Abstract
“The beginning of knowledge is the discovery of something we do not understand.” – Frank Herbert
ATYPICAL FRACTURES
Bisphosphonate use is associated with the occurrence of stress fractures in the femoral diaphysis, also referred to as atypical femoral fractures. We now know that the risk increases with prolonged use, is not closely related to other drugs, and decreases rapidly after treatment cessation. A stringent radiographic definition of cases is essential for adequate risk calculations. Erroneous classifications in some studies can, at least partially, explain previous large discrepancies in risk estimations among different studies.
The histological analysis of the fracture site itself shows a thin fracture line running perpendicular to the long axis of the femur. Despite ongoing remodeling in the bone adjacent to the fracture gap, no healing occurs within the gap itself. Necrotic material in the gap suggests that strains within the gap might prohibit ingrowth of cells necessary for healing. This mechanism of inhibited healing might share similarities with that of stress fractures in athletes. Although it is highly likely that bisphosphonates play a causative role, the pathogenesis of these fractures is still unclear. It may involve a reduced capacity for targeted remodeling.
Background
Bone remodeling
Bone resorption and replacement with new bone, also referred to as remodeling, is a natural process regulated by complex hormonal systems to achieve three major functions. First, it provides a mechanism for the skeleton to adapt to its mechanical environment. Second, it helps to maintain homeostasis of essential minerals by regulating serum concentrations. Third, it constitutes a mechanism to repair the damage created in bone by daily loading. Site specific remodeling initiated by microdamage is also called targeted remodeling and is distinguished from a more random form of remodeling referred to as stochastic remodeling.
Microdamage are small cracks in bone (microcracks) or diffusely damaged areas (diffuse microdamage) that occur physiologically as a consequence of repeated cycles of loading during activities of daily living. Microdamage accumulates over time and the overall burden of microdamage is kept under control by remodeling targeted towards damaged areas. The progression of microcracks is deflected by morphological features of bone. The heterogeneous lamellar structure of osteons and the alternation of interstitial and osteonal lamellae are examples of such morphological barriers. If microcracks grow, the osteocyte-canalicular network gets disrupted and causes apoptosis of nearby osteocytes (Frost Citation1998, Cardoso et al. Citation2009). As a result, osteocytes secrete receptor activator of nuclear factor kappa B ligand (RANKL) and trigger the formation of osteoclasts that resorb the damaged area. Targeted remodeling starts and the damaged area is replaced with new bone. The mechanism behind the localization of remodeling sites in stochastic remodeling is less clear.
Osteoporosis
In osteoporosis, the coupling mechanism between osteoclasts and osteoblasts is defect. Normally, osteoclasts require weeks to resorb bone, whereas osteoblasts need months to produce the same amount of new bone to fill the resorption cavity. In osteoporotic bone, osteoclasts resorb bone efficiently but osteoblasts are incapable of refilling the cavity completely. Therefore, an increase in bone remodeling results in net bone loss over time. Increased resorption also deteriorates the microarchitecture of the bone. Trabeculae decrease in number and size and change their shape from stronger, plate-like formations to weaker rods. In remodeling, the new bone is formed on an old bone surface. If a surface is lost because a trabecular plate is perforated by a resorption pit, no new bone can form at all.
In periods of rapid remodeling (e.g. after menopause), a larger proportion of the bone is new and immature. This leads to a higher risk of fracture, because the new bone is less densely mineralized, and the isomerization and maturation of collagen are incomplete. Moreover, the resorption sites are temporarily unfilled.
Age and loss of gonadal function are the two main factors in the development of osteoporosis. Decreases in estrogen levels result in higher numbers of preosteoclasts and an increased lifespan, vigor and activity of mature osteoclasts. With higher age the number of osteoblasts decreases, which creates a negative balance between resorption and formation of bone. Men are less affected by osteoporosis and lose only 15–20% of their cortical bone and 25–30% of trabecular bone, whereas women lose 30–40% of their cortical bone and 50% of their trabecular bone over their lifetime.
It seems obvious that interventions leading to an increase in bone mass should reduce the risk of osteoporosis related fractures. With Dual Energy X-ray Absorptiometry (DXA) measured at the hip, hip fracture risk increases approximately 2.6-fold per SD decrease in bone mineral density (BMD), and the risk of any fracture increases 1.6-fold per SD (Marshall et al. Citation1996). However, the equation is not that simple when treatment efficacy of anti-osteoporosis drugs is calculated. The correlation between higher BMD and decreased hip fracture risk is strong for younger patients but decreases with age (Johnell et al. Citation2005). This discrepancy can be explained by extra-skeletal risk factors affecting the risk of falls, but also by age related changes in trabecular architecture, remodeling and accumulation of microdamage.
Bisphosphonates
The most commonly used drugs in the prevention and treatment of osteoporosis are bisphosphonates. Chemically they are similar to pyrophosphates, and were derived from molecules originally designed to inhibit calcification. The initial treatment intention was the prevention of calcification of blood vessels in atherosclerosis, the formation of kidney stones and plaque in dental care. Empirically, their effect on bone resorption was discovered, and molecules with high affinity to hydroxyapatite crystals were subsequently developed, of which the most widely used is alendronic acid. After administration, either orally or intravenously, bisphosphonates bind to bone selectively. They remain within the bone with a half-life of about 10 years. Sites with ongoing bone resorption have a higher affinity because the osteoclasts have removed the protein layer that normally covers the mineral. The osteoclast is therefore exposed to very high concentrations of bisphosphonate during resorption of mineral bound with bisphosphonate.
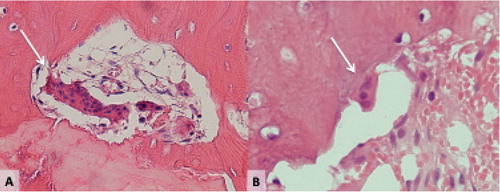
Alendronate, ibandronate, risedronate, and zoledronate are the bisphosphonates most commonly used and belong to the group of nitrogen containing bisphosphonates. They act on the osteoclast by inhibiting several enzymes within the mevalonate biosynthetic pathway. By inhibiting this pathway, multiple cell processes important for osteoclast function are affected, such as cytoskeletal arrangement, membrane ruffling, trafficking of vesicles and apoptosis. The inhibition of these cellular processes lead to increased numbers of inactive osteoclasts. About one third of osteoclasts show detachment from the underlying bone and an increased number of nuclei, which are pyknotic (). These cells are referred to as giant osteoclasts (Weinstein et al. Citation2009).
Figure 1. Different osteoclasts. A: Giant osteoclast, detached from the bone, in a resorption cavity close to the fracture line of an atypical femoral fracture. B: Normal osteoclast in a healthy individual with tibial stress fracture.
In addition, experimental studies suggest that bisphosphonates might mediate osteoclast activity through effects on osteoblasts (Sahni et al. Citation1993). The inhibition of RANK-ligand expression and an increase of osteoprotegerin expression in the osteoblast could be possible mechanisms (Mackie et al. Citation2001, Viereck et al. Citation2002). However these hypotheses are based on in vitro studies of cell cultures and it remains unclear if this effect is relevant in vivo. One study investigated the effect of bisphosphonates on osteocyte apoptosis induced by microcracks, and found a decrease in the amount of apoptotic osteocytes with bisphosphonate treatment (Follet et al. Citation2007). In another experiment exposing osteoclasts and osteoblasts to a bisphosphonate bound to a calcium loaded surface, osteoclast activity diminished while osteoblasts were largely unaffected (Schindeler and Little Citation2005). Thus the evidence is contradictory and does not allow definite conclusions.
Inhibition of resorptive activity in osteoporotic bone will break the vicious circle of increased bone resorption and insufficient bone formation. An increase in BMD can be noted. This increase differs among individuals and anatomic location. Hip BMD, measured with DXA, typically raises by 3-5% during the first 2 years of treatment. Thereafter only minimal changes can be measured (Bone et al. Citation2000). In vertebral bodies the effect is stronger, and BMD typically increases with 8-10% and continues to rise also after 5 years of treatment (Cummings Citation1998, Bone et al. Citation2004, Mellstrom et al. Citation2004). Interestingly an increase in vertebral body BMD can be noted over time also in placebo-treated groups. This change however is lower than in the treated groups and might be caused by calcifications due to degenerative changes of the spine (Yu et al. Citation1995, Bone et al. Citation2004). Higher BMD is correlated with a decrease in the risk of fracture after 3–5 years of treatment. However, only a small proportion of this risk reduction can be explained by changes in BMD (Delmas and Seeman Citation2004).
The efficacy in the reduction of relative fracture risk in some clinical trials has been reported as high as 50% for vertebral and non-vertebral fractures after 3–5 years of treatment (Black et al. Citation2000, Citation2007). After this initial treatment duration no placebo-controlled trial has been able to show a further decrease in the risk of hip fracture. There are a few prospective trials investigating treatment efficacy of continuation after some years of treatment (Black et al. Citation2006, Citation2012). These are extensions of pivotal trials where one group received placebo after 3 or 5 years of treatment and the other continued treatment. Primary outcomes were changes in BMD but not in fracture risk. One study found no difference in the risk of hip fractures with extended treatment and the other found a beneficial effect of extended treatment only in a post-hoc analysis of a highly selected subgroup of individuals with hip fractures.
