Abstract
Background and purpose For 20 years, medical treatment of rheumatoid arthritis (RA) has been improving and the incidence of joint surgery has decreased. We investigated the rates of primary ankle joint arthrodesis and total ankle arthroplasty in patients with RA in Finland between 1997 and 2010 to establish whether trends have changed during that period.
Methods The annual figures for primary ankle joint arthrodeses and total ankle replacements performed in patients with RA were obtained from nationwide population-based registries. Incidences were calculated per population of 105 and they are reported in 2-year periods.
Results During the study period, 593 primary ankle joint arthrodeses and 318 total ankle arthroplasties were performed in patients with RA. The incidence of ankle joint arthrodesis reached its highest value (2.4/105) in 1997–1998 and it was lowest in 2001–2002 (1.1/105). After 2002, the incidence increased slightly but did not reach the level in 1997–1998, even though total ankle replacements almost ended in Finland during the period 2009–2010. From 1997, total ankle replacements increased until 2003–2004 (incidence 1.5/105) and then gradually decreased. In 2009–2010, the incidence of total ankle replacements was only 0.4/105.
Interpretation During the observation period 1997–2010, while total ankle replacements generally became more common in patients with RA, the incidence of primary ankle joint arthrodesis decreased and did not increase in the period 2009-2010, even though total ankle replacement surgery almost ended in Finland. No change in the incidence of these operations, when pooled together, was observed from 1997 to 2010.
In rheumatoid arthritis (RA), an alternative to ankle joint arthrodesis is total ankle arthroplasty (TAA). TAA preserves joint motion and function, with protection of other joints (Valderrabano et al. Citation2003, Doets et al. Citation2007, Piriou et al. Citation2008). Currently, the main indications for TAA are end-stage idiopathic, inflammatory, and post-traumatic osteoarthritis (Rydholm Citation2007, Skyttä et al. Citation2010, Henricson et al. Citation2011).
During the past 2 decades, medical treatment for RA has improved. Studies from different countries have suggested that rates of joint replacement in RA have decreased in recent years (Da Silva et al. Citation2003, Kobelt et al. Citation2004, Ward Citation2004, Pedersen et al. Citation2005, Weiss et al. Citation2006, Citation2008, Sokka et al. Citation2007, Momohara et al. Citation2010, Jämsen et al. Citation2013). However, there have only been a few studies on the incidence of ankle joint arthrodesis and TAA in patients with RA (Fevang et al. Citation2007, Louie and Ward Citation2010).
Using data from nationwide population-based registries, we determined the rates of primary ankle joint arthrodesis and TAA in patients with RA in Finland, 1997–2010.
Patients and methods
The annual figures for primary ankle joint (talocrural) arthrodesis were obtained from the Finnish Hospital Discharge Register, based on RA-related diagnosis codes M05–M09 and M45 according to ICD-10 classification, and appropriate surgical procedure codes (NHG20) according the Nordic Medico-Statistical Committee classification. The annual figures for TAA were collected from the Finnish Arthroplasty Register (based on obligatory reports by operating units).
The incidences of primary ankle joint arthrodesis and TAA, and the sum for both operations, were calculated per population of 105 (with respective 95% confidence intervals (CIs), calculated according to Wilson’s method).
As the prevalence of rheumatoid arthritis cannot be derived from any nationwide Finnish register, the incidences were calculated for the general population, which makes comparison of incidences between RA and other diagnoses possible. To control for year-to-year variation in operation figures, the incidences were calculated in 2-year periods from 1997 to 2010. The population at the mid-point of each 2-year period was used as denominator in the calculations (derived from the Statistics Finland website, http://pxweb2.stat.fi/database/StatFin/vrm/vaerak/vaerak_en.asp). The statistical significance of the temporal trends observed was tested using general linear regression.
Results
During the study period 1997–2010, 593 primary ankle joint arthrodeses and 318 TAAs were performed for patients with RA (). Within that time period, the population of Finland increased from 5,114,510 to 5,335,481 (4%).
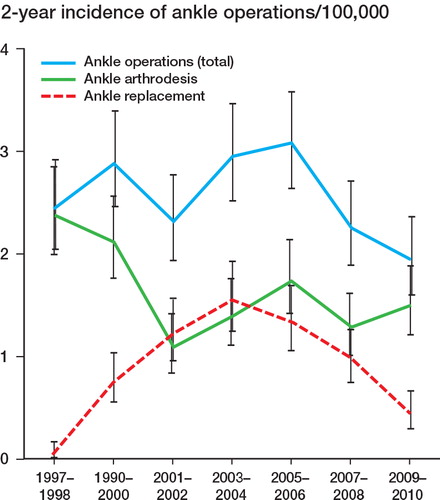
Figure 1. The incidence (per 105 of population) of primary ankle joint arthrodesis, total ankle arthroplasty, and the sum of both in patients with RA, in 2-year periods from 1997 to 2010 (with 95% CIs).
