
Abstract
Background and purpose — The alpha angle is the most used measurement to classify concavity of the femoral head-neck junction. It is not only used for treatment decisions for hip impingement, but also in cohort studies relating hip morphology and osteoarthritis. Alpha angle measurement requires identification of the femoral neck axis, the definition of which may vary between studies. The original “3-point method” uses 1 single point to construct the femoral neck axis, whereas the “anatomic method” uses multiple points and attempts to define the true anatomic neck axis. Depending on the method used, the alpha angle may or may not account for other morphological characteristics such as head-neck offset.
Methods — We compared 2 methods of alpha angle measurement (termed “anatomic” and “3-point”) in 59 cadaver femora and 83 cross-table lateral radiographs of asymptomatic subjects. Results were compared using Bland-Altman plots.
Results — Discrepancies of up to 13 degrees were seen between the methods. The 3-point method had an “equalizing effect” by disregarding femoral head position relative to the neck: in femora with high alpha angle, it resulted in lower values than anatomic measurement, and vice versa in femora with low alpha angles. Using the anatomic method, we derived a reference interval for the alpha angle in normal hips in the general population of 30–66 degrees.
Interpretation — We recommend the anatomic method because it also reflects the position of the femoral head on the neck. Consensus and standardization of technique of alpha angle measurement is warranted, not only for planar measurements but also for CT or MRI-based measurements.
Hip morphology variants may influence the development of osteoarthritis (OA) (Ganz et al. Citation2008). Femoral morphology variants may be best characterized by concavity, a compound measure determined by the sphericity and offset of the femoral head (determined from relative neck width and femoral head position on the neck). The most used concavity measure is the alpha angle, described initially by Nötzli et al. (Citation2002) to diagnose cam deformity and increasingly used in cohort studies examining the risk of OA development (Johnston et al. Citation2008, Nicholls et al. Citation2011, Agricola et al. Citation2013). Nötzli et al. (Citation2002) measured the alpha angle between 2 lines drawn between 3 points (“3-point method”). One line is called the femoral neck axis based on a single point at the center of the narrowest part of the femoral neck (), but it is important to recognize that this line will only correspond to the anatomic femoral neck axis if the femoral head is positioned centrally on the neck.
Figure 1. 3-point and anatomic method compared in high alpha angle (A) and low alpha angle (B). 3-point method (A.1 and B.1) uses the midpoint of the femoral neck at its narrowest point. The anatomic method (B.2 and B.2) defines the femoral neck axis by connecting the centers of 3 circles projected over the neck contour. The axis is translated to the center of the femoral head if necessary, to measure the alpha angle. In this example, alpha angle A.1 = 64˚, A.2 = 73˚. Angle B.1 and B.2 are both 30˚, while the femoral head is positioned central on the femoral neck.
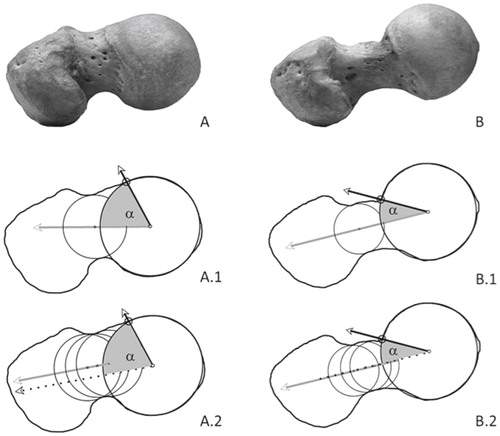
However, in many human femora the position of the femoral head on the neck may not be central, but shifted or tilted posteriorly (Murray and Duncan Citation1971, Hogervorst et al. Citation2009). In such femora, use of a femoral neck axis line connecting the center of the femoral head and neck will decrease the alpha angle (). Use of the anatomic center line (the “anatomic method”) rather than a single point for the femoral neck axis (the “3-point method”) probably more accurately represents femoral head-neck morphology, as it may also account for femoral head translation as measured by the anterior offset ratio (Eijer et al. Citation2001, Pollard et al. Citation2010). Furthermore, the increasing number of cohort studies using the alpha angle mandates consensus on measurement technique.
Measurements in 155 cross-table radiographs
We hypothesized that the 2 measurement methods differ in their representation of proximal femoral morphology. Specifically, we asked: (1) What is the degree of correlation of each method with the anterior offset ratio (AOR)? (2) What is the reference interval for the alpha angle in normal hips in the general population?