In a matched case-control analysis from the Netherlands no reduction in fracture risk could be found after more than 5 years of treatment. The investigators found a 12% reduction in fracture risk after 1–2 years of compliant use and 46% after 3–4 years of use. Unexpectedly, after 5–6 years of treatment with different bisphosphonates the reduction in fracture risk had decreased to levels similar to that with < 1 year of use (Meijer et al. Citation2008).
Improvements in BMD are achieved by a reduction of remodeling. However, remodeling as a repair mechanism – targeted remodeling – is still needed for maintenance of the skeleton. The improvement of BMD therefore might be at the cost of deterioration in the ability to deal with local bone microdamage.
Potential side effects on bone quality
Turnover in trabecular bone, measured with tetracycline double label or as the activation frequency, can decrease with up to 90% in patients treated with bisphosphonates compared to untreated patients (Chavassieux et al. Citation1997, Bone et al. Citation2000). The reduction in turnover in cortical bone is somewhat lower, estimated to 60% (Mashiba et al. Citation2000). Measurements of markers of bone turnover show a similar decrease (Bieglmayer et al. Citation2012). In preclinical models, effects on bone turnover were highly site-specific, with differences by an order of magnitude between different bone sites (Smith et al. Citation2003, Allen et al. Citation2009). Both stochastic remodeling and targeted remodeling are affected by the antiresorptive effect of the bisphosphonate (Li et al. Citation2001). Stochastic remodeling is estimated to contribute approximately 70%, and targeted remodeling about 30% to overall bone turnover (Burr Citation2002). Bisphosphonates are attracted to metabolically active bone sites and therefore appear to preferentially suppress the targeted repair process (Li et al. Citation2001).
Inhibition of remodeling, therefore, can change the mechanical properties of bone in different ways. First, by inhibition of stochastic remodeling, the composition of the bone mineral and its matrix can be altered. Second, through an inhibition of targeted remodeling, microcracks can accumulate. Each mechanism by itself or in combination with the other can cause deteriorations in the mechanical properties of bone.
Early reports on atypical femoral fractures
The first clinical report of a potential negative effect of bisphosphonate use on patients with osteoporosis came in 2005 (Odvina et al. Citation2005). Patients on long-term bisphosphonate treatment were reported to have suffered femoral shaft fractures during activities such as standing, walking or turning around. Some patients had bilateral femoral shaft fractures. The authors related these fractures to severely suppressed bone turnover (SSBT) caused by bisphosphonate treatment, and defined this condition histologically by reduced osteoblastic and osteoclastic surfaces with decreased or absent tetracycline labeling in iliac crest biopsies.
This report triggered intensive research on femoral shaft fractures and its potential association with bisphosphonate treatment. The distinctive radiographic pattern of these fractures, resembling features of stress fractures, made them easy to identify among other more common fractures of the femur ().
Figure 2. Bisphosphonate-associated shaft fractures show radiographic signs of stress fractures. Note the fracture line running perpendicular to the long axis of the femur and its origin at the tensional side of the bone. Black arrow: endosteal callus reaction. Horizontal white arrow: periosteal callus reaction. Oblique white arrow: medial spike.

Goh et al. (Citation2007) described a series of 13 patients with subtrochanteric femur fractures caused by low energy trauma. Nine patients were on alendronate therapy and showed a transverse fracture pattern on the tensional side of the femoral shaft, with focal cortical thickening and prodromal pain in the affected thigh for weeks before the fracture occurred. Three of 9 patients had bilateral lesions. In 2008, also Neviaser et al. (Citation2008) reported a strong association between the specific fracture pattern and alendronate use, in a series of diaphyseal femur fractures. None of these studies were able to calculate the relative or absolute risk of atypical femoral fractures in the population.
With access to local hospital registries and digitized radiographs, as well as a national drug registry, we saw the possibility to assess the absolute risk for femoral stress fractures among bisphosphonate users and non-users in two Swedish health care districts. In a population-based study (Schilcher and Aspenberg Citation2009) we were able to show that patients treated with bisphosphonates had a 46 times higher risk to suffer a femoral insufficiency fracture compared to non-users. The absolute risk after 5 years of treatment was 1/1000 for bisphosphonate users. We were not able to adjust for comorbidities and drug use and the sample was too small to correct for age differences.
Meanwhile, further case series were published and the term “atypical femoral fractures” was forged by a publication in The New England Journal of Medicine by Lenart et al. (Citation2008).
The pendulum swings
After these initial reports, an association between atypical femoral fractures and bisphosphonate use seemed plausible. Some researchers involved in osteoporotic research, however, appeared to oppose this view.
Epidemiologists in Denmark used the Danish National Hospital Discharge Registry and National Prescription Database to search for an association between bisphosphonate treatment and atypical fractures (Abrahamsen et al. Citation2009). In their report the term atypical femoral fracture and subtrochanteric or diaphyseal femoral fracture were used synonymously. Fractures were identified by diagnosis codes and no x-rays were reviewed to identify the specific fracture pattern. The authors detected no difference in alendronate exposure between patients with femoral neck or intertrochanteric fractures and subtrochanteric or shaft fractures. Both fracture types were reduced with high adherence to bisphosphonate treatment. They concluded: “subtrochanteric/diaphyseal femur fractures share the epidemiology and treatment response of classical hip fractures and are best classified as osteoporotic fractures”.
In 2010, Black et al. reported that the risk of fracture of the subtrochanteric or diaphyseal femur was not increased with bisphosphonate use. They reviewed patient records of 284 patients with fractures of the femur that had occurred among 14,195 women included in three large randomized clinical trials of bisphosphonates, the Fracture Intervention Trial (Black et al. Citation2000) and its long-term extension (Black et al. Citation2006), and the HORIZON trial (Black et al. Citation2012). Radiographs from one patient were available for review by the investigators. For the remaining cases, only radiographic reports from community radiologists were available. When those radiographic reports were written, radiologists were unaware of the specific fracture pattern and therefore it is unlikely that features of atypical fractures would have been reported even if they were present. Because of the rarity of these fractures and the relatively small sample size, the statistical power was extremely low, reflected in wide confidence intervals. Also, only a minority of patients received more than 4 years of bisphosphonate, and some received a lower dose of alendronate than commonly prescribed. Despite these limitations the report gained much attention.
One case series reported on a high prevalence of glucocorticoid use among atypical fracture patients (34%) and identified this as an additional risk factor (Girgis et al. Citation2010). Several case reports established an association with other antiresorptive drugs in addition to bisphosphonates (estrogen, raloxifene, calcitonin) (Schneider Citation2006, Demiralp et al. Citation2007, Somford et al. Citation2009).
Also a high incidence of proton-pump-inhibitor use (PPI) was identified in a large proportion (39%) of atypical femoral fracture patients in some case series. The authors speculated that PPIs could constitute an additional important risk factor (Ing-Lorenzini et al. Citation2009, Giusti et al. Citation2010).
Contradiction leading to Paper I
The contradictory results from case series and registry-based analyses or randomized trials were difficult to understand. The confusion increased even further when speculations on other drugs as additional risk factors appeared. The question arose whether the case series were biased or the registry studies and randomized studies did not identify atypical fractures accurately. Our population-based study from 2009 (Schilcher and Aspenberg Citation2009) gained little attention, perhaps due to a small number of cases, but also some methodological weaknesses. We therefore decided to perform a stringent epidemiological investigation among all women in Sweden.
Epidemiology of atypical femoral fractures (Paper I)
Aims
Our primary aim was to find out whether an association between atypical femoral fractures and bisphosphonate use can be shown, when a large registry database is combined with radiographic adjudication of fracture types.
Methods and results
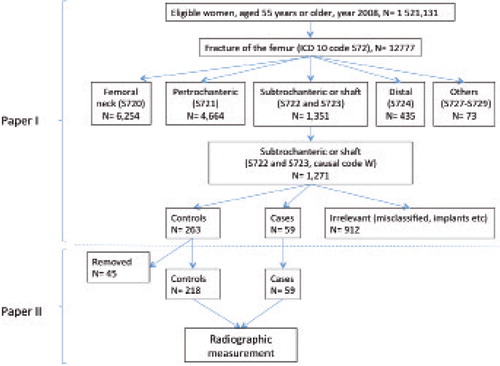
In Sweden, 12,777 women 55 years of age or older sustained a fracture of the femur in 2008. We reviewed radiographs of 1234 of the 1271 women who had subtrochanteric or shaft fractures and identified 59 patients with atypical fractures (). Atypical femoral fractures were identified according to commonly used radiographic signs of stress fractures (transverse fracture line originating from the tensional side of the femur, and callus reaction). Fractures associated with pre-existing implants, and pathologic fractures were excluded.
