Abstract
Background and purpose Hip arthroplasty is an option for elderly patients with osteoporosis for the treatment of failure after fixation of trochanteric and subtrochanteric fractures, either as a total hip arthroplasty (THA) or as a hemiarthroplasty (HA). We analyzed the reoperation rate and risk factors for reoperation in a consecutive series of patients.
Methods All patients (n = 88) operated from 1999 to 2006 with a THA (n = 63) or an HA (n = 25) due to failure of fixation of a trochanteric fracture (n = 63) or subtrochanteric fracture (n = 25) were included. Background data were collected from the patient records. A search was performed in the national registry of the Swedish National Board of Health and Welfare in order to find information on all reoperations. The follow-up time was 5–11 years.
Results The reoperation rate was 16% (14/88 hips). A periprosthetic fracture occurred in 6 patients, a deep prosthetic infection in 5 patients, and a dislocation of the prosthesis in 3 patients. Standard-length femoral stems had an increased risk of reoperation (11/47) compared to long stems (3/41) (HR = 4, 95% CI: 1.0–13; p = 0.06).
Interpretation The high reoperation rate reflects the complexity of the surgery. Using long femoral stems that bridge previous holes and defects may be one way to reduce the risk for reoperation.
The standard treatment for trochanteric and subtrochanteric femoral fractures is internal fixation (IF). When fixation failure occurs, the surgical options include re-osteosynthesis or prosthetic replacement. While re-osteosynthesis may be used in younger patients with good bone quality, a prosthetic replacement is preferred in elderly patients with osteoporotic bone, either as a total hip arthroplasty (THA) or as a hemiarthroplasty (HA) (Mariani and Rand Citation1987, Sarathy et al. Citation1995, Said et al. Citation2006). In the elderly patient with low functional demands and an intact acetabulum, an HA is an option, whereas a THA is an optimal alternative for a lucid patient with long life expectancy and higher functional demands (Hedbeck et al. Citation2011). In the case of failure with screw cutout and destruction of the acetabular cartilage, a THA must be performed if acceptable hip function is to be restored, irrespective of the status of the patient. A prosthesis operation after a failed trochanteric or subtrochanteric fracture is a challenge for the surgeon because of several factors such as: altered anatomy due to the primary fracture, nonunion, malunion, bone loss, holes from previous implant, and poor bone quality. Despite this, few authors have described the surgical outcome in these patients and the studies have usually only involved a few patients (Mehlhoff et al. Citation1991, Haidukewych and Berry Citation2003, Waddell et al. Citation2004, Zhang et al. Citation2004, Laffosse et al. Citation2007, Exaltacion et al. Citation2011, Thakur et al. Citation2011).
We wanted to determine the reoperation rate and risk factors for reoperation of secondary hip replacement after failed fixation of trochanteric and subtrochanteric fractures in the context of a large cohort study involving consecutive patients, with a medium- to long-term follow-up time.
Patients and methods
Approximately 3,600 patients were operated at the Department of Orthopaedics at Stockholm Söder Hospital between January 1, 1999 and December 31, 2006 due to a trochanteric or subtrochanteric femoral fracture. All patients were registered in a clinical audit database. Until August 31, 2011, a total of 88 secondary hip arthroplasties had been performed after failure of the fracture treatment, and they were included in this study. All patients had undergone a primary operation with internal fixation of the fracture. No pathological fractures were included.
In addition to the audit data, all individual patient records were searched until August 31, 2011, or death, in order to find information about all reoperations. Finally, the Swedish personal identification number was used to perform a search in the national registry of the National Board of Health and Welfare to find patients who had been treated elsewhere in Sweden for a reoperation up to August 31, 2011. No such cases were found. The median follow-up time was 4.0 (0–11) years for all cases, and 7.9 (4.9–11) years for those who were still alive on August 31, 2011.