Methods
Methods of measurement of alpha angle ()
For the 3-point method, we placed a best-fit circle over the osseous contour of the femoral head. Next, we placed a circle over the narrowest part of the femoral neck (i.e. the shortest possible distance between the anterior (ventral) and posterior (dorsal) outline of the femoral neck on the photographs or radiographs). A line was drawn connecting the center of these 2 circles. Then a line was drawn connecting the center of the femoral head circle to the point where the contour of the femoral head or head-neck junction first exited the femoral head circle. The alpha angle was then measured as the angle between these 2 lines.
For the anatomic method, first the axis of the neck was determined by placing 3 circles, touching the contour of the neck. The middle circle was the same as the 3-point circle as described above. The 2 remaining circles were placed on either side of the first circle as distantly as possible, while ensuring that the center of these circles was still placed on the neck. Then, a line was drawn as a best fit over the centers of these circles. The accuracy of placement of this line was verified visually. When the axis was confirmed, we placed a best-fit circle over the femoral head and a line connecting the center of the femoral head circle to the point where the femoral head contour exited the femoral head circle (i.e. the femoral head was measured in a manner identical to the 3-point method). If necessary, the anatomic femoral neck axis line was translated to the center of the femoral head circle. The alpha angle was then measured as the acute angle between these 2 lines.
Method of measurement of anterior offset ratio (AOR)
The AOR (Eijer et al. Citation2001, Pollard et al. Citation2010) was calculated by first defining the anatomic femoral neck axis, as described above. Parallel lines were then drawn along the anterior cortex of the neck and along the anterior outer part of the femoral head. The perpendicular distance between these latter 2 lines was the anterior offset. AOR is calculated by dividing the anterior offset by the diameter of the femoral head.
We used the GNU Image Manipulation Program version 2.8 (www.gimp.org) to perform all measurements.
Photographs of cadaver femora
The photographs of cadaver femora described earlier by Toogood et al. (Citation2009) were re-measured. We choose these specimens to approximate optimum measurement conditions. In this study, visualization of the femoral neck and head-neck junction was optimized by positioning the lens of the camera parallel to the femoral neck axis in the coronal plane (Toogood et al. Citation2009). Parallelism was checked visually. To examine the difference between the 2 measurement methods for alpha angle, we compared the anatomic and 3-point method in 3 groups of 20 specimens each of the 20 highest, 20 median, and 20 lowest alpha angles. 1 specimen in the high-alpha group was excluded due to low image quality, leaving 59 cadaver femora for analysis (29 male).
Cross-table lateral radiographs
The cross-table lateral radiographs described in detail by Pollard et al. (Citation2010) were re-measured. We choose these radiographs because this cohort represents normal hips in the general population and it was therefore deemed suitable upon which to base a reference-interval calculation. All subjects in this cohort underwent an interview and clinical examination as described in detail earlier, and they were free of hip signs and symptoms. All cross-table lateral radiographs were taken with the femur internally rotated 15 degrees, using a 15-degree wedge under the lateral femoral condyle.
The cohort consisted of 166 radiographs in 83 individuals. 11 radiographs were excluded due to low image quality (n = 1) or difficulty in identifying the femoral neck contour (n = 10), for example due to overprojection of the greater trochanter. The remaining 155 radiographs were measured using both methods (anatomic and 3-point). Independent t-test showed no difference in alpha angles between males and females for the anatomic method (p = 0.7) or 3-point method (p = 0.9) in radiographs. The male and female groups were therefore combined into 1 radiographic group.
The 95% reference intervals for the alpha angle were calculated and compared between methods.
Statistics
Statistical analysis was done using PASW Statistics 17.0. The Kolmogorov-Smirnov test was used to test whether the radiographic group was normally distributed for both measurement methods. This was not the case for the cadaver group, because we selected the 20 highest, middle, and lowest samples from 375 specimens. Bland-Altman plots were used to analyze the difference between the 2 measurement methods. Student’s t-test was used for the confidence intervals and statistical characteristics in the radiographic measurements. The 95% reference intervals were calculated as the mean ± 1.96 SD. The Spearman test was used to calculate the correlation of the 2 alpha angle methods and the AOR. To identify whether the difference in r values of both methods was statistically significant, Steiger’s test was used (Steiger Citation1980). Statistical significance was assumed at p-values of < 0.05.
Power calculation
We calculated the power needed to find a difference of 5 degrees between the 2 measurement methods with an SD of 9 degrees in the data provided by Pollard et al. (Citation2010), and we found that 23 measurements were needed. As we used 155 samples, the power of this study was 0.99. We choose to measure all 155 radiographs of sufficient quality in order to obtain the best possible information from the Bland-Altman plot.
