemodynamic parameters were obtained through radial and pulmonary artery catheter lines. Hemodynamic monitoring comprised measurement of heart rate (HR), mean arterial pressure (MAP), and cardiac output (CO). Derived cardiovascular variables such as cardiac index (CI) were calculated from standard formulas. All CO measurements were based on the thermodilution technique, and data collection was started as base line measurements before induction of anesthesia. Preoperative baseline CK-MB, TNT and hemodynamic measurements were obtained, followed by postoperative hemodynamic measurements up to the first postoperative morning.
Histology
For histology, the 5-μm sections were stained with hematoxylin and eosin. Evaluation was performed blinded to the study protocol (AM) and technically unclear slides were rejected. The following signs of injury were evaluated separately: presence of myocardial edema and ischemia, presence of hemorrhage, and intramyocardial artery edema and periadventitial inflammation. Myocardial edema and ischemia was scored as follows and expressed as point score units (PSU): 0 (no changes), 1 (presence of occasional foci of myocardial edema with dark myocardial nuclei), 2 (large areas of edema including also non-edematous myocardium with round-shaped normal nuclei), 3 (myocardial edema including vacuolized and shrink dark myocardial nuclei). As hemorrhage was only seldom present in occasional foci, it was scored as either 0 (not present) or 1 (present). As vacuolization of nuclei of the media layer of intramyocardial arteries reflected edema (Citation12), a representative cross-sectional intramyocardial artery was chosen randomly. The majority of the arterial wall nuclei was round-shaped representing normal nuclei, and sharp-edged blue nuclei of the media cells were defined as non-preserved and estimated together with vacuolated and edematous nuclei: 0 (presence of neither sharp-edged blue nor vacuolated nuclei), 1 (>50% of the arterial wall nuclei being round-shaped normal nuclei), 2 (presence of both round- and sharp-shaped nuclei with occasional foci of vacuolization), 3 (>50% of the arterial wall nuclei being non-preserved and vacuolated). Periadventitial inflammation was graded either 0 (not present) or 1 (presence of occasional inflammatory cells). A histological damage score was obtained by adding the evaluated signs of injury to allow semi-quantitative comparison between patients. A relative histological damage score change was obtained by subtracting the histological damage score during operation from that before operation.
Quantitative RT-PCR analysis
The frozen tissue was homogenized and RNA was extracted using a rotor-stator homogenizer and NucleoSpin® RNA II kit (Machery-Nagel GmbH & Co, Düren, Germany) according to the manufacturer's instructions. 50 ng of total RNA was reverse-transcribed into cDNA in reaction volume of 20 μl. The quantitative reverse transcriptase polymerase chain reaction (qRT-PCR) was performed with standard protocols on Abi Prism 7300 instrument (Applied Biosystems, CA, USA). The PCR reaction was performed with TaqMan® Gene Expression assays for aquaporin-7 (ID Rn00569727_m1) and GAPDH (ID Rn01462662_g1) (both from Applied Biosystems) according to the manufacturer's instructions with TaqMan® Universal PCR Master Mix. All samples were performed as three replicates.
The expression levels of Aquaporin-7 and GAPDH as an internal control/house keeping gene were evaluated. Ct values were determined for every reaction and the relative quantification was calculated using the 2−ΔΔCt method (Citation14). Briefly, the data was normalized to the expression of house keeping gene GAPDH, and values of control samples were used as a calibrator. The expression of Aquaporin-7 before operation in each patient was settled to obtain the value 1, while Aquaporin-7 during CABG was expressed as Fold Changes. Aquaporin-7 change was therefore either positive (+1) or negative (-1) during operation as compared with a base line of 1 before operation.
Statistics
Data is presented as mean ± standard error of the mean (sem). Nonparametric data were analyzed with Mann-Whitney U-test among study groups. Statistical significance was attributed to p-values lower than 0.05. Statistical analyses were performed with commercial statistical software (SPSS 17.0, SPSS Inc, Chicago, IL). Power calculation was set to display the 95% confidence interval and performed with statistical software (PowerAndPrecision 4.0, Biostat, Englewood, NJ).
