Abstract
Background: The deletion/insertion (D/I) polymorphism in the angiotensin-converting enzyme (ACE) gene has been implicated in susceptibility of chronic obstruction pulmonary disease (COPD), but a number of studies have reported inconclusive results. The aim of this study is to investigate the relationship between the D/I polymorphism in the ACE gene and COPD risk by meta-analysis. Method: We searched Pubmed database, Embase database, CNKI database and Wanfang database, covering all studies until October 10, 2011. Statistical analysis was performed by using the software Revman4.2 and STATA 10.0. Results: A total of 710 COPD cases and 862 controls in 10 case-control studies were included in this study. The results suggested that the DD homozygote carriers did not have an increased or decreased risk of COPD when compared with the heterozygote DI and II homozygote carriers. However, in the subgroup analysis by race, significant increased risks were found in Asian DD homozygote carriers (OR = 2.6 and 95% CI = 1.47–4.57 for DD vs. DI+II) but not in Caucasian DD homozygote carriers (OR = 0.91, 95%CI = 0.69–1.22, P = 0.54 for DD vs. DI+II). Conclusions: This meta-analysis suggested that the ACE gene is a COPD susceptible gene in Asian populations. Future studies are needed to validate our conclusions..
Keywords :
Introduction
Chronic obstructive pulmonary disease (COPD) remains the fourth-leading cause of death worldwide (Citation1,2). It is well known that the disease is characterized by infiltration of inflammatory cells, destruction of lung parenchyma, and airway wall remodeling (Citation3). It is widely accepted that COPD is a complex disease that affected by both environmental and genetic factors (Citation4), and efforts to elucidate the genetic background of COPD have been increased in the past few years (Citation5,6). Many candidate genes have been considered as COPD susceptible genes, such as mEPHX(Citation7), GSTP1(Citation8), GSTT1(Citation9), TNF-α(Citation10)and ACE(Citation11), et al. Among them, the ACE gene was one of the extensively studied.
Angiotensin-converting enzyme is a key enzyme of the rennin-angiotensin system and may play important roles in the pathogenesis of COPD, a significant higher serum ACE activity and plasma rennin activity was found in COPD patients than in normally subjects (Citation13). Angiotensin-converting enzyme converts angiotensin I(AI) to angiotensin II(AII), which may be involved in the etiology of COPD (Citation13). The ACE gene is located on chromosome 17q23 and consists of 26 exons and 25 introns (Citation12). An important polymorphism which is based on insertion (I) or deletion (D) of 287 base pairs has been identified in the intron 16. The D allele of the polymorphism has been associated with elevated plasma ACE levels and ACE activity. Several studies have reported the associations between the D/I polymorphism in the ACE gene and the risk of COPD (Citation13–22), however, the results have been inconclusive. This may be partly because of the possible small sample size in each of the published studies and different populations. A quantitative synthesis for accumulate data from different studies is needed to provide precise evidence on the association (Citation23). To derive a more precise result, we performed a meta-analysis of all eligible studies. To our knowledge, this is the most comprehensive genetic meta-analysis concerning the relationship between the ACE D/I polymorphism and the risk of COPD.
Methods
Search strategy
We searched the Pubmed database, Embase database, Chinese National Knowledge Infrastructure database (CNKI), and the Wanfang database to identify studies that assessed the association between the D/I polymorphism in the ACE gene and the risk of COPD. We collected all available studies before October 10, 2011. The search terms were used as follows: ‘chronic obstructive pulmonary disease or COPD’, and ‘angiotensin-converting enzyme or ACE’, and in combination with ‘polymorphism or mutation or variant’. There was no language restriction. The studies included the meta-analysis should meet the following inclusion criteria: (Citation1) the study should assess the association between the D/I polymorphism of ACE gene and the risk of COPD, (Citation2) the included studies should be designed as a case-control study, (Citation3) genotype distributions in both cases and controls were available for estimating an odds ratio (OR) with 95% confidence interval (CI), (Citation4) the genotype distributions of the controls should be consistent with Hardy-Weinberg Equilibrium(HWE). In addition, the following exclusion criteria were used: (Citation1) abstract and reviews, (Citation2) repeated or overlapped studies.