Figure 3. Upper part: Identification of atypical fractures in Paper I. Lower part: Further selection of cases and controls for Paper II.
Data on medications and coexisting conditions were obtained from national registries. The relative and absolute risk of atypical fractures associated with bisphosphonate use was estimated by means of a nationwide cohort analysis. To minimize bias, we compared baseline characteristics between 59 patients with atypical fracture and 263 control patients in a case-control analysis. The control group comprised patients with ordinary subtrochanteric or shaft fractures and was chosen in order to represent patients with a similar risk profile of skeletal fragility as patients with atypical fracture.
The age-adjusted relative risk of atypical fracture was 47 (95% confidence interval [CI], 26 to 87) in the cohort analysis (). The increase in absolute risk was 5 cases per 10,000 patient-years (95% CI, 4 to 7). A total of 78% of the case patients and 10% of the controls had received bisphosphonates, corresponding to a multivariable-adjusted odds ratio (OR) of 33 (95% CI, 14 to 78) (). The risk was independent of co-existing conditions and of concurrent use of other drugs with known effects on bone. Patients with atypical femoral fractures were slightly younger and appeared healthier than controls. They used antidepressants less frequently than control patients but there was no difference in the use of corticosteroids or PPIs. The duration of use influenced the risk (OR per 100 daily doses, 1.3; 95% CI, 1.1 to 1.6). After drug withdrawal, the risk diminished by 70% per year since the last use (OR, 0.28; 95% CI, 0.21 to 0.38).
Table 1. Age-adjusted relative risk (RR) and absolute risk (AR), with 95% confidence intervals (95% CI), of atypical femoral fracture associated with the use of bisphosphonate during the 3 years (2005–2008) preceding the fracture
Table 2. Odds ratios (OR), with 95% confidence intervals (95% CI), for atypical femoral fractures associated with bisphosphonate use
Conclusion and discussion
The data of Paper I show a strong association between bisphosphonate use and atypical fractures. The absolute risk is low and atypical fractures also occur in patients without reported bisphosphonate use. With a correct indication, the benefits of fracture prevention with bisphosphonate use will outweigh the risk of atypical femoral fracture.
The risk of atypical fractures decreased more rapidly after drug withdrawal than would be expected, given the prolonged presence of the drug in the bone. This observation and the increased risk already during the first years of treatment are difficult to reconcile with the etiologic hypothesis that these fractures are a consequence of increased age of the cortical bone because of reduced remodeling. Thus, the pathogenic role of bisphosphonates probably involves faster processes.
New literature challenging Paper I
In 2010, the American Society for Bone and Mineral Research (ASBMR) published a classification system defining major and minor features of atypical femur fractures in order to provide unified criteria for both clinicians and researchers () (Shane et al. Citation2010). For a correct case definition, all major criteria needed to be satisfied but none of the minor was compulsory.
Table 3. ASBMR Task force criteria for atypical femoral fractures from the first report in 2010 (left column) and revised after the second report in 2013 (right column). Bold font according to ASBMR´s original
All of these criteria were typical for stress fractures, except for the generalized cortical thickening among the minor criteria. However, the ASBMR criteria were not precisely defined, and typical features of stress fractures can be found both among the major and minor categories. The major criterion of a transverse fracture line is a hallmark feature of material fatigue. However, the ASBMR provided a very wide definition of fracture angle. Besides the transverse fracture angle also short oblique fractures were included. Short oblique is usually defined as a fracture angle between 45–135 degrees (Dencker Citation1963), which is not indicative of material fatigue.
If also patients without the typical stress fracture pattern become included in cohort studies or case-control studies, the strength of the association with bisphosphonate use is likely to be reduced.
In a large cohort study, Feldstein et al. (Citation2012) calculated an odds ratio of 2 for patients on bisphosphonate treatment to suffer an atypical fracture, compared to non-users. They studied the incidence of femur fractures in a large health care provider cohort in women and men between 1996 and 2009. During the observation period 5034 fractures occurred and from these 864 radiographs were reviewed. Atypical fractures were categorized as those with ASBMR major criteria or those with major criteria and at least one of the ASBMR minor criteria. Out of all 197 subtrochanteric or shaft fractures, 75 patients (38%) met the major criteria. Of these, 22 also met at least one minor criterion. Bisphosphonates were used during the year before the fracture of 24% of the patients with only major criteria (compared to 78 % in Paper I). The resulting odds ratio of 2 for patients on bisphosphonate treatment to suffer an atypical femoral fractures is contradictory to our finding of an odds ratio of 33 in Paper I. The work by Feldstein was published in the Journal of Bone and Mineral Research (JBMR) along with a commentary by Abrahamsen (Citation2012). In this commentary, the Feldstein study was compared with our study (Paper I) discussing strengths of the one study and limitations of the other.
Contradiction leading to Paper II
To restore balance between the Feldstein study and our study (Paper I), we wrote a letter to the editor of the JBMR pointing out some important limitations of the Feldstein study that we found necessary to emphasize in order to empower the reader to interpret the results adequately. Feldstein et al. (Citation2012) had chosen a wide range of fracture angles to identify atypical fractures. With too wide definitions of an atypical fracture they would disappear in the noise of other fractures. Our letter was rejected without motivation, but was later published along with an editorial in Acta Orthopaedica (Rydholm Citation2012).
In order to find explanations for the conflicting results in different studies, we found it necessary to investigate the radiographic characteristics of atypical femoral fractures in detail.
Radiographic features (Paper II)
Aims
The primary aim was to investigate whether atypical femoral fractures constitute a well-delineated separate entity, defined by the angle of the fracture line, or if they represent one end of a continuum of osteoporotic fracture appearances. If they constitute a separate entity, they should be easily identified by specific radiographic features typical for stress fractures: a transverse fracture line and callus reaction. Therefore we aimed to evaluate the specificity and sensitivity of various radiographic features to detect bisphosphonate treatment.
We also hypothesized that if a feature with a lower specificity is chosen, such as a fracture angle between 60° and 120°, instead of a transverse pattern, the number of atypical fractures will be overestimated and the relation to bisphosphonate use attenuated. To test this we aimed to evaluate differences in atypical fracture incidence when applying radiographic ASBMR criteria instead of the traditional orthopedic criteria for stress fractures that were used in our study (Paper I).
Methods and results
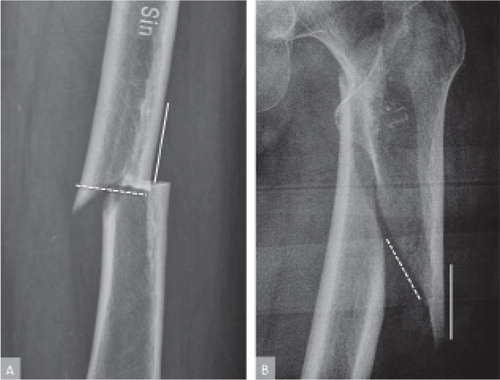
In Paper I we diagnosed 59 atypical and 263 control fractures of the femoral shaft. In Paper II we excluded 45 control patients who either had implants that were not initially detected or fracture extensions into the trochanteric region (). The atypical fractures were defined by their stress-type fracture pattern (Schilcher et al. Citation2011). All fractures were now reassessed by a physician in training, who was blinded to drug treatment and previous classifications. The fracture angle (0–180°) was measured (). Presence of focal lateral cortical thickening (a callus reaction), more than 2 fragments, or a medial spike was noted (). All fractures were then reclassified according to the ASBMR criteria.
Figure 4. Measurement of fracture angle. A: atypical femoral fracture with a fracture angle close to 90 degrees measured on the proximal shaft fragment. B: fracture with an angle of about 30 degrees.
Frequency distribution analysis of the fracture angle showed a distinct subgroup, comprising roughly 25% of all fractures, with a mean of 89 degrees and SD of 10 (). 42 of 57 patients with a fracture angle between 75 and 105 degrees used bisphosphonates, whereas only 27 of the 213 others did. The presence of a callus reaction had a specificity for bisphosphonate use of 96% (). The ASBMR criteria had a lower specificity, increasing the number of atypical fractures without bisphosphonate use from 13 to 31. This led to a decrease in age-adjusted relative risk associated with bisphosphonate use from 47 to 19.
Figure 5. Frequency distribution of fracture angles. Fracture angles occurred in three different peaks. The peak in the middle represents a distinct subpopulation with fracture lines running close to perpendicular to the lateral cortex of the femoral shaft, i.e. 89 degrees, SD 10.