Primary ankle joint arthrodesis
While total ankle replacement surgery became more common, the number of primary ankle joint arthrodeses in patients with RA decreased. In 1997–1998, the incidence of primary ankle joint arthrodesis was 2.4/105 (CI: 2.0–2.8) and in 2001–2002 the incidence was lowest, 1.1/105 (CI: 0.8–1.4). After 2002, it increased slightly, although no statistically significant difference was observed and it did not reach the level of 1997–1998, even though by 2009–2010 the use of TAAs had almost ended.
Total ankle arthroplasty
During the study period, one third of all TAAs in Finland were undertaken due to RA. These were performed in 14 hospitals; annually, only 1 or 2 hospitals performed more than 10 replacements. Altogether, 5 different implants were used: the LINK S.T.A.R. (Waldemar Link, Hamburg, Germany), the AES (Ankle Evolutive System, Valence, France), the Mobility (DePuy, Warsaw, IN), the Hintegra (Newdeal, Lyon, France), and the CCI (Van Straten Medical, the Netherlands). In 2003, there was a shift from the commonly used LINK S.T.A.R. prosthesis to the AES prosthesis.
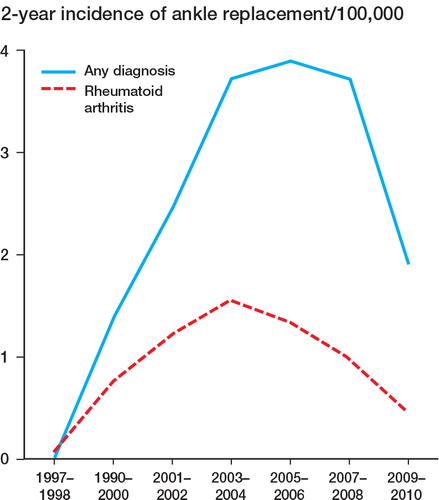
Since 1997, the numbers of TAAs in patients with RA increased (p < 0.001) until 2003–2004 (incidence 1.5/105, CI: 1.3–1.9) and then gradually decreased (p = 0.001). In 2009–2010, the incidence of TAA was only 0.4/105 (CI: 0.3–0.7). The incidence of TAA performed due to any diagnosis followed a similar pattern ().
Figure 2. The incidence (per 105 of population) of total ankle arthroplasty in patients with RA and in patients with any diagnosis (including RA), in 2-year periods from 1997 to 2010.
Regression analysis confirmed the statistical significance of the declining trend in the incidence of primary ankle arthrodesis in patients with RA from 1997 to 2010 (p = 0.04), whereas no change was observed in the total incidence of ankle surgery in patients with RA (primary arthrodesis and TAA, pooled) (p = 0.226).
Discussion
The Finnish Hospital Discharge Register does not contain information on disease onset and disease duration in RA patients. However, since 1995 the Finnish Arthroplasty Register data have been synchronized with the Discharge Register every few years, and currently over 95% of implantations are recorded (Skyttä et al. Citation2010).
By reason of changes in the classification of diagnoses and surgical procedures in the Hospital Discharge Register in 1997, we could not analyze data on arthrodeses from earlier years. Indications for TAA and ankle joint arthrodesis are not entirely consistent. In most severe cases of ankle joint destruction, TAA may be technically impossible and ankle arthrodesis must be used.
Previously, Fevang et al. (Citation2007) reported that in Norway during 1994–2004 the incidence of arthroplasty of the foot had decreased, whereas the opposite was true for arthrodesis of the ankle/foot with chronic inflammatory joint disease. We found a decrease in incidence for total ankle arthroplasties in patients with RA since 2003–2004, and a slight increase in the incidence of primary ankle joint arthrodesis since 2001–2002, but the increase was not statistically significant.
In their study of patients on RA in California 1983–2007, Louie and Ward (Citation2010) found that the rates of ankle surgery (arthrodesis and arthroplasty, pooled) peaked in the mid-1990s. Thereafter, the rates decreased and the relative risk of operative treatment was one third lower in 2003–2007 than in 1983–1987. At the end of our observation period, the numbers of ankle operations (arthrodesis and TAA, pooled) decreased due to the steep drop in TAA surgery.