Data extraction
Two independent authors carefully assessed all studies, and extracted the following information from each study: the first author's name, country of origin, year of publication, race, number of cases and controls, genotyping methods, definition of COPD, genotype distribution in cases and controls.
Statistical analysis
The strength of association between ACE D/I polymorphism and COPD risk was assessed by odds ratios (OR) with the corresponding 95% confidence intervals (CI). The genetic models evaluated for pooled OR of the polymorphism was recessive model (DD vs. DI+II), which was based on most of the primary studies. OR was calculated by a fixed-effects model (the Mantel-Haenszel method) or a random-effects model (the DerSimonian and Laird method) according to the heterogeneity. Heterogeneity among studies was checked by a X2 based Q statistic and I2 and was considered statistical significant at P < 0.10. When the P value is greater than 0.10, the pooled OR of each study was calculated by the fixed-effects model, otherwise, a random-effects model was used. The significance of the pooled OR was determined by the Z-test and P less than 0.05 was considered as statistically significant. To evaluate the race-specific effects, subgroup analyze was performed by race groups. For the polymorphism, other genetic models (DD+DI vs. II, DD vs. II, DI vs. II, D vs. I) were also used to assess the association with the risk of COPD.
Publication bias was analyzed by several methods. Visual inspection of asymmetry in funnel plots was carried out. The Begg's test and Egger's test were also used to statistically assess publication bias (using a p-value of <0.05) (Citation24). Hardy-Weinberg equilibrium was tested by using Pearson's X2 test. All statistical tests were performed by using the Revman4.2 software and STATA 10.0.
Results
Studies selected
As shown in , after an initial search from the selected electronic databases, a total of 85 literatures were identified. After reading the titles and abstracts, 64 literatures were excluded for not being relevant to COPD risk and ACE gene. The remaining 21 literatures were identified for full-text view and data extraction (details can be obtained on request from the corresponding author). Seven literatures were excluded for not reporting the usable data or not a case-control study. Thus, a total of 14 case-control studies in 14 literatures were identified. In addition, 3 case-control studies were excluded for data overlapped or duplicated, 1 case-control study was excluded for the genotype in the control population not consistent with HWE. Finally, a total of 10 case-control studies in 10 literatures which met the inclusion criteria were identified (Citation13-22). The characteristics of each case-control study are listed in . Genotype and allele distributions for each case-control study are shown in .
Figure 1. Flow diagram of included/excluded studies.
Table 1. Characteristics of 10 case-control studies included in meta-analysis
There were 5 case-control studies in Asians (Citation14,15,Citation17,Citation20,Citation22) and 5 in Caucasians (Citation13,Citation16,Citation18,19,Citation21). As shown in , the average age of COPD patients were >60 years-old except 1 study did not mention the age of the population. For the gender difference, we can found that more males than females were included in the meta-analysis for both COPD patients and controls. As for the definition for COPD, 5 case-control studies employ the AST/ERS COPD criteria, 2 used the GLOD criteria, 2 used Chinese COPD criteria and 1 did not present the definition. All case-control studies employed normal/healthy persons as controls.
Quantitative data synthesis
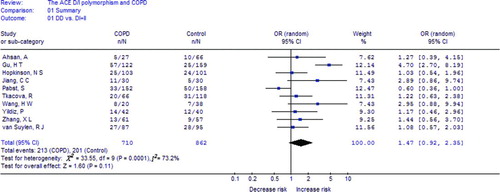
All studies. In , the heterogeneity of DD vs. II+DI for all eighteen studies was analyzed. The value of X2 was 33.55 with 9 degrees of freedom and P = 0.0001 in a random-effects model. Additionally, I-square value is another index of the test of heterogeneity. In , the I-square was 73.2%, suggesting a moderate heterogeneity. Thus, we chose the random-effects model to synthesize the data. Overall, OR was 1.47 (95%CI = 0.92–2.35) and the test for overall effect Z value was 1.60 (P = 0.11) for DD vs. DI+II model. The results suggested that individuals who carry DD homozygote may not have an increased/decreased COPD risk compared with the homozygote II and heterozygote DI.