Results
Demographics, hemodynamics and outcome
As shown in , the majority of the patients receiving Diazoxide were males (7/8). All patients with Diazoxide had 3-vessel coronary artery disease, whereas three of eight 8 Control patients had 2-vessel coronary artery disease. The majority of the patients had preoperative sinus rhythm. There were no differences in the preoperative treatment protocol of the patients. As shown in , no differences were observed among patients in hemodynamic parameters evaluated before operation at base line and at the end of operation. Postoperatively, sinus rhythm was equally distributed among patients. Momentary atrial fibrillation was treated with Amiodarone infusion in six patients, three with Diazoxide and three without Diazoxide. However, one patient experienced postoperative subacute stroke, and one patient had sudden unexpected asystole leading to emergency resternotomy and death. Both of these latter two patients had received Diazoxide.
Table I. Demographics of Controls and patients with Diazoxide.
Table II. Perioperative hemodynamics.
Histology
Before and during operation, edema situated not only in the myocardium, but was often detected as vacuolization of intramyocardial arteries. In three Controls, periadventitial inflammation was also present after operation. No differences in these parameters of tissue edema between groups were observed (). Nevertheless, as shown in , histological differences were apparent already before operation at base line reflecting severity of myocardial ischemia.
Figure 1. Representative histology of right atrium before (A) and during (B) coronary artery bypass grafting (CABG). Note increased vacuolized and dark sharp-edged intramyocardial nuclei indicating tissue edema and ischemia shown with arrows in B.
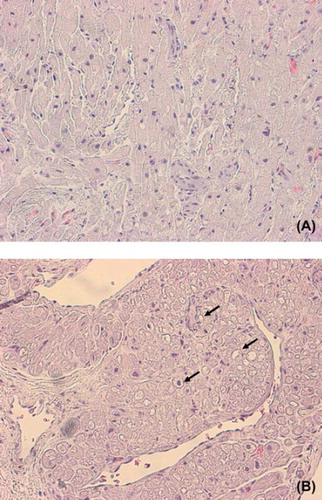
Table III. Postoperative hemodynamics.
Table IV. Histology of right atrium.
Aquaporin-7 expression
Technically, qRT-PCR for Aquaporin-7 expression was successful in 12 patients (six patients in each group) before and during operation. As shown in , Aquaporin-7 expression of the right atrium in each patient during operation was either positive or negative in relation to Fold Changes of expression before operation. Aquaporin-7 expression during operation was positive in all but one Control, whereas Aquaporin-7 expression was positive in only two patients receiving Diazoxide.
Figure 2. Aquaporin-7 during coronary artery bypass grafting (CABG) in Controls and in patients with Diazoxide. Dark thick line indicates base line (+ 1) Aquaporin-7 expression before CABG to which Fold Change values during CABG were compared within each patient.
Relative Aquaporin-7 expression changes
Aquaporin-7 expression changes were adjusted according to histological damage in each patient, since both Aquaporin-7 and histological damage score changes differed among patients at base line and at the end of operation. The relative Aquaporin-7 expression was calculated by dividing Aquaporin-7 change by the relative histological damage score in each patient. As shown in , the median of relative Aquaporin-7 expression was significantly lower in patients treated with Diazoxide (p < 0.05). For the effect size (group means of 20.5 vs. 0.7), SD (0.6), patient number (5 and 6), alpha (0.050, 2-tailed), power is 0.84.
Figure 3. Aquaporin-7 change/ histological damage score change during coronary artery bypass grafting (CABG) in Controls (black boxes) and in patients with Diazoxide (open triangles). Median is shown in each group with a horizontal line. In comparison with histological damage score change, Aquaporin-7 change after CABG was significantly decreased in patients with Diazoxide treatment (p < 0.05, Power 0.84).