The first-generation total ankle prostheses were abandoned in the 1980s and 1990s due to unacceptable failure and complication rates (Bolton-Maggs et al. Citation1985, Doets et al. Citation2007). In 1997, a new 3-component design was introduced in Finland and the number of total ankle replacements increased while the numbers of ankle arthrodeses began to decrease. Remarkably, during the study period 5 different implants were used and TAA surgery was done in several hospitals; only a few hospitals performed more than 10 operations annually. Our opinion, although not supported by the present data, is that ankle prosthesis surgery in patients with RA should be centralized to a few hospitals in Finland to give an adequate number of operations per unit and surgeon in order to ensure repetition and quality (Lehto Citation2011).
At the end of the study period 2008–2010, complications were seen with the AES prosthesis as a result of osteolysis (Koivu et al. Citation2009, Kokkonen et al. Citation2011). These observations rapidly changed the practice, and total ankle replacement surgery was almost completely abandoned in Finland. This applied both to TAAs performed for RA and to those performed for other diagnoses. Thus TAAs radically decreased whereas, interestingly, the incidence of ankle joint arthrodesis in patients with RA did not increase.
In Finland, the incidence of rheumatoid factor-positive RA decreased in 1980–2000 (Kaipiainen-Seppänen and Kautiainen Citation2006), but at the moment there is no published evidence of a changing incidence of RA. At the same time, current care guidelines advocate active treatment of RA using drug combinations, and the number of patients receiving anti-rheumatic drugs has increased (The drug registers of the Social Insurance Institution of Finland). This change in the management of RA has been considered to be a major factor underlying the decrease in the rates of hip, knee, elbow, and shoulder replacements (Jämsen et al. Citation2013).
Thus, we can only speculate on what will happen in future. Anti-rheumatic agents will probably reduce the need for ankle surgery, due to the prevention of ankle joint destruction. New prosthesis designs will be developed with expectations of better survival rates.
However, the ankle joint (talocrural) is involved at a late stage of RA and is usually affected only in patients with severe disease (Belt et al. Citation2001). Thus, a longer-term follow-up will be required to explain how improved medical therapy, particularly biological, influences the risk of ankle joint destruction, and whether there are any changes in epidemiology that would affect the need for ankle surgery in RA.
In conclusion, during the observation period 1997–2010, while total ankle replacements became generally more common in patients with RA, the incidence of primary ankle joint arthrodesis decreased and did not increase in 2009–2010, even though total ankle replacement surgery almost ended in Finland. When the data were pooled together, no change in the incidence of these operations was observed in the period 1997–2010.
All 4 authors designed the study. AK and EJ gathered the data. All 4 authors analyzed the data and drafted the initial manuscript. They also ensured the accuracy of the data and analysis, and critically revised the manuscript. All authors read and approved the final manuscript.
No competing interests declared.
- Belt EA, Kaarela K, Mäenpää H, Kauppi MJ, Lehtinen JT, Lehto MU. Relationship of ankle joint involvement with subtalar destruction in patients with rheumatoid arthritis. A 20-year follow-up study. Joint Bone Spine 2001; 68 (2): 154-7.
- Bolton-Maggs BG, Sudlow RA, Freeman MA. Total ankle arthroplasty. A long-term review of the London Hospital experience. J Bone Joint Surg (Br) 1985; 67: 785-90.
- Da Silva E, Doran MF, Crowson CS, O’Fallon WM, Matteson EL. Declining use of orthopedic surgery in patients with rheumatoid arthritis? Results of a long-term, population-based assessment. Arthritis Rheum 2003; 49: 216–20.
- Doets HC, van Middelkoop M, Houdijk H, Nelissen RG, Veeger HE. Gait analysis after successful mobile bearing total ankle replacement. Foot Ankle Int 2007; 28 (3): 313-22.
- Fevang BT, Lie SA, Havelin LI, Engesaeter LB, Furnes O. Reduction in orthopedic surgery among patients with chronic inflammatory joint disease in Norway. 1994–2004. Arthritis Rheum 2007; 15:57 (3): 529-32.
- Henricson A, Nilsson JÅ, Carlsson A. 10-year survival of total ankle arthroplasties: a report on 780 cases from the Swedish Ankle Register. Acta Orthop 2011; 82 (6): 655-9.