Figure 2. Meta-analysis with a random-effects model for the association between COPD risk and the ACE D/I polymorphism (DD vs. DI+II).
Subgroup analyses
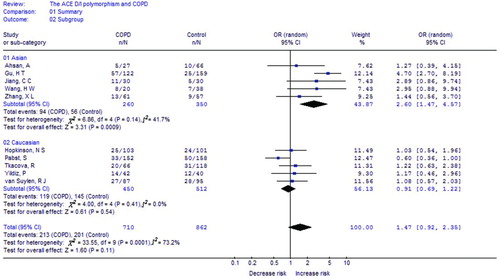
In the subgroup analysis by race, significantly increased risks were found among Asians (OR = 2.60, 95%CI = 1.47–4.57, P = 0.0009 for DD vs. DI+II), but not in Caucasians (OR = 0.91, 95%CI = 0.69–1.22, P = 0.54 for DD vs. DI+II) (). Thus, the Asian DD carriers may have higher risk of COPD than Caucasian DD carriers. As 4 of 5 Asian studies were performed in Chinese population, we also assessed the Chinese population. For the Chinese population, significantly increased risks were found (OR = 3.31, 95%CI = 2.19-5.01, P < 0.00001 for DD vs. DI+II), thus, the ACE gene may take as a susceptible COPD gene for Chinese population.
Figure 3. Meta-analysis with a random-effects model for the association between COPD risk and the ACE D/I polymorphism (DD vs. DI+II): subgroup analysis by race.
Summary results of other genetic comparisons are listed in . Briefly, no significant association was found in the total comparisons. Significant associations were found in Asian population for DD vs. II comparative(OR = 2.62, 95%CI = 1.51-4.55, P = 0.0007) and D vs. I comparative(OR = 1.66, 95%CI = 1.15-2.39, P = 0.007) (). In contract, no significant association was found in Caucasian population.
Table 2. Summary of different comparative results
Publication bias
Publication bias was assessed by Begg's funnel plot and Egger's test. The shape of the funnel plots seemed symmetrical in the DD vs. II+DI comparison genetic model, suggesting the absence of publication bias (). Then, the Egger's test was performed to provide statistical evidence of funnel plot asymmetry. The results indicated a lack of publication bias of the current meta-analysis (t = 0.61, P = 0.557).
Figure 4. Begg's funnel plot for publication bias in selection of studies on the ACE D/I polymorphism (DD vs. DI+II).
Sensitivity analysis
To assess the stability of the results of the current meta-analysis, we performed sensitivity analysis by sequentially excluding each study. Statistically similar results were obtained after sequentially excluding each study expect for the Pabst's study (Citation18), suggesting the stability of our meta-analysis is affected by Pabst's study.
Discussion
The current meta-analysis, including a total of 710 COPD patients and 862 controls from 10 case-control studies, investigated the association between one polymorphism within the ACE gene and COPD risk. Our results indicated that the DD homozygote carriers did not have an increased or decreased risk of COPD. However, after subgroup analysis by race, significant increased risk of COPD were found among Asians, but not in Caucasians. There were several reasons which might account for the differences. First, different genetic backgrounds may account for these differences. Second, the living environment for Asians and Caucasians might be different, and these differences may account for the different genetic effects. Although we found a significant association between the D/I polymorphism and COPD risk in Asians, the results should be explained with caution, because most of the included studies were from China. Thus, in future, more studies should be recruited to analyze these results.
In the sensitivity analysis, statistically similar results were obtained after sequentially excluding each study expect for the Pabst's study. As to the Pabst's study, the employed cases and controls in Germans, this suggested that that study may affect the stability of the results. Because the Pabst's study did not included in the Asian subgroup, the results for the Asians might be more stable than those for the Caucasians.