Discussion
In this study, we show that Diazoxide administrated during CABG attenuates Aquaporin-7 expression of the right atrium as compared with its histological damage score. Excessive Aquaporin-7 expression is dependent on histopathology and may indicate tissue damage (Citation12).
Though Diazoxide is a mitochondrial KATP-channel opener, it may have a dual effect on sarcolemma as well. In an experimental model of acute myocardial infarction, Diazoxide decreases apoptosis and regional myocardial cell necrosis by attenuating mitochondrial damage (Citation15). Studies on ischemic preconditioning suggest for apoptotic related mechanisms associated with opening of KATP-channels (Citation16). In another experimental setting, Diazoxide inhibited caspase-dependent and -independent apoptotic pathways while preserving mitochondrial structure thus enhancing neurological recovery after spinal cord ischemia and reperfusion injury (Citation17). We did not study apoptosis from biopsies taken from the right atrium, since previously it has been shown that apoptosis may in overall be non-significant very early after reperfusion in the human heart (Citation13).
Besides KATP-channel opening, other molecular mechanisms seem to be involved with Diazoxide. The down-regulation of Aquaporin-4 expression in an experimental setting was associated with decrease of neuronal edema after treatment with a KATP-channel opener (Citation7). This in turn, promoted behavioral recovery and enhanced protection against neuronal apoptosis and necrosis. Edema and water balance are regulated by Aquaporins and associated with cellular electrolyte trafficking. Diazoxide, while opening KATP-channels, may directly or indirectly ameliorate cellular electrolyte balance after ischemia-reperfusion. Aquaporin-7, as a member of the aquaglyceroporin family, permeates intracellular water and glycerol. Glycerol acts as an energy substrate in the heart (Citation11), and down-regulation of Aquaporin-7 may indicate relatively low energy need of the heart during CPB and Diazoxide treatment. Thence, Aquaporin-7 expression may be considered here as a surrogate of tissue edema and damage (Citation12).
Nevertheless, we did neither observe decrease in incidence of atrial fibrillation nor functional amelioration despite Diazoxide, may be owing to other simultaneous treatment such as Beta blockers. Sevoflurane may have had an effect on the KATP-channels comparable to that of adenosine. However, both groups of patients received the same anesthetic and treatment protocol, lest not counting Diazoxide. While biopsies from the right atrium were most vulnerable to histopathological edema changes after operation, it is worth to note that the patients may have been at base line susceptible to heterogeneous ischemic insult. Though the demographics of the patients were non-significant among groups and the patient were carefully selected to obtain only stable coronary artery disease, it may be argued that this still represents an inadequate selection to delete bias from different histopathological pictures associated with clinical ischemia due to coronary artery disease. The relative small number of patients is a limitation of the study. Again, two unexpected complications (subacute stroke and unexpected hemodynamic collapse) occurred both in the Diazoxide group. The possible connection of these events with Diazoxide needs to be verified in a subsequent study.
Despite these limitations, we link Diazoxide with decrease of relative Aquaporin-7 expression as compared with histopathological damage score for the first time in a clinical setting. Though power calculation of even up to 84% for Aquaporin-7 change associated with histology change indicates that Diazoxide may have an important impact during surgery, it is pertinent to warrant further clinical evidence for its efficacy. It thus remains to be shown whether this indicates that Diazoxide treatment may be associated with preserving heart energy supplies and functional capacity by decreasing the incidence of arrhythmias after CABG.
Acknowledgements
This study was financially supported by the Competitive Research Funding of the Tampere University Hospital (Grant 9M056), the Finnish Cultural Foundation and the Tampere Tuberculosis Foundation.
Declaration of interest: The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
References
- Toraman F, Evrenkaya S, Yuce M, Turek O, Aksoy N, Karabulut H, . Highly positive intraoperative fluid balance during cardiac surgery is associated with adverse outcome. Perfusion. 2004;19:85–91.
