
To the Editor:
We would like to address our concerns regarding the safety of ibogaine, after a case of a cardiac arrest following ibogaine use in a young, previously healthy man admitted to our hospital.
Ibogaine is an indole alkaloid derived from the West African plant Tabernanthe Iboga.Citation1 It is used by indigenous people for hallucinogenic properties and to reduce hunger and fatigue. There is special interest for its presumed anti-addictive properties. Various intoxications with ibogaine have been described, some with a fatal outcome.Citation2
In our hospital, a previously healthy 26-year-old man (74 kg) presented after an out-of-hospital cardiac arrest based on ventricular fibrillation, approximately 5 h after taking 2400 mg of ibogaine for a spiritual experience. Basic life support was initiated immediately and he was defibrillated. Return of spontaneous circulation occurred after 20 min. After arriving into hospital he remained comatose (Glasgow Coma Scale [GCS] score 3, E1M1V1[tube]) on midazolam and propofol. He received therapeutic hypothermia, mechanical ventilation and fluid resuscitation. The physical examination revealed no abnormalities besides decreased GCS score. His potassium serum level was 4.0 mmol/l [ref 3.5–5.0]. No other abnormalities in blood tests were found. His ECGs showed a prolonged QTc interval from admission up to 32 h, with a maximum up to 663 ms, 18 h after his cardiac arrest. A recent ECG, performed before ibogaine ingestion, showed a normal QTc.
Toxicological screening revealed benzodiazepines (received during resuscitation in the ED) and ibogaine. The serum level of ibogaine was 948 ug/L 5 h after ingestion as analyzed using LC-MS/MS ().
Fig. 1. Serum concentration–time curve of ibogaine in our patient (colour version of this figure can be found in the online version at www.informahealthcare.com/ctx).
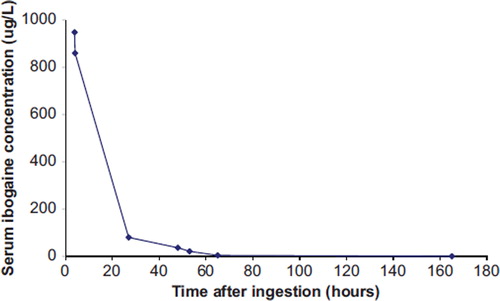
Earlier case reports on ibogaine intoxications described a wide range of serum concentrations (i.e. 360–10800 ug/L).Citation3,Citation4
In ICU he developed seizures for which he was treated with anti-epileptics (phenytoin, valproic acid and levetiracetam). A cerebral CT showed no abnormalities. After 8 days, he was transferred to another hospital with a GCS score of 4 (E1M2V1[tube]) without sedation. Several weeks later he was awake and able to communicate, but permanent cognitive and neurologic deficits (loss of vision) remained, most likely due to post anoxic encephalopathy.
We propose a direct relationship between the ventricular fibrillation and the ingestion of ibogaine, because our patient was previously healthy with a normal cardiology exam prior to the ibogaine use. There was no suspicion of other drugs/medication taken by the patient. The QTc prolongation might in part have been caused or exacerbated by propofol or hypothermia; but ibogaine is well known for its QTc prolongation.Citation5 Recent findings suggest that hERG channel blockade by ibogaine as partial opioid agonist may be the pharmacological mechanism of QTc prolongation.Citation6 The hERG channel is a potassium channel involved in repolarisation of the cardiac action potential. Mutations or blockade of this channel by pharmacologically active compounds can result in prolonged QTc.Citation7,Citation8
Ibogaine is available in different pharmaceutical forms (powders and oral capsules in more or less purified forms). Its use is not wide spread, however, the effects can be devastating and its use should therefore be strongly discouraged.
Declaration of interest
The authors report no declarations of interest. The authors alone are responsible for the content and writing of the paper.
References
- Mash DC, Kovera CA, Pablo J, Tyndale RF, Ervin FD, Williams IC, et al. Ibogaine: complex pharmacokinetics, concerns for safety, and preliminary efficacy measures. Ann N Y Acad Sci 2000; 914:394–401.
- Alper KR, Stajic M, Gill JR. Fatalities temporally associated with the ingestion of ibogaine. J Forensic Sci 2012; 57:398–412.
- Kontrimaviciūte V, Mathieu O, Mathieu-Daudé JC, Vainauskas P, Casper T, Baccino E, et al. Distribution of ibogaine and noribogaine in a man following a poisoning involving root bark of the Tabernanthe iboga shrub. J Anal Toxicol 2006; 30:434–440.
- Chèze M, Lenoan A, Deveaux M, Pépin G. Determination of ibogaine and noribogaine in biological fluids and hair by LC-MS/MS after Tabernanthe iboga abuse Iboga alkaloids distribution in a drowning death case. Forensic Sci Int 2008; 176:58–66.
- Hoelen DW, Spiering W, Valk GD. Long-QT syndrome induced by the anti-addiction drug Ibogaine. N Engl J Med 2009; 360:308–309.
- Thurner P, Stary-Weinzinger A, Gafar H, Gawali VS, Kudlacek O, Zezula J, et al. Mechanism of hERG channel block by the psychoactive indole alkaloid ibogaine. J Pharmacol Exp Ther 2014; 348:346–358.
- Sanguinetti MC, Jiang C, Curran ME, Keating MT. A mechanistic link between an inherited and an acquired cardiac arrhythmia: HERG encodes the IKr potassium channel. Cell 1995; 81:299–307.
- Redfern WS, Carlsson L, Davis AS, Lynch WG, MacKenzie I, Palethorpe S, et al. Relationships between preclinical cardiac electrophysiology, clinical QT interval prolongation and torsade de pointes for a broad range of drugs: evidence for a provisional safety margin in drug development. Cardiovasc Res 2003; 58:32–45.