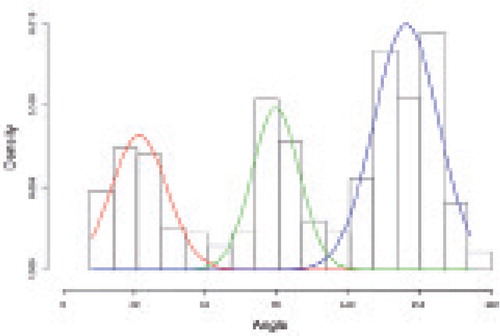
Table 4. Specificity and sensitivity of radiographic features to detect bisphosphonate treatment with 95% Confidence Intervals (CI)
Conclusion and discussion
Atypical fractures of the femoral shaft are a specific entity and radiographic features of stress fractures are strongly related to bisphosphonate use. The re-analysis of our own material according to ASBMR criteria decreased the relative risk by about half.
Still, a large part of the risk difference from e.g. Feldsteins study remains unexplained. The difference might be explained by the fact that Feldstein et al. chose to extend the criterion of fracture angle even further than the already wide range according to the ASBMR criteria. More than half of their diaphyseal fractures were classified as atypical and measured a fracture angle between 30 and 150 degrees. Three fractures deviated even further. The intention behind these wide inclusion criteria is unclear but might explain the very low association between atypical femoral fractures and bisphosphonate treatment in that study.
In 2013 the ASBMR revised their criteria. In their new report, the authors emphasize the importance of a transverse fracture line for a correct case definition, and the feature of focal cortical thickening at the level of the fracture line was added to the major criteria (). The criterion of generalized cortical thickening remained among the minor criteria and we have discussed it elsewhere (Koeppen et al. Citation2012).
Theories on pathogenesis
Stress fractures can be divided into fatigue fractures and insufficiency fractures. Fatigue fractures typically occur in athletes and military recruits due to excessive loading. Insufficiency fractures occur in conditions of normal loading where the problem lies within the bone. Some examples are osteopetrosis, Pagets disease, osteogenesis imperfecta, hypophosphatasia, and adynamic bone disease. Atypical femoral fractures most likely belong to the category of insufficiency fractures.
Regardless the underlying mechanism, incomplete stress fractures have a number of common characteristics such as a fracture line running perpendicular to the long axis of the bone, slow progression with attempts to heal (callus formation), pain at the fracture site and a high risk for delayed healing or non-union. Ultimately, fracture progression and insufficient healing can lead to displacement of the fracture.
In athletes, 2 theories on the pathogenesis of stress fractures exist (Bennell et al. Citation1996). The primary microdamage hypothesis describes the initiation of the fracture where microdamage accumulates due to high local stresses and where damage exceeds repair. In the primary remodeling hypothesis, accelerated bone remodeling due to various local or systemic factors is the initiating stimulus for the development of the fracture. Excessive bone remodeling, which precedes bone formation, can lead to focal weakening of the bone, microdamage can accumulate and a fracture develop. Most likely these two mechanisms interact with each other, and continuous loading in both cases can result in a symptomatic stress fracture.
The mechanism that causes the formation of a stress fracture in aged women on bisphosphonate treatment is not that well understood but some theories have been postulated in recent years.
Changes in bone matrix composition
Bone is heterogeneous due to its constant remodeling and the different rates at which mineralization occurs. This heterogeneity is reflected by a varying distribution of bone mineral density, mineral crystal composition, and collagen maturity (cross-linking). A heterogeneous distribution of tissue composition appears to be advantageous in terms of mechanical properties compared to a homogenous composition. In a computational model, heterogeneous distribution reduced local stress and enhanced energy dissipation, whereas a homogeneous distribution was associated with greater propensity for crack formation and propagation (Tai et al. Citation2007, Renders et al. Citation2011).
Healthy individuals show a remarkably small biological variation in bone composition suggesting the existence of an evolutionary optimum with respect to its biomechanical performance.
Both mineralization and collagen maturity substantially add strength to developing bone. However, a too high mineral content is known to make bones brittle, while a too low mineral content makes them soft (Fratzl et al. Citation2007).
The material properties can now be measured due to advances in Fourier transformed imaging (FTIR). This technology has made it possible to measure bone material properties and relate these indirectly to changes in mechanical properties (Miller et al. Citation2007) and fracture risk (Gourion-Arsiquaud et al. Citation2009).
Bisphosphonates are believed to increase the age of the bone within an individual, since older lamellae are less frequently resorbed and fewer bone metabolic units form less new bone. With time, the lamellae retain more hydroxyapatite crystallites, the crystallites mature and the structure of the bone becomes more homogeneous (Mashiba et al. Citation2005, Boskey et al. Citation2008, Donnelly et al. Citation2012). Fully mineralized osteons allow a faster progression of microcracks that occur during physiological loading. Physiological barriers of crack progression, such as cement lines and lamellar structures in the osteons are weakened by a higher degree of homogeneity. Also highly mineralized collagen might become more brittle and thus more susceptible to microdamage (Ettinger et al. Citation2013).
Accumulation of advanced glycation end products (AGEs) in the bone matrix due to long-term bisphosphonate treatment could be another pathophysiological mechanism. An increase in AGEs has been associated with a decrease in post-yield work-to-fracture, maybe due to an increase in brittleness of the bone matrix (Vashishth et al. Citation2001, Tang et al. Citation2009). AGEs have also been associated with a reduction in osteoclast-derived bone resorption with subsequent deteriorations in the structural integrity of bone matrix protein (Valcourt et al. Citation2007).
Microcrack accumulation
Microdamage in bone, diffuse microdamage and microcracks, is physiological and occurs in both trabecular and cortical bone in a similar way as in other composite materials. The first level at which microdamage might form is the debonding of the collagen fiber from the matrix, the disruption of the mineral-collagen composite or the disruption of the collagen fiber itself (Burr et al. Citation1996). These small damaged areas can grow and coalesce with neighboring damaged areas to form a fine crack. Such a crack can grow and propagate until it reaches a canaliculus containing the cytoplasmatic process of an osteocyte. The disruption of the cytoplasmatic process initiates apoptosis of the osteocyte and the secretion of cytokines such as RANKL. This will initiate the process of targeted remodeling, and the damaged area becomes resorbed and replaced with new bone. In healthy individuals, microdamage accumulation is kept in balance by remodeling, but with age and female gender the burden of microdamage increases (Norman and Wang Citation1997). Also the size and amount of cracks differ between younger and older individuals (Diab et al. Citation2006). While the bone from older persons tends to form long linear microcracks, that of younger individuals tends to form smaller cracks in localized areas. These differences might explain the higher tolerance to fatigue loading in bone from younger compared to older individuals (Diab et al. Citation2006).
Microcracks seem important for bone health, providing the bone with plasticity. As long as their progression is inhibited by natural barriers, microcracks can inhibit growth of larger macrocracks by functioning as energy absorbers dissipating energy from the tip of a large crack (Vashishth et al. Citation1997).
With the application of an antiresorptive with documented effects on both stochastic and targeted remodeling (Li et al. Citation2001), the equilibrium of microdamage formation and repair can be brought out of balance. Damage can then accumulate to levels that are significantly higher than in healthy, untreated individuals. These theories of microdamage accumulation are mainly based on animal studies. In beagle dogs treated with bisphosphonates at 6 times the clinically recommended doses, microdamage accumulation was noted in both cortical and trabecular bone (Mashiba et al. Citation2001). In the lumbar vertebrae, microdamage increased 2-4 fold compared to a 4-7 fold increase in the rib. Similar results were shown with doses of bisphosphonates recommended in the treatment of osteoporosis (Allen et al. Citation2006). In monkeys treated with different bisphosphonates, microcrack density in vertebral bodies was higher compared to untreated controls, but there was no statistically significant difference in crack morphology or density in the femoral cortex (Yamagami et al. Citation2013).
There seems to be an association between bisphosphonate treatment and accumulation of microdamage, but it remains unclear whether changes in bone mechanical properties are related to microdamage or rather to changes in BMD and architecture. Even in untreated animals it is not clear whether increased microdamage leads to deteriorations in mechanical properties. Some groups could find indications of an association (Burr et al. Citation1998), while others could not (Follet et al. Citation2010).
At the moment there is no consistent evidence that bisphosphonate treatment increases the burden of microdamage in bone in humans (Allen and Burr Citation2011).
Even if microdamage does not affect mechanical properties of bone that are measureable with conventional testing, a microcrack unhindered in its progression could grow quickly and lead to the formation of a macrocrack and ultimately a stress fracture.
Mechanical properties of bone
Mechanical properties of bone can be divided into structural properties and material properties. Structural properties, such as ultimate load, stiffness, and work to failure are measured at the level of the whole bone and are dependent on bone mass, architecture, and the material properties of the tissue. Material properties are determined by components of the mineral such as degree of mineralization and its heterogeneity and the organic matrix, such as the content of collagen and its maturity. Bisphosphonates alter material properties of bone as well as microarchitecture and therefore might have an effect on both properties.
Several animal studies have shown that bisphosphonate treatment is associated with a decrease in tissue toughness when material properties are normalized for the increase in bone mass (Mashiba et al. Citation2000, Citation2001, Komatsubara et al. Citation2003, Allen et al. Citation2006).