The mean (range) age at the primary operation was 83 (63–95) years for women (n = 76) and 81 (54–93) years for men (n = 12). The indication for the primary procedure was a trochanteric femoral fracture in 63 patients, and a subtrochanteric femoral fracture in 25 patients. The standard implant was a plate with a sliding hip screw (SHS) (Synthes, West Chester, PA) for stable 2-part trochanteric fractures. Unstable 3- to 4-part trochanteric fractures and subtrochanteric fractures were treated with a short Gamma nail (SGN), a long Gamma nail (LGN) (Stryker Howmedica, Kalamazoo, MI), or a Medoff sliding plate (Swemac, Linköping, Sweden) ().
Table 1. Baseline data for all patients included (n = 88)
The median time between the primary IF operation and the secondary prosthesis operation was 5 (0.2–45) months. The most common indication for the secondary operation was a cutout of the sliding screw due to a fracture nonunion or femoral head necrosis (n = 59), followed by nonunion (n = 21), femoral head necrosis (n = 6), posttraumatic osteoarthritis (n = 1), and unacceptable implant position and fracture reduction (n = 1).
The prosthesis type used for the secondary operation was a THA in 63 patients and an HA in 25 patients. In the HA patients, the prosthesis used was a cemented Exeter HA with a unipolar Universal Head Replacement (n = 7) or a bipolar Bicentric Head with a 28-mm head (n = 18) (Stryker Howmedica, Kalamazoo, MI). Standard-length femoral stems were used in 47 of the hips, and long femoral stems in 41 (). An anterolateral surgical approach (Hardinge Citation1982) with the patient in a lateral position was used in 53 patients, and a posterolateral surgical approach (Moore Citation1957) with the patient in a lateral position was used in 35 patients. The total numbers of surgeons were 29 (23 consultants and 6 registrars).
Table 2. Secondary prostheses used for all patients who were operated upon using a THA (n = 63)
The patients were mobilized on the day after surgery using crutches and allowed to bear weight as tolerated.
The study was approved by the Regional Ethics Committee in Stockholm June 15, 2011 (reference no. 2011/836-31/3).
Statistics
Nominal variables were tested 2-sided by Fisher’s exact test. We used Cox regression to evaluate factors associated with reoperation risk. Primary fracture type, primary implant type, secondary prosthesis type, femoral stem length, and surgical approach were tested as independent factors in the model. First, crude associations for each factor were studied in univariable models. Secondly, a multivariable model with all independent factors was used to study the adjusted associations. The associations are presented as hazard ratios (HRs) with 95% confidence intervals (CIs). The results were considered significant at p-values < 0.05. The statistical software used was PASW Statistics 18 for Windows.
Results
Reoperations (including closed reduction of prosthetic dislocation) were performed in 14 of the 88 hips, giving a total reoperation rate of 16%. Of these reoperations, a periprosthetic femoral fracture () was the cause in 6 patients, a deep prosthetic infection in 5 patients, and a dislocation of the prosthesis in 3 patients. The periprosthetic fractures occurred late (2–59 months) after surgery, in contrast to dislocations and deep infections which all occurred within the first 2 months of the prosthesis operation ().
A. A 72-year-old women (patient 6) who was operated with a cemented Exeter THA with a standard-length femoral stem, and who sustained a periprosthetic femoral fracture. B. The same patient after reoperation with stem revision and plate osteosynthesis.