We also have to mention the importance of heterogeneity. Heterogeneity is an important issue when interpreting the results of meta-analysis. Significant heterogeneity existed in overall comparison in the recessive model. After subgroup analyses by race, the heterogeneity was decreased in Asians and removed in Caucasians, suggesting the race differences may account for the heterogeneity. Another important factor contributing to heterogeneity was the homogeneity for cases and controls. Ideally, all cases and controls should be matched for age, sex, environmental exposures, smoking stage, lung functions and stable/exacerbation situation. However, these items could not be explained, because insufficient information could be extracted from the original studies. In addition, as for the publication bias analysis, although no significant publication bias was found by the Begg's funnel plots and Egger's test, the results should also be explained with caution, because interpreting the p value in setting of significant heterogeneity between studies and relatively small number of studies might be limited.
We also have to mention the definitions of COPD patients and controls. Because the COPD phenotype is very heterogeneous and the progression of disease severity may be associated with pulmonary vascular disease, ideally, the COPD phenotype for each COPD patients should be known and the data should also be analyzed. In addition, it is important to know the smoking status of the COPD patients and controls. Weather the controls were smokers or healthy non-smokers? These questions should also be known. In this meta-analysis, due to lack of these original data, we could not analyze these issues. Future case-control studies which included all these issues may help to resolve these questions.
Some limitations of this meta-analysis should be considered when explaining the results. First, all case-control studies were from Asians and Caucasians, so our results may be applicable to these two race groups only. In addition, there was no study concerning the Africans or the Latinos, thus, future studies are needed to investigate the association between the ACE D/I polymorphism and COPD risk. Second, because only studies included by the selected databases were included for data analysis, some relevant published studies or unpublished studies with null results were missed, which might bias our results. Third, due to the limitation of the original information for individuals, data were not stratified by other variables, such as, gender, PaCO2, PaO2, FEV1%, SaO2, the smoking status and the complication of COPD. Fourth, the small sample sizes (<100 cases or controls) may limited the results of our study.
Despite of these limitations, our study has some advantages. First, it is the most comprehensive study for this polymorphism and COPD risk by meta-analysis. Second, it is the first time to study the race specific and ACE D/I polymorphism interactions. Third, the methodological issues for meta-analysis, such as, heterogeneity, publication bias, stability of results were all well investigated.
This study is the most comprehensive meta-analysis to date to have assessed the relationship between the ACE D/I polymorphism and COPD risk. In conclusion, the meta-analysis suggested that the ACE D/I polymorphism is associated with increased risk of COPD in Asians but not in Caucasians. Future large-scale studies are needed to validate these conclusions.
Declaration of Interest
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
References
- Soriano JB, Rodriguez-Roisin R. Chronic Obstructive Pulmonary Disease Overview: Epidemiology, Risk Factors, and Clinical Presentation. In: Am Thoracic Soc; 2011:363.
- Halpin D. Mortality in COPD: inevitable or preventable? Insights from the cardiovascular arena. COPD 2008;5:187–200.
- Bracke KR, Dentener MA, Papakonstantinou E, Enhanced deposition of low-molecular-weight hyaluronan in lungs of cigarette smoke-exposed mice. Am J Resp Cell Mol 2010;42:753.
- Hallberg J, Dominicus A, Eriksson UK, Interaction between smoking and genetic factors in the development of chronic bronchitis. Am J Resp Crit Care 2008;177:486.
- Smolonska J, Wijmenga C, Postma DS, Boezen HM. Meta-analyses on suspected COPD genes-a summary of 20 years’ research. Am J Resp Crit Care 2009:200722–200905.
- Sørheim IC, DeMeo DL, Washko G, Polymorphisms in the Superoxide Dismutase-3 Gene Are Associated with Emphysema in COPD. COPD 2010;7:262–268.