Bala et al. (Citation2011) investigated transiliac bone biopsies from women on long term bisphosphonate treatment, and found that alendronate treatment was associated with a 84% lower remodeling activity compared to untreated women. Treated patients showed an increase in the degree of mineralization in both cortical and trabecular bone but microhardness was lower than that measured in untreated patients. In a study using a nanoindentation technique in transiliac bone biopsies, bisphosphonate treated patients showed a greater resistance to plastic deformation and harder trabecular bone than controls (Tjhia et al. Citation2011). An in-vivo measurement using nanoindentation at the tibia showed deteriorations of bone material properties in patients with atypical femoral fractures compared to untreated controls without fractures. However, a control group consisting of patients with typical osteoporotic fractures showed similar deteriorations (Güerri-Fernández et al. Citation2013).
Most studies investigated transiliac bone biopsies, a location rarely affected by fracture and sample sizes were often small. Also, bone composition seems to vary across anatomic sites (Donnelly et al. Citation2011) and there is evidence that femoral cortical bone behaves differently both in the respect of microdamage accumulation, and changes in bone mineral and matrix properties compared to sites with predominantly trabecular bone (Yamagami et al. Citation2013). Thus the information on bisphosphonate induced changes in biomechanical properties seems insufficient to draw any final conclusions on the pathogenesis of atypical fractures.
Discussions leading to Paper III
Changes in bone material properties might explain why atypical femoral fractures occur in association with bisphosphonate treatment. However, once the fracture is established and has penetrated the lateral femoral cortex and its periosteum, osteoblast derived callus formation is initiated, a mechanism unaffected by bisphosphonate treatment. Nevertheless the fractures do not heal and frequently progress to become displaced.
The lateral periosteal bump at the level of a clearly visible fracture line constitutes an established radiographic feature of atypical femoral fractures and stress fractures alike. Even if the pathophysiological mechanisms behind the development of these fractures differ, the reason for delayed fracture healing and non-union might be similar and not related to bisphosphonate treatment alone. Further information about the pathophysiology might be found at the fracture site itself.
Histology of the fracture site (Paper III)
Aims
We have previously described the histological picture of a bisphosphonate-associated atypical femoral fracture and found indicators suggesting impaired healing of the crack, in spite of increased remodeling of the adjacent bone (Aspenberg et al. Citation2010). The current study aimed to verify those early findings and to find new clues that might help us to explain the pathogenesis of atypical fractures at the microscopic level.
Methods and results
Between 2008 and 2013, bone biopsies comprising the fracture site were collected from 4 complete and 4 incomplete atypical femoral fractures (). The biopsies were taken during surgical fixation of the fracture (). Seven female patients reported continuous bisphosphonate use for an average of 10 years. One patient was a man, not using bisphosphonates. The bone biopsies were evaluated histologically, with Fourier transformed infrared imaging (FTIR) and micro-computed tomography.
Figure 6. A: Fracture line in the operating field surrounded by callus formation seen as a slight elevation of the surface. B: Bone biopsy including the fracture line.
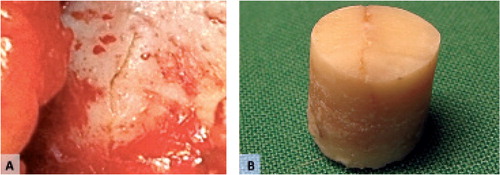
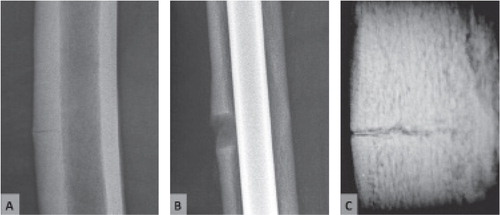
Figure 7. Incomplete fracture. A: conventional radiograph. B: Cortical defect after taking a biopsy. C: Microradiography of the bone biopsy. Note the fracture line.
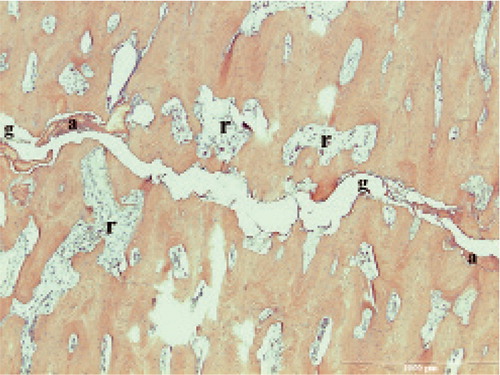
Incomplete fractures engaged the whole cortical thickness and comprised a 150 to 200 µm wide fracture gap filled with amorphous necrotic material. Active resorption and remodeling was common in the close vicinity of the fracture gap, but only rarely reached all the way into the gap ().
Figure 8. Incomplete fracture. g fracture gap, a amorphous material, r resorption cavity.
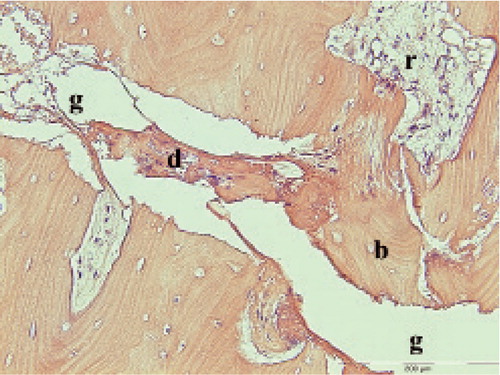
In some areas, the bone adjacent to the gap appeared to undergo fragmentation and disintegration, possibly due to abrasion. Loose bone fragments and cellular remnants could be found in the fracture gap in all cases (). Defects in the fracture surface occurred where fragments had loosened or resorption cavities reached into the fracture. Woven bone was common adjacent to the fracture gap, and appeared to have been formed in such defects.
Figure 9. Incomplete fracture. g fracture gap. b bone fragments about to break off. d cellular remnants. r resorption cavity almost reaching into the fracture gap.
Conclusion and discussion
Atypical femoral fractures appear to consist of a crack, meandering through the lateral femoral cortex with a main direction perpendicular to the long axis of the bone. The crack is thin (200 µm or less) and contains mainly amorphous material, but also traces of bony fragments and cells with different degrees of degradation. The surrounding bone shows signs of remodeling, mainly represented by the presence of osteoclasts, resorption cavities, woven bone and new osteons running parallel to the fracture line. All of these appear mainly in the vicinity of the fracture gap. No signs of remodeling or callus formation could be seen within the fracture gap itself, except for one case where bisphosphonate treatment was ceased 18 months prior to surgery. Especially the change in osteon direction suggests that the area around the fracture gap has been remodeled intensely during months or years, without achieving fracture union.
Judging by histology, it seems that mechanical reasons can explain why these fractures heal poorly, if at all. We found almost no living tissue in the crack. This could be in accordance with the theory of interfragmentary strain and tissue differentiation. Perren (Citation1979) stated that the strain in the fracture influences tissue differentiation and whether a pseudarthrosis develops or not. Because the cracks in our patients were so thin, even a moderate deformation of the entire femur due to loading could be expected to cause strains in the gap that preclude cell survival.
General conclusions
Atypical femoral fractures show a strong association with bisphosphonate use. The absolute risk is low – roughly 5 out of 10,000 patients per year of use. With a correct treatment indication, the benefits of treatment outweigh the risks.
Other drug treatments do not seem to affect the risk of atypical fractures associated with bisphosphonate use.
The risk increases with longer treatment duration and decreases rapidly after cessation.
Middle-aged and older women with atypical femoral fractures appear to be younger and slightly healthier than patients with common, low-energy related fractures of the femur.
There is no continuum between atypical and osteoporotic fracture appearances. The atypical fractures constitute a well-delineated separate fracture entity defined by a transverse fracture angle.
Commonly recognized radiographic features of stress fractures have a high specificity to detect bisphosphonate treatment in fracture patients. The use of wide radiographic inclusion criteria can attenuate risk calculations.
Histologically, atypical femoral fractures show a thin fracture line extending through the whole thickness of the lateral femoral cortex. Periosteal and endosteal callus can be seen, indicating attempts to heal the fracture during weeks or months.
The bone adjacent to the fracture line shows ongoing remodeling, but there are no signs of remodeling within the gap itself.
The fracture gap is filled with necrotic material including cellular remnants and bony structures. This finding and the small size of the fracture gap raise the question whether strains between fracture surfaces induced by daily loading could be made responsible for the inhibition of healing.
Perspective
It is now widely accepted that atypical femoral fractures are associated with bisphosphonate use. The association appears strong, but the absolute risk remains low. Owing to an intense scientific discussion in high impact journals these fractures have become well known by general physicians, endocrinologists, orthopedic surgeons, and the public. Those few patients that will suffer an atypical fracture will have a good chance to be recognized and treated according to current recommendations.