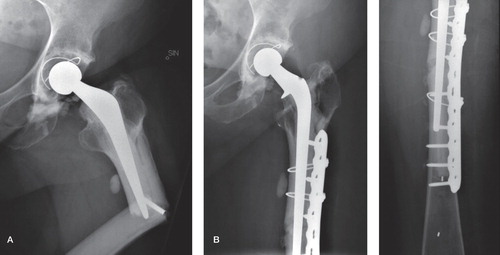
Table 3. Patients with reoperations of the secondary prosthesis (n = 14)
Of the 6 patients who sustained a periprosthetic fracture, 4 patients were reoperated with open reduction and internal fixation with plate osteosynthesis, and 2 patients were reoperated with a revision to a longer femoral stem—1 of whom also had a plate osteosynthesis performed (). Of the 5 patients with deep infection, 4 were successfully treated with debridements (1 to 3 times) plus antibiotics. In 1 patient, the prosthesis was extracted permanently due to persistent infection despite debridement and antibiotic treatment. Of the 3 patients who had a dislocation of the prosthesis, 2 underwent a successful closed reduction and had no recurrent dislocations. In the third patient, a closed reduction failed. In the subsequent open procedure, the stem was found to be loose and was therefore revised using cement-in-cement fixation. No further dislocations occurred in this patient.
A primary analysis showed an increased risk of reoperation when using standard-length femoral stems (11/47), compared to long stems (3/41) (p = 0.05). However, this difference in risk was not statistically significant when multivariable Cox regression analysis was performed adjusting for fracture type, primary implant type, prosthesis type, and surgical approach: HR = 4 (1.0–13) (p = 0.06) (). Of the 6 patients who sustained a periprosthetic fracture, 5 were primary operated using standard-length stems and 1 patient had a long stem.
Table 4. Baseline data in relation to the occurrence of reoperation
There was no statistically significant difference in the reoperation rate of the prosthesis between primary trochanteric and subtrochanteric fractures, or between the primary implant types: intramedullary nails (SGN and LGN) and plates (SHS and Medoff plate), between THAs and HAs, or between the anterolateral and the posterolateral surgical approaches (). There was no difference in the incidence of reoperations between operations performed by consultants (13/82) and those performed by registrars (1/6).
The mean operative time for the prosthesis surgery was 153 (75–355) min, and mean intraoperative blood loss was 1.1 (0.3–3.9) L.
The 6-month mortality was 8%, and the 1-year mortality was 16%. Other adverse events occurring within 6 weeks included a stroke in 3 patients (1 fatal), a cardiac infarction in 2 patients (1 fatal), and a pneumonia, a deep vein thrombosis, a peroneal nerve palsy, and extensive decubital ulcers in 1 patient each.
Discussion
Our main finding, a reoperation rate of 16%, highlights the challenges in the treatment of patients with failure after internal fixation of trochanteric and subtrochanteric fractures. As a comparison, Bonnevialle et al. (Citation2011) recently reported a reoperation rate of 3% in a prospective study of 106 patients followed for at least 6 months after an arthroplasty performed as a primary procedure due to a trochanteric fracture. These figures can also be compared to a previously published study from our department on patients with femoral neck fractures, where the reoperation rate was 13% in 154 secondary HAs after failed IF, as compared to 5% for 676 primary HAs (Enocson et al. Citation2011). A similar finding has been reported by Roberts and Parker (Citation2002) in a prospective cohort study of patients operated upon with an uncemented Austin-Moore HA due to a femoral neck fracture. They found an increased risk of reoperation (12% vs. 4%) in 100 patients with a secondary prosthesis as compared to 730 patients with a primary one. All these results confirm the high reoperation rate after secondary hip arthroplasty, and with respect to the difficulties, we recommend that this surgical procedure should be performed only by experienced surgeons.
Another finding was that standard-length femoral stems were associated with a higher risk of reoperation than long stems. A periprosthetic fracture was the most common reason for reoperation (6/88 patients), and this is probably associated with stem length, as 5 of these 6 patients were operated with standard-length femoral stems—as compared to 47/88 for the whole cohort. Our results can also be compared with those of Haidukewych and Berry (Citation2003), who reported on 44 patients who were followed for 2–15 years after a secondary arthroplasty due to failed trochanteric fractures. Their total reoperation rate (including closed reduction of dislocated hips) was 5/44, but this included only 1 patient with a postoperative periprosthetic fracture. It is possible that the fact that they used standard femoral stems in only 9 of their patients reduced the risk of periprosthetic fractures. In contrast, Zhang et al. (Citation2004) reported no postoperative periprosthetic fractures, but 6 intraoperative fractures in 19 patients who were operated using standard-length stems. Furthermore, Exaltacion et al. (Citation2011) described 20 patients with secondary arthroplasties who were primarily treated with intramedullary nails. During the 12-month follow-up, they found 9 patients with a fracture of the greater trochanter and 2 patients who were reoperated with exchange of the acetabular component due to loosening and dislocations, respectively. Periprostheic fractures are obviously a major problem for these patients, and we believe that it is of vital importance to bridge previous defects and holes in the femur to reduce the risk.