Interobserver agreement
The interclass correlation coefficient (ICC) was calculated between the measurements by 2 observers. Both observers (HB and NS) independently measured the alpha angles according to the 2 methods on 59 photographs of cadaver femora and 155 crosstable lateral radiographs. After 10 trial measurements with each method, both observers agreed on how to determine the contour of the femoral neck, taking into account overprojection of the greater trochanter (when present) on radiographs. Interobserver agreement was calculated for both methods and for both samples (photographs and radiographs). The ICCs for all 4 measurement groups were found to be excellent (defined as ICC > 0.9 (0.95–0.99); p < 0.001 for all 4 measurement groups).
Results
Representation of anatomy
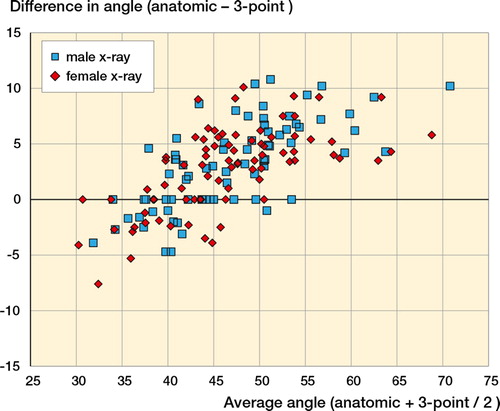
The Bland-Altman plots for cadaver femora and for radiographs showed that in femora with high alpha angles, the anatomic method resulted in higher values than the 3-point method, while in femora with low alpha angles, the anatomic method gave lower values than the 3-point method ( and ). Thus, compared to the anatomic method, the 3-point method had a “leveling” or “equalizing” effect on alpha angle measurement: high values with the anatomic method were lower with the 3-point method and vice versa for low values. The maximum discrepancy in alpha angle measurement between the 2 methods was 13.5 degrees in a cadaver femur and 10.8 degrees in a radiograph.
Figure 2. Bland-Altman plot of the measurements of cadaver photographs. The x-axis depicts the average of 2 measurements for each cadaver femur. The y-axis depicts their difference (anatomic minus 3-point).
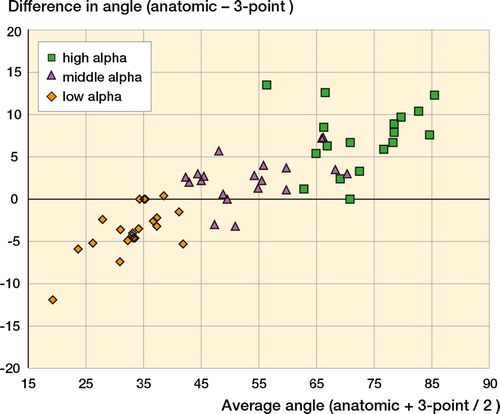
Figure 3. Bland-Altman plot of the measurements of radiographs. The x-axis depicts the average of 2 measurements for each cadaver femur. The y-axis depicts their difference (anatomic minus 3-point).
Correlation of alpha angle with anterior offset ratio (AOR)
The Spearman test showed stronger correlation with AOR for the anatomic method than for the 3-point method: 0.74 (95% CI: 0.68–0.8) vs. 0.68 (95% CI: 0.54–0.7), respectively (p < 0.001).
Reference interval
The anatomic method gave a wider reference interval than the 3-point method (Table). This means that using the anatomic method, alpha angles above 66 degrees can be considered abnormal, while this value would be 58 degrees for the 3-point method using the same group of radiographs.
Discussion
When introduced in 2002, the reason stated for choosing the 3-point method was its simplicity, supported by adequate intra- and interobserver agreement (with an interobserver value of ± 7%) (Nötzli et al. Citation2002). No direct comparison with another method to represent the femoral neck axis was made, however. We made such a comparison between the 3-point method and the anatomic method and found no difference in interobserver agreement (ICC) between the 2, either in cadaver measurements or in radiographic measurements. Our ICC values correspond to those found by Meyer et al. (Citation2006).
We interpret the equalizing effect of the 3-point method in measuring alpha angles as being a consequence of the compound nature of the alpha angle. When the femoral head is translated posteriorly, the 3-point method decreases the alpha angle. Posterior position of the femoral head is mostly seen with high alpha angles (low concavity), as can be found in cam morphotype (Toogood et al. Citation2009, Ellis et al. Citation2011). Conversely, anterior femoral head translation is associated with lower alpha angles.