Novel hypothesis on the pathogenesis of atypical femoral fractures
Despite almost a decade of research, little is known about the pathophysiology of atypical fractures. There is a widely held belief that changes in bone matrix composition – “frozen bone” – are a key factor. Much of the information behind these theories is derived either from different animal models or transiliac bone biopsies in humans. Findings are inconsistent and sample sizes small. The theories might be able to explain why increased microdamage occurs during bisphosphonate therapy, but are currently unable to grasp the complexity of the fracture occurrence, progression, and inhibited healing of the established incomplete fracture.
Quite a large proportion of atypical fracture patients (10–20%) have no reported use of bisphosphonates and do not seem to suffer from osteoporosis or other diseases affecting bone health (Tan et al. Citation2010). It is likely that these patients share some of the pathophysiological mechanisms of common stress fractures, which would indicate the existence of a background risk of stress fractures of the femoral shaft in the aged population, although very small. Bisphosphonate use might increase this risk, which still remains low.
The formation and growth of microcracks could be a key factor in the development of atypical femoral fractures in bisphosphonate treated and untreated patients. Microcracks in cortical bone of older individuals (80 years of age) are about 3 times more common than in younger individuals (40 years of age) (Diab et al. Citation2006). Older individuals show longer and more linear cracks than younger individuals (Diab et al. Citation2006). In consequence, the formation of a larger crack is more likely in older people. Under physiological conditions, microcracks will be at least partially removed by targeted remodeling. This mechanism might be severely suppressed during bisphosphonate treatment. Also bone matrix properties can be affected negatively by bisphosphonate treatment. As a result, microcracks are less likely to be remodeled in a structurally altered bone with less resistance to microcrack progression.
Physiologically formed microcracks can grow to one or several larger cracks (Frost Citation1989). When this crack reaches a critical size and penetrates the margin of the lateral cortex, micromovements can lead to thigh pain during weightbearing, by irritation of the periosteal envelope. At the same time the extension of the fracture line into the periosteum causes the formation of a callus reaction. Micromotion, leading to strains within the crack could inhibit ingrowth of cells, thereby inhibiting healing. Ultimately, and with minimal trauma, the fracture can progress to a complete, displaced fracture.
Under physiological circumstances the bone surfaces of the fracture gap would be resorbed by osteoclasts, widening the fracture gap. This widening would reduce strains, allow cells to grow into the crack, and bone formation to occur within the gap. Osteoclast dysfunction during ongoing bisphosphonate use might inhibit this resorption, and the fracture gap would remain too thin for cells to survive in it without being crushed. Inhibited resorption of stress fracture surfaces and delayed healing of stress fractures during bisphosphonate treatment has been shown in a stress fracture model of the rat ulna (Sloan et al. Citation2010, Kidd et al. Citation2011).
When bisphosphonate treatment is stopped osteoclast function is likely to recover much quicker than bone structural properties. In Paper I we saw a decrease in the risk of atypical fractures by 70% for each year after treatment was stopped. A similar rapid decrease in fracture risk was found in an extension analysis of Paper I (unpublished data) and by others (Dell et al. 2013). Once osteoclasts can widen the fracture gap, cells growing into it might be able to survive. We could see indirect signs of this cellular recovery in a patient that had stopped bisphosphonate treatment 18 months prior to surgery. We observed remodeling within the crack, creating a bony bridge between the opposing fracture surfaces (). None of the other patients in Paper III, who were on bisphosphonate treatment at the time of surgery, showed signs of remodeling within the gap. We were not able to evaluate local strains in the fracture gap of atypical femoral fractures but Fågelberg et al. (Citation2013) were able to do so in a mathematical model of a tibial stress fracture. They showed that deformations in the fracture gap reach far beyond the critical 2% that prevents bony healing, according to the interfragmentary strain theory by Perren (Citation1979). However, further research is needed to validate our hypothesis ().
Figure 10. Incomplete atypical fracture, 18 months after cessation of bisphosphonate treatment. C periosteal callus. Dashed lines: fracture gap. White arrows: Remodeling within the fracture gap.
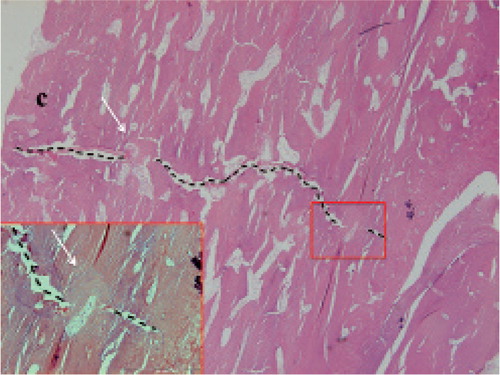
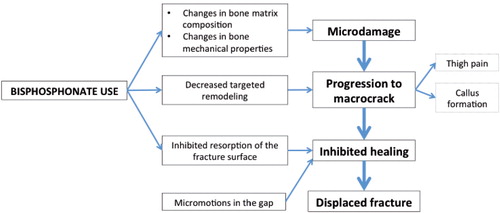
Figure 11. Hypothesis on the series of events leading to atypical femoral fracture.
How long is enough?
There has been a paradigm in osteoporosis research that the greater the suppression of bone turnover, the higher the benefits will be. However, with increasing duration of bisphosphonate use, the increment in risk reduction is likely to become smaller and smaller. In contrast, the risk of atypical fracture continues to increase (Dell et al. Citation2012). Thus, it is possible that by prolonging treatment for another year, we mainly add a risk factor for very little gain. Further research is needed to find the optimal treatment duration for different ages and indications.
Acknowledgements
Per Aspenberg, my supervisor, for his unrestrained sharing of wisdom and his friendship.
Karl Michaëlsson, co-author and co-supervisor, for his invaluable contribution with Paper I and II and for his friendship.
My colleagues at the department of orthopedic surgery for their warm welcome at the start of my residency and for guiding me throughout surgical and scientific training.
Deep gratitude to Ingemar Ivarsson and Lars Palm for their extraordinary sacrifice in mentoring me during almost a decade of surgical training.
Andreas Meunier, head of the department of orthopedic surgery, for providing resources to fulfill this work and for his encouragement.
The PhD students and personnel at the lab. Especially Olof, Anna, Fredrik, Pernilla and Therese, for teaching me different methods and for their help with all “small things” that I did not know had to be done. Teréz for her extraordinary effort in the administration of letters, blood samples and countless other things. Vroni for her thorough work with radiographic measurements in Paper II.
Linköping University, for a well-organized PhD program.
Kristina, my partner, for her love and patience during endless hours of work with this thesis. Thank you for listening to my thoughts, asking wise questions and for the freedom you gave me to fulfill this work.
Vilhelm, my son, for giving me a new kind of happiness and meaningfulness in my life.
Klaus and Ingrid, my parents, for their love, reassurance and support throughout my life and for guidance while letting me choose my own way.
Craig, my friend, for letting me understand as a teenager, that I myself define the boundaries of what I can achieve.
References
- Abrahamsen B, Eiken P, Eastell R. Subtrochanteric and diaphyseal femur fractures in patients treated with alendronate: A register-based national cohort study. J Bone Miner Res 2009; 24(6): 1095–102.
- Abrahamsen BB. Atypical femur fractures: refining the clinical picture. J Bone Miner Res 2012; 27(5): 975–6.
- Allen MR, Burr DB. Bisphosphonate effects on bone turnover, microdamage, and mechanical properties: What we think we know and what we know that we don’t know. Bone 2011; 49(1): 56–65.
- Allen MR, Iwata K, Phipps R, Burr DB. Alterations in canine vertebral bone turnover, microdamage accumulation, and biomechanical properties following 1-year treatment with clinical treatment doses of risedronate or alendronate. Bone 2006; 39(4): 872–9.
- Allen MR, Kubek DJ, Burr DB. Cancer treatment dosing regimens of zoledronic acid result in near-complete suppression of mandible intracortical bone remodeling in beagle dogs. J Bone Miner Res 2009; 25(1): 98–105.
- Aspenberg P, Schilcher J, Fahlgren A. Histology of an undisplaced femoral fatigue fracture in association with bisphosphonate treatment. Acta Orthop 2010; 81(4): 460–2.
- Bala Y, Farlay D, Chapurlat RD, Boivin G. Modifications of bone material properties in postmenopausal osteoporotic women long-term treated with alendronate. Eur J Endocrinol 2011; 165(4): 647–55.
- Bennell KL, Malcolm SA, Wark JD, Brukner PD. Models for the pathogenesis of stress fractures in athletes. Br J Sports Med 1996; 30(3): 200–4.
- Bieglmayer C, Dimai HP, Gasser RW, Kudlacek S, Obermayer-Pietsch B, Woloszczuk W, et al. Biomarker des Knochenumbaus in Diagnose und Therapie der Osteoporose. Wien Med Wochenschr 2012; 162(21-22): 464–77.
- Black DM, Delmas PD, Eastell R, Reid IR, Boonen S, Cauley JA, et al. Once-yearly zoledronic acid for treatment of postmenopausal osteoporosis. N Engl J Med 2007; 356(18): 1809–22.