- Lee J, Nordestgaard BG, Dahl M. EPHX1 polymorphisms, COPD and asthma in 47,000 individuals and in meta-analysis. Eur Respir J 2011;37:18.
- Zhong L, Zhang YP, Fu WP, The Relationship between GSTP1 I105V Polymorphism and COPD: A Reappraisal. Am J Resp Crit Care 2010;181:763.
- Shukla RK, Kant S, Bhattacharya S, Mittal B. Association of Genetic Polymorphism of GSTT1, GSTM1 and GSTM3 in COPD Patients in a North Indian Population. COPD 2011;8:167–172.
- Zhan P, Wang J, Wei SZ, TNF-308 gene polymorphism is associated with COPD risk among Asians: meta-analysis of data for 6,118 subjects. Mol Biol Rep 2011;38:219–227.
- Zhang X, Wang C, Dai H, Lin Y, Zhang J. Association between angiotensin-converting enzyme gene polymorphisms and exercise performance in patients with COPD. Respirology 2008;13:683–688.
- van Suylen RJ, Wouters EF, Pennings HJ, The DD genotype of the angiotensin converting enzyme gene is negatively associated with right ventricular hypertrophy in male patients with chronic obstructive pulmonary disease. Am J Resp Crit Care 1999;159:1791.
- Kanazawa H, Okamoto T, Hirata K, Yoshikawa J. Deletion polymorphisms in the angiotensin converting enzyme gene are associated with pulmonary hypertension evoked by exercise challenge in patients with chronic obstructive pulmonary disease. Am J Resp Crit Care 2000;162:1235.
- Ahsan A, Ram R, Baig MA, Pasha MA. ACE I allele and eNOS G allele crosstalk may have a role in chronic obstructive pulmonary disease. Clin Biochem 2004;37:1037–1040.
- Gu HT, Zhang HS, Yang L. Relationship between polymorphism in the angiotensin converting enzyme gene and susceptibility to COPD(Chinese). Ji Chu Yi Xue Yu Lin Chuang 2003;23:174–177.
- Hopkinson NS, Nickol AH, Payne J, Angiotensin converting enzyme genotype and strength in chronic obstructive pulmonary disease. Am J Resp Crit Care 2004;170:395.
- Jiang CC, Zhang LH. The correlation between the polymorphism of angiotensin-converting enzyme gene and the risk of COPD(Chinese). Guo Wai Yi Xue Lin Chuang Sheng Wu Hua Xue Yu Jian Yan Xue Fen Ce 2002;23:248–249.
- Pabst S, Theis B, Gillissen A, Angiotensin-converting enzyme I/D polymorphism in chronic obstructive pulmonary disease. Eur J Med Res 2009;14:177.
- Tkáčová R, Joppa P, Stančák B, The link between angiotensin-converting enzyme genotype and pulmonary artery pressure in patients with COPD. Wien Klin Wochenschr 2005;117:210–214.
- Wang HW, Nie ZS, Duan YZ, The correlation between the polymorphism of angiotensin-converting enzyme gene and the risk of lung cancer and COPD(Chinese). Hai Jun Zong Yi Yuan Xue Bao 2000;13:203–206.
- Yildiz P, Oflaz H, Cine N, Gene polymorphisms of endothelial nitric oxide synthase enzyme associated with pulmonary hypertension in patients with COPD. Resp Med 2003;97:1282–1288.
- Zhang X, Wang C, Dai H, Lin Y, Zhang J. Association between angiotensin-converting enzyme gene polymorphisms and exercise performance in patients with COPD. Respirology 2008;13:683–688.
- Chapman KR, Stockley RA, Dawkins C, Wilkes MM, Navickis RJ. Augmentation therapy for α1 antitrypsin deficiency: a meta-analysis. COPD 2009;6:177–184.
- Zhang YG, Li XB, Zhang J, The I/D polymorphism of angiotensin-converting enzyme gene and asthma risk: a meta-analysis. Allergy 2011;66:197–205.