We recommend using the anatomic femoral neck axis because this method accounts for the translation that may be measured separately by the AOR (which also references the anatomic neck axis). The anatomic method expresses femoral head position relative to the neck as part of the morphotype, whereas the 3-point method may mask it by tilting the femoral neck axis (). Accordingly, the anatomic method correlates better with the AOR than the 3-point method. For hips with poor head-neck offset, the anatomic method will increase their alpha angles appropriately, which may make the AOR redundant and simplify assessment of morphology.
Our study had several limitations. We used cross-table lateral radiographs but we do acknowledge that Dunn views are more sensitive in detecting cam deformity (Meyer et al. Citation2006, Domayer et al. Citation2011). Nevertheless, our study was not designed to improve sensitivity for cam detection. Anatomic representation and standardization of the femoral neck axis is desirable regardless of imaging tool or technique, including concavity measurements on anteroposterior radiographs and 3-D imaging such as CT or MRI. 3-D imaging facilitates identification of the anatomic femoral neck axis because there is no overprojection of other structures such as the greater trochanter—a limitation we encountered in 10 of 166 radiographs. To minimize inconsistency of imaging technique and projection, we also examined cadaver femora. In the cadaver study, femoral neck version was controlled for and projection of the head-neck junction was optimized as described previously (Toogood et al. Citation2009). Nevertheless, our findings were almost identical for both cadaver studies and radiographic studies.
The smaller number of radiographs measured in this study (n = 155) compared to that in the earlier study by Pollard et al. (n = 166) also explains the difference we observed in the reference interval for cross-table lateral radiographs with the 3-point method (32–58˚ and 32–62˚, respectively). Thus, differences in study population and imaging method can lead to different reference intervals. We caution against treatment algorithms for FAI based solely or mainly on alpha angle measurements and their cut-off values. Whether or not operative FAI treatment is a sensible option depends on clinical judgment, weighing not only an individual’s morphology—including acetabular morphology—but also his/her cartilage biology and activity pattern (Hogervorst et al. Citation2012).
In conclusion, both techniques of alpha angle measurement had excellent reliability in this study. The 3-point method had an equalizing effect on the alpha angle because it disregards the position of the femoral head relative to the neck. We recommend the anatomic method, as it better characterizes hip morphology by accounting for the position of the head on the neck.
HB and NS performed all measurements. PT contributed with photographs of the cadaver specimens. TP contributed with radiographs of the control population. PK and HB performed the analysis. TH designed the study. TH, HB, PT, and TP prepared the manuscript.
HB was supported by an educational grant from Depuy Johnson and Johnson and Link GmbH.
No competing interests declared.
- Agricola R, Heijboer MP, Bierma-Zeinstra SM, Verhaar JA, Weinans H, Waarsing JH. Cam impingement causes osteoarthritis of the hip: a nationwide prospective cohort study (CHECK). Ann Rheum Dis 2013; 72 (6): 918-23.
- Domayer SE, Ziebarth K, Chan J, Bixby S, Mamisch TC, Kim YJ. Femoroacetabular cam-type impingement: Diagnostic sensitivity and specificity of radiographic views compared to radial MRI. Eur J Radiol 2011; 80 (3): 805-10.
- Eijer H, Leunig M, Mahomed N, Ganz R. Cross-table lateral radiographs for screening of anterior femoral head–neck offset in patients with femoroacetabular impingement. Hip Int 2001; 11: 37-41.
- Ellis A, Noble PC, Schroder J, Thompson M, Stocks G. The cam impinging femur has multiple morphologic abnormalities. J Arthroplasty (6 Suppl) 2011; 26: 59-65.
- Ganz R, Leunig M, Leunig-Ganz K, Harris WH. The etiology of osteoarthritis of the hip: an integrated mechanical concept. Clin Orthop 2008; (466) (2): 264-72.
- Hogervorst T, Bouma HW, de Vos J. Evolution of the hip and pelvis. Acta Orthop (Suppl 336) 2009; 80: 1-39.
- Hogervorst T, Eilander W, Fikkers JT, Meulenbelt I. Hip ontogenesis: How evolution, genes, and load history shape hip morphotype and cartilotype. Clin Orthop 2012; 28; ( 470) (12): 3284-96.
- Johnston TL, Schenker ML, Briggs KK, Philippon MJ. Relationship between offset angle alpha and hip chondral injury