- Black DM, Kelly MP, Genant HK, Palermo L, Eastell R, Bucci-Rechtweg C, et al. Bisphosphonates and fractures of the subtrochanteric or diaphyseal femur. New England Journal of Medicine. Mass Medical Soc; 2010; 362(19): 1761–71.
- Black DM, Reid IR, Boonen S, Bucci-Rechtweg C, Cauley JA, Cosman F, et al. The effect of 3 versus 6 years of zoledronic acid treatment of osteoporosis: a randomized extension to the HORIZON-Pivotal Fracture Trial (PFT). J Bone Miner Res 2012; 27(2): 243–54.
- Black DM, Schwartz AV, Ensrud KE, Cauley JA, Levis S, Quandt SA, et al. Effects of continuing or stopping alendronate after 5 years of treatment: The Fracture Intervention Trial Long-term Extension (FLEX): A randomized trial. JAMA: The Journal of the American Medical Association 2006; 296(24): 2927–38.
- Black DM, Thompson DE, Bauer DC, Ensrud K, Musliner T, Hochberg MC, et al. Fracture risk reduction with alendronate in women with osteoporosis: the Fracture Intervention Trial. FIT Research Group. J Clin Endocrinol Metab 2000; 85(11): 4118–24.
- Bone HG, Greenspan SL, McKeever C, Bell N, Davidson M, Downs RW, et al. Alendronate and estrogen effects in postmenopausal women with low bone mineral density. Alendronate/Estrogen Study Group. J Clin Endocrinol Metab 2000; 85(2): 720–6.
- Bone HG, Hosking D, Devogelaer J-P, Tucci JR, Emkey RD, Tonino RP, et al. Ten years’ experience with alendronate for osteoporosis in postmenopausal women. N Engl J Med 2004; 350(12): 1189–99.
- Boskey AL, Spevak L, Weinstein RS. Spectroscopic markers of bone quality in alendronate-treated postmenopausal women. Osteoporos Int 2008; 20(5): 793–800.
- Burr DB. Targeted and nontargeted remodeling. Bone 2002; 30(1): 2–4.
- Burr DB, Turner CH, Naick P, Forwood MR, Ambrosius W, Sayeed Hasan M, et al. Does microdamage accumulation affect the mechanical properties of bone? J Biomech 1998; 31(4): 337–45.
- Burr D BD, Forwood M RM, Fyhrie D PD, Martin R BR, Schaffler M BM, Turner C HC. Bone microdamage and skeletal fragility in osteoporotic and stress fractures. J Bone Miner Res 1996; 12(1): 6–15.
- Cardoso L, Herman BC, Verborgt O, Laudier D, Majeska RJ, Schaffler MB. Osteocyte apoptosis controls activation of intracortical resorption in response to bone fatigue. J Bone Miner Res 2009; 24(4): 597–605.
- Chavassieux P MP, Arlot M EM, Reda CC, Wei LL, Yates A JA, Meunier P JP. Histomorphometric assessment of the long-term effects of alendronate on bone quality and remodeling in patients with osteoporosis. J Clin Invest 1997; 100(6): 1475–80.
- Cummings SR. Effect of alendronate on risk of fracture in women with low bone density but without vertebral fractures: Results from the Fracture Intervention Trial. JAMA: The Journal of the American Medical Association. 1998; 280(24): 2077–82.
- Dell R, Greene D, Tran D. Stopping bisphosphonate treatment decreases the risk of having a second atypical femur fracture. 2012 AAOS Annual Meeting Abstract. http://www.aaos-annualmeeting-presskit.org/2012/clinicalpressreleases/osteoporosis.shtml
- Dell RM, Adams AL, Greene DF, Funahashi TT, Silverman SL, Eisemon EO, et al. Incidence of atypical nontraumatic diaphyseal fractures of the femur. J Bone Miner Res 2012; 27(12): 2544–50.
- Delmas PD, Seeman E. Changes in bone mineral density explain little of the reduction in vertebral or nonvertebral fracture risk with anti-resorptive therapy. Bone 2004; 34(4): 599–604.
- Demiralp B, Ilgan S, Ozgur Karacalioglu A, Cicek EI, Yildrim D, Erler K. Bilateral femoral insuffiency fractures treated with inflatable intramedullary nails: a case report. Arch Orthop Trauma Surg 2007; 127(7): 597–601.
- Dencker HM. Fractures of the shaft of the femur. A clinical study based on 1003 fractures treated in Swedish hospitals during the three-year period 1952 to 1954. Thesis. Pp.1-135. University of Gothenburg; 1963.
- Diab T, Condon KW, Burr DB, Vashishth D. Age-related change in the damage morphology of human cortical bone and its role in bone fragility. Bone 2006; 38(3): 427–31.
- Donnelly E, Meredith DS, Nguyen JT, Boskey AL. Bone tissue composition varies across anatomic sites in the proximal femur and the iliac crest. J Orthop Res 2011; 30(5): 700–6.
- Donnelly E, Meredith DS, Nguyen JT, Gladnick BP, Rebolledo BJ, Shaffer AD, et al. Reduced cortical bone compositional heterogeneity with bisphosphonate treatment in postmenopausal women with intertrochanteric and subtrochanteric fractures. J Bone Miner Res 2012; 27(3): 672–8.
- Ettinger B, Burr DB, Ritchie RO. Proposed pathogenesis for atypical femoral fractures: Lessons from materials research. Bone 2013; 55(2): 495–500.
- Fågelberg E, Grassi L, Aspenberg P, Isaksson H. Can widening of a stress fracture decrease local strains sufficiently to enable healing? Accepted conference abstract. In: European Society of Biomechanics, Patras, Greece; 2013 pp. 1–1.
- Feldstein AC, Black DD, Perrin NN, Rosales A GA, Friess DD, Boardman DD, et al. Incidence and demography of femur fractures with and without atypical features. J Bone Miner Res 2012; 27(5): 977–86.
- Follet H, Viguet-Carrin S, Burt-Pichat B, Depalle B, Bala Y, Gineyts E, et al. Effects of preexisting microdamage, collagen cross-links, degree of mineralization, age, and architecture on compressive mechanical properties of elderly human vertebral trabecular bone. J Orthop Res 2010; 29(4): 481–8.
- Follet HH, Li JJ, Phipps R JR, Hui SS, Condon KK, Burr D BD. Risedronate and alendronate suppress osteocyte apoptosis following cyclic fatigue loading. Bone 2007; 40(4): 6–6.
- Fratzl P, Roschger P, Fratzl-Zelman N, Paschalis EP, Phipps R, Klaushofer K. Evidence that treatment with risedronate in women with postmenopausal osteoporosis affects bone mineralization and bone volume. Calcif Tissue Int 2007; 81(2): 73–80.
- Frost HM. Transient-steady state phenomena in microdamage physiology: a proposed algorithm for lamellar bone. Calcif Tissue Int 1989; 44(6): 367–81.
- Frost HM. A brief review for orthopedic surgeons: fatigue damage (microdamage) in bone (its determinants and clinical implications). J Orthop Sci 1998; 3(5): 272–81.
- Girgis CM, Sher D, Seibel MJ. Atypical femoral fractures and bisphosphonate use. N Engl J Med 2010; 362(19): 1848–9.
- Giusti A, Hamdy N AT, Papapoulos SE. Atypical fractures of the femur and bisphosphonate therapy. Bone 2010; 47(2): 169–80.
- Goh S-K, Yang KY, Koh J SB, Wong MK, Chua SY, Chua D TC, et al. Subtrochanteric insufficiency fractures in patients on alendronate therapy: a caution. J Bone Joint Surg Br 2007; 89(3): 349–53.
- Gourion-Arsiquaud S, Faibish D, Myers E, Spevak L, Compston J, Hodsman A, et al. Use of FTIR spectroscopic imaging to identify parameters associated with fragility fracture. J Bone Miner Res 2009; 24(9): 1565–71.
- Güerri-Fernández RC, Nogués X, Quesada Gómez JM, Torres Del Pliego E, Puig L, García-Giralt N, et al. Microindentation for in vivo measurement of bone tissue material properties in atypical femoral fracture patients and controls. J Bone Miner Res 2013; 28(1): 162–8.
- Ing-Lorenzini K, Desmeules J, Plachta O, Suva D, Dayer P, Peter R. Low-energy femoral fractures associated with the long-term use of bisphosphonates. Drug Saf 2009; 32(9): 775–85.
- Johnell O, Kanis JA, Oden A, Johansson H, De Laet C, Delmas P, et al. Predictive value of BMD for hip and other fractures. J Bone Miner Res 2005; 20(7): 1185–94.
- Kidd LJ, Cowling NR, Wu A CK, Kelly WL, Forwood MR. Bisphosphonate treatment delays stress fracture remodeling in the rat ulna. J Orthop Res 2011; 29(12): 1827–33.
- Koeppen VA, Schilcher J, Aspenberg P. Atypical fractures do not have a thicker cortex. Osteoporos Int 2012; 23(12): 2893–6.