The low incidence of prosthetic dislocations in our study (3/88) is probably explained by the fact that more than half of the patients were operated through an anterolateral approach. We have previously reported that the posterolateral surgical approach is associated with a higher risk of dislocations after femoral neck fractures than with the anterolateral approach (Enocson et al. Citation2008, Citation2009). The current results correspond well with our previous findings, where there was a dislocation rate of 6% for both HA patients (Enocson et al. Citation2008) and THA patients (Enocson et al. Citation2009) in large series involving both antero- and posterolateral approaches.
A deep infection occurred in 5 patients. This is in line with a study by Exaltacion et al. (Citation2011) on arthroplasty patients after failed trochanteric fractures, and also studies on patients with femoral neck fractures (Calder et al. Citation1996, Baker et al. Citation2006, Frihagen et al. Citation2007). Other authors such as Mehlhoff et al. (Citation1991) and Laffosse et al. (Citation2007) reported no deep infections in arthroplasty patients after failed trochanteric fractures. The wide range of the reported incidence of infections after hip arthroplasty may be explained at least in part by different definitions.
Not surprisingly, the intraoperative blood loss (mean 1.1 L) and the operating times (mean 153 min) are both considerably higher than after primary hip arthroplasty, but they correspond well with those in revision hip arthroplasty surgery in general (Bozic et al. Citation2005) and reflect the complexity of the surgery. The high incidence of other severe adverse events (10%), including fatal events of stroke and cardiac infarction, not only reflects the complexity but also the general risk of the surgery.
One limitation of our study was the lack of postoperative assessment of functional outcome. The strengths of the study were the large number of consecutively included patients, the relatively long follow-up period, and the validation of reoperation and dislocation data via the nationwide registry of the Swedish National Board of Health and Welfare. We therefore have good reason to assume that our conclusions for this patient cohort are valid.
AE and LL designed the study. AE, LM, CO, and LL gathered the data, analyzed it, and wrote the manuscript.
No competing interests declared.
- Baker RP, Squires B, Gargan MF, Bannister GC. Total hip arthroplasty and hemiarthroplasty in mobile, independent patients with a displaced intracapsular fracture of the femoral neck. A randomized, controlled trial. J Bone Joint Surg (Am) 2006; 88 (12): 2583-9.
- Bonnevialle P, Saragaglia D, Ehlinger M, Tonetti J, Maisse N, Adam P, Le Gall C. Trochanteric locking nail versus arthroplasty in unstable intertrochanteric fracture in patients aged over 75 years. Orthop Traumatol Surg Res (6 Suppl) 2011; 97: S95-100.
- Bozic KJ, Katz P, Cisternas M, Ono L, Ries MD, Showstack J. Hospital resource utilization for primary and revision total hip arthroplasty. J Bone Joint Surg (Am) 2005; 87 (3): 570-6.
- Calder SJ, Anderson GH, Jagger C, Harper WM, Gregg PJ. Unipolar or bipolar prosthesis for displaced intracapsular hip fracture in octogenarians: a randomised prospective study [see comments]. J Bone Joint Surg (Br) 1996; 78 (3): 391-4.
- Enocson A, Tidermark J, Törnkvist H, Lapidus LJ. Dislocation of hemiarthroplasty after femoral neck fracture: better outcome after the anterolateral approach in a prospective cohort study on 739 consecutive hips. Acta Orthop 2008; 79 (2): 211-7.