- Al-Dadah AS, Voeller R, Shuessler RB, Damiano R, Lawton JS. Maintenance of myocyte volume homeostasis during stress by Diazoxide is cardioprotective. Ann Thorac Surg. 2007;84: 857–62.
- Mizutani S, Al-Dadah AS, Bloch JB, Prasad SM, Diodato MD, Shuessler RB, . Hyperkalemic cardioplegia-induced myocyte swelling and contractile dysfunction: Prevention by Diazoxide. Ann Thorac Surg. 2006;81:154–9.
- Prasad SM, Al-Dadah AS, Byrd GD, Fagg TP, Gomes J, Damiano R, . Role of the sarcolemmal adenosine triphosphate-sensitive potassium channel in hyperkalemic cardioplegia-induced myocyte swelling and reduced contractility. Ann Thorac Surg. 2006;81:148–53.
- Liu Y, Sato T, O'Rourke B, Marban E. Mitochondrial ATP-dependent potassium channels: Novel effectors of cardioprotection? Circulation. 1998;97:2463–9.
- Broadhead MW, Kharbanda RK, Peters MJ, MacAllister RJ. KATP channel activation induces ischemic preconditioning of the endothelium in humans in vivo. Circulation. 2004;110: 2077–82.
- Zhu HL, Luo WQ, Wang H. Iptakalim protects against hypoxic brain injury through multiple pathways associated with ATP-sensitive potassium channels. Neuroscience. 2008;157:884–94.
- Sellitto AD, Maffit SK, Al-Dadah AS, Zhang H, Schuessler RB, Nichols CG, . Diazoxide maintenance of myocyte volume and contractility during stress: Evidence for a non-sarcolemmal KATP channel location. J Thorac Cardiovasc Surg. 2010;140: 1153–9.
- Warth A, Eckle T, Kohler D, Faigle M, Zug S, Klingel K, . Upregulation of the water channel aquaporin-4 as a potential cause of postischemic cell swelling in a murine model of myocardial infarction. Cardiology. 2007;107:402–10.
- Xu H, Zhang Y, Wei W, Shen L, Wu W. Differential expression of aquaporin-4 in human gastric normal and cancer tissues. Gastroenterologie Clin Biol. 2009;33:72–6.
- Hibuse T, Maeda N, Nakatsuji H, Tochino Y, Fujita K, Kihara S, . The heart requires glycerol as an energy substrate through aquaporin 7, a glycerol facilitator. Cardiovasc Res. 2009;83:34–41.
- Liu Z, Vuohelainen V, Tarkka M, Tenhunen J, Lappalainen RS, Narkilahti S, . Glutamate release predicts ongoing myocardial ischemia of rat hearts. Scand J Clin Lab Invest. 2010; 70:217–24.
- Slalaby A, Rinne T, Jarvinen O, Saraste A, Laurikka J, Porkkala H, . Initial results of a clinical study: Adenosine enhanced cardioprotection and its effect on cardiomyocytes apoptosis during coronary artery bypass grafting. Eur J Cardiothorac Surg. 2008;33:639–44.
- Livak KJ, Schmittgen TD. Analysis of relative gene expression data using real-time quantitative PCR and the 22ΔΔCt method. Methods. 2001;25:402–8.
- McCully JD, Wakiyama H, Cowan DB, Federman M, Parker RA, Levitsky S. Diazoxide amelioration of myocardial injury and mitochondrial damage during cardiac surgery. Ann Thorac Surg. 2002;74:2138–46.
- Beresewicz A, Maczewski M, Duda M. Effect of classic preconditioning and Diazoxide on endothelial function and O2 and NO generation in the post-ischemic guinea-pig heart. Cardiovasc Res. 2004;63:118–29.
- Roseborough G, Gao D, Chen L, Trush MA, Zhou S, Williams GM, . The mitochondrial K-ATP channel opener, Diazoxide, prevents ischemia-reperfusion injury in the rabbit spinal cord. Am J Pathol. 2006;168:1443–51.