- Komatsubara SS, Mori SS, Mashiba TT, Ito MM, Li JJ, Kaji YY, et al. Long-term treatment of incadronate disodium accumulates microdamage but improves the trabecular bone microarchitecture in dog vertebra. J Bone Miner Res 2003; 18(3): 512–20.
- Lenart BA, Lorich DG, Lane JM. Atypical fractures of the femoral diaphysis in postmenopausal women taking alendronate. N Engl J Med 2008; 358(12): 1304–6.
- Li J, Mashiba T, Burr DB. Bisphosphonate treatment suppresses not only stochastic remodeling but also the targeted repair of microdamage. Calcif Tissue Int 2001; 69(5): 281–6.
- Mackie PS, Fisher JL, Zhou H, Choong PF. Bisphosphonates regulate cell growth and gene expression in the UMR 106-01 clonal rat osteosarcoma cell line. Br J Cancer 2001; 84(7): 951–8.
- Marshall D, Johnell O, Wedel H. Meta-analysis of how well measures of bone mineral density predict occurrence of osteoporotic fractures. BMJ 1996; 312(7041): 1254–9.
- Mashiba T, Dell RM, Mori S, Adams AL, Burr DB, Greene DF, et al. The effects of suppressed bone remodeling by bisphosphonates on microdamage accumulation and degree of mineralization in the cortical bone of dog rib. J Bone Miner Metab 2005; 23 Suppl: 36–42.
- Mashiba T, Turner CH, Hirano T, Forwood MR, Johnston CC, Burr DB. Effects of suppressed bone turnover by bisphosphonates on microdamage accumulation and biomechanical properties in clinically relevant skeletal sites in beagles. Bone 2001; 28(5): 524–31.
- Mashiba TT, Hirano TT, Turner C HC, Forwood M RM, Johnston C CC, Burr D BD. Suppressed bone turnover by bisphosphonates increases microdamage accumulation and reduces some biomechanical properties in dog rib. J Bone Miner Res 2000; 15(4): 613–20.
- Meijer WM, Penning-van Beest F JA, Olson M, Herings R MC. Relationship between duration of compliant bisphosphonate use and the risk of osteoporotic fractures. Curr Med Res Opin 2008; 24(11): 3217–22.
- Mellstrom DD, Sörensen OH, Goemaere S, Roux C, Johnson TD, Chines AA. Seven years of treatment with risedronate in women with postmenopausal osteoporosis. Calcif Tissue Int 2004; 75(6): 462–8.
- Miller LM, Little W, Schirmer A, Sheik F, Busa B, Judex S. Accretion of bone quantity and quality in the developing mouse skeleton. J Bone Miner Res 2007; 22(7): 1037–45.
- Neviaser AS, Lane JM, Lenart BA, Edobor-Osula F, Lorich DG. Low-energy femoral shaft fractures associated with alendronate use. J Orthop Trauma 2008; 22(5): 346–50.
- Norman TL, Wang Z. Microdamage of human cortical bone: incidence and morphology in long bones. Bone 1997; 20(4): 375–9.
- Odvina CV, Zerwekh JE, Rao DS, Maalouf N, Gottschalk FA, Pak CY. Severely suppressed bone turnover: a potential complication of alendronate therapy. J Clin Endocrinol Metab 2005; 90(3): 1294–301.
- Perren SM. Physical and biological aspects of fracture healing with special reference to internal fixation. Clin Orthop Relat Res 1979; (138): 175–96.
- Renders G A P, Mulder L, van Ruijven L J, Langenbach G E J, van Eijden T M G J. Mineral heterogeneity affects predictions of intratrabecular stress and strain. J Biomech 2011; 44(3): 402–7.
- Rydholm A. Highly different risk estimates for atypical femoral fracture with use of bisphosphonates - debate must be allowed! Acta Orthop 2012; 83(4): 319–20.
- Sahni M, Guenther HL, Fleisch H, Collin P, Martin TJ. Bisphosphonates act on rat bone resorption through the mediation of osteoblasts. J Clin Invest 1993; 91(5): 2004–11.
- Schilcher J, Aspenberg P. Incidence of stress fractures of the femoral shaft in women treated with bisphosphonate. Acta Orthop 2009; 80(4): 413–5.
- Schilcher J, Koeppen V, Ranstam J, Skripitz R, Michaëlsson K, Aspenberg P. Atypical femoral fractures are a separate entity, characterized by highly specific radiographic features. A comparison of 59 cases and 218 controls. Bone 2013; 52(1): 389–92.
- Schilcher J, Michaëlsson K, Aspenberg P. Bisphosphonate use and atypical fractures of the femoral shaft. N Engl J Med 2011; 364(18): 1728–37.
- Schindeler A, Little DG. Osteoclasts but not osteoblasts are affected by a calcified surface treated with zoledronic acid in vitro. Biochem Biophys Res Commun 2005; 338(2): 710–6.
- Schneider JP. Should bisphosphonates be continued indefinitely? An unusual fracture in a healthy woman on long-term alendronate. Geriatrics 2006; 61(1): 31–3.
- Shane E, Burr D, Abrahamsen B, Adler RA, Brown TD, Cheung AM, et al. Atypical subtrochanteric and diaphyseal femoral fractures: Second report of a task force of the American society for bone and mineral research. J Bone Miner Res 2013 May 28. doi: 10.1002/jbmr.1998. [Epub ahead of print].
- Shane E, Burr D, Ebeling PR, Abrahamsen B, Adler RA, Brown TD, et al. Atypical subtrochanteric and diaphyseal femoral fractures: report of a task force of the American Society for Bone and Mineral Research. J Bone Miner Res 2010; 25(11): 2267–94.
- Sloan AV, Martin JR, Li S, Li J. Parathyroid hormone and bisphosphonate have opposite effects on stress fracture repair. Bone 2010; 47(2): 235–40.
- Smith SY, Recker RR, Hannan M, Müller R, Bauss F. Intermittent intravenous administration of the bisphosphonate ibandronate prevents bone loss and maintains bone strength and quality in ovariectomized cynomolgus monkeys. Bone 2003; 32(1): 45–55.
- Somford MP, Draijer FW, Thomassen BJ, Chavassieux PM, Boivin G, Papapoulos SE. Bilateral fractures of the femur diaphysis in a patient with rheumatoid arthritis on long-term treatment with alendronate: Clues to the mechanism of increased bone fragility. J Bone Miner Res 2009; 24(10): 1736–40.
- Tai K, Dao M, Suresh S, Palazoglu A, Ortiz C. Nanoscale heterogeneity promotes energy dissipation in bone. Nat Mater 2007; 6(6): 454–62.
- Tan SC, Koh S BJ, Goh SK, Howe TS. Atypical femoral stress fractures in bisphosphonate-free patients. Osteoporos Int 2010; 22(7): 2211–2.
- Tang SY, Allen MR, Phipps R, Burr DB, Vashishth D. Changes in non-enzymatic glycation and its association with altered mechanical properties following 1-year treatment with risedronate or alendronate. Osteoporos Int 2009; 20(6): 887–94.
- Tjhia CK, Odvina CV, Rao DS, Stover SM, Wang X, Fyhrie DP. Mechanical property and tissue mineral density differences among severely suppressed bone turnover (SSBT) patients, osteoporotic patients, and normal subjects. Bone 2011; 49(6): 1279–89.
- Valcourt U, Merle B, Gineyts E, Viguet-Carrin S, Delmas PD, Garnero P. Non-enzymatic glycation of bone collagen modifies osteoclastic activity and differentiation. J Biol Chem 2007; 282(8): 5691–703.
- Vashishth D, Behiri JC, Bonfield W. Crack growth resistance in cortical bone: concept of microcrack toughening. J Biomech 1997; 30(8): 763–9.
- Vashishth D, Gibson GJ, Khoury JI, Schaffler MB, Kimura J, Fyhrie DP. Influence of nonenzymatic glycation on biomechanical properties of cortical bone. Bone 2001; 28(2): 195–201.
- Viereck V, Emons G, Lauck V, Frosch K-H, Blaschke S, Gründker C, et al. Bisphosphonates pamidronate and zoledronic acid stimulate osteoprotegerin production by primary human osteoblasts. Biochem Biophys Res Commun 2002; 291(3): 7–7.
- Weinstein RS, Roberson PK, Manolagas SC. Giant osteoclast formation and long-term oral bisphosphonate therapy. New Engl J Med 2009; 360(1): 53–62.
- Yamagami Y, Mashiba T, Iwata K, Tanaka M, Nozaki K, Yamamoto T. Effects of minodronic acid and alendronate on bone remodeling, microdamage accumulation, degree of mineralization and bone mechanical properties in ovariectomized cynomolgus monkeys. Bone 2013; 54(1): 1–7.
- Yu W, Glüer CC, Fuerst T, Grampp S, Li J, Lu Y, et al. Influence of degenerative joint disease on spinal bone mineral measurements in postmenopausal women. Calcif Tissue Int 1995; 57(3): 169–74.