- Enocson A, Hedbeck C-J, Tidermark J, Pettersson H, Ponzer S, Lapidus LJ. Dislocation of total hip replacement in patients with fractures of the femoral neck. A prospective cohort study on 713 consecutive hips. Acta Orthop 2009; 80 (2): 184-9.
- Enocson A, Hedbeck CJ, Törnkvist H, Tidermark J, Lapidus LJ. Unipolar versus bipolar Exeter hip hemiarthroplasty: a prospective cohort study on 830 consecutive hips in patients with femoral neck fractures. Int Orthop 2011; 26: Epub ahead of print.
- Exaltacion JJ, Incavo SJ, Mathews V, Parsley B, Noble P. Hip Arthroplasty After Intramedullary Hip Screw Fixation: A Perioperative Evaluation. J Orthop Trauma 2011; 18: Epub ahead of print.
- Frihagen F, Nordsletten L, Madsen JE. Hemiarthroplasty or internal fixation for intracapsular displaced femoral neck fractures: randomised controlled trial. Bmj 2007; 335 (7632): 1251-4.
- Haidukewych GJ, Berry DJ. Hip arthroplasty for salvage of failed treatment of intertrochanteric hip fractures. J Bone Joint Surg (Am) 2003; 85 (5): 899-904.
- Hardinge K. The direct lateral approach to the hip. J Bone Joint Surg (Br) 1982; 64 (1): 17-9.
- Hedbeck CJ, Enocson A, Lapidus G, Blomfeldt R, Törnkvist H, Ponzer S, Tidermark J. Comparison of bipolar hemiarthroplasty with total hip arthroplasty for displaced femoral neck fractures: a concise four-year follow-up of a randomized trial. J Bone Joint Surg (Am) 2011; 93 (5): 445-50.
- Laffosse JM, Molinier F, Tricoire JL, Bonnevialle N, Chiron P, Puget J. Cementless modular hip arthroplasty as a salvage operation for failed internal fixation of trochanteric fractures in elderly patients. Acta Orthop Belg 2007; 73 (6): 729-36.
- Mariani EM, Rand JA. Nonunion of intertrochanteric fractures of the femur following open reduction and internal fixation. Results of second attempts to gain union. Clin Orthop 1987; (218): 81-9.
- Mehlhoff T, Landon GC, Tullos HS. Total hip arthroplasty following failed internal fixation of hip fractures. Clin Orthop 1991; (269): 32-7.
- Moore AT. The self-locking metal hip prosthesis. J Bone Joint Surg (Am) 1957; 39 (4): 811-27.
- Roberts C, Parker MJ. Austin-Moore hemiarthroplasty for failed osteosynthesis of intracapsular proximal femoral fractures. Injury 2002; 33 (5): 423-6.
- Said GZ, Farouk O, El-Sayed A, Said HG. Salvage of failed dynamic hip screw fixation of intertrochanteric fractures. Injury 2006; 37 (2): 194-202.
- Sarathy MP, Madhavan P, Ravichandran KM. Nonunion of intertrochanteric fractures of the femur. Treatment by modified medial displacement and valgus osteotomy. J Bone Joint Surg (Br) 1995; 77 (1): 90-2.
- Thakur RR, Deshmukh AJ, Goyal A, Ranawat AS, Rasquinha VJ, Rodriguez JA. Management of failed trochanteric fracture fixation with cementless modular hip arthroplasty using a distally fixing stem. J Arthroplasty 2011; 26 (3): 398-403.
- Waddell JP, Morton J, Schemitsch EH. The role of total hip replacement in intertrochanteric fractures of the femur. Clin Orthop 2004; (429): 49-53.
- Zhang B, Chiu KY, Wang M. Hip arthroplasty for failed internal fixation of intertrochanteric fractures. J Arthroplasty 2004; 19 (3): 329-33.