- Jämsen E, Virta L, Hakala M, Kauppi MJ, Malmivaara A, Lehto M UK. The decline in joint replacement surgery in rheumatoid arthritis associates with a concomitant increase in the intensity of anti-rheumatic therapy. A nationwide register-based study from 1995 through 2010. Acta Orthop 2013; 84 (4): 331-7.
- Kaipiainen-Seppänen O, Kautiainen H. Declining trend in the incidence of rheumatoid factor-positive rheumatoid arthritis in Finland 1980-2000. J Rheumatol 2006; 33 (11): 2132-8.
- Kobelt G, Eberhardt K, Geborek P. TNF inhibitors in the treatment of rheumatoid arthritis in clinical practice: costs and outcomes in a follow-up study of patients with RA treated with etanercept or infliximab in southern Sweden. Ann Rheum Dis 2004; 63: 4–10.
- Koivu H, Kohonen I, Sipola E, Alanen K, Vahlberg T, Tiusanen H. Severe periprosthetic osteolytic lesions after the Ankle Evolutive System total ankle replacement. J Bone Joint Surg (Br) 2009; 91 (7): 907–14.
- Kokkonen A, Ikävalko M, Tiihonen R, Kautiainen H, Belt EA. High rate of osteolytic lesions in medium-term followup after the AES total ankle replacement. Foot Ankle Int 2011; 32 (2): 168-75.
- Lehto M UK. Nationwide execution of rheumaorthopedics (in Finnish). Report of the Ministry of Social Affairs and Health. 3, 2011. ISBN 958-952-00-3206-7.
- Louie GH, Ward MM. Changes in the rates of joint surgery among patients with rheumatoid arthritis in California. 1983-2007. Ann Rheum Dis 2010; 69 (5): 868-71.
- Momohara S, Inoue E, Ikari K, Kawamura K, Tsukahara S, Iwamoto T, Hara M, Taniguchi A, Yamanaka H. Decrease in orthopaedic operations, including total joint replacements, in patients with rheumatoid arthritis between 2001 and 2007: data from Japanese outpatients in a single institute-based large observational cohort (IORRA). Ann Rheum Dis 2010; 69 (1): 312-3.
- Pedersen AB, Johnsen SP, Overgaard S, Søballe K, Sørensen HT, Lucht U. Total hip arthroplasty in Denmark: incidence of primary operations and revisions during 1996–2002 and estimated future demands. Acta Orthop 2005; 76: 182–9.
- Piriou P, Culpan P, Mullins M, Cardon JN, Pozzi D, Judet T. Ankle replacement versus arthrodesis: a comparative gait analysis study. Foot Ankle Int 2008; 29 (1): 3-9.
- Rydholm U. Is total replacement of the ankle an option? Acta Orthop 2007; 78 (5): 567-8.
- Sokka T, Kautiainen H, Hannonen P. Stable occurrence of knee and hip total joint replacement in Central Finland between 1986 and 2003: an indication of improved long-term outcomes of rheumatoid arthritis. Ann Rheum Dis 2007; 66: 341–4.
- Skyttä ET, Koivu H, Eskelinen A, Ikävalko M, Paavolainen P, Remes V. Total ankle replacement: a population-based study of 515 cases from the Finnish Arthroplasty Register. Acta Orthop 2010; 81 (1): 114-8.
- The drug registers of the Social Insurance Institution of Finland (SII), (Drug Prescription Register and Drug Reimbursement Register).
- Valderrabano V, Hintermann B, Nigg BM, Stefanyshyn D, Stergiou P. Kinematic changes after fusion and total replacement of the ankle: Part 1: Range of motion. Part 2: Movement transfer. Part 3: Talar movement. Foot Ankle Int 2003; 24 (12): 881-900.
- Ward MM. Decreases in rates of hospitalizations for manifestations of severe rheumatoid arthritis. 1983–2001. Arthritis Rheum 2004; 50: 1122–31.
- Weiss RJ, Stark A, Wick MC, Ehlin A, Palmblad K, Wretenberg P. Orthopaedic surgery of the lower limbs in 49802 rheumatoid arthritis patients: results from the Swedish National Inpatient Registry during 1987 to 2001. Ann Rheum Dis 2006; 65 (3): 335–41.
- Weiss RJ, Ehlin A, Montgomery SM, Wick MC, Stark A, Wretenberg P. Decrease of RA-related orthopaedic surgery of the upper limbs between 1998 and 2004: data from 54579 Swedish RA inpatients. Rheumatology 2008; 47 (4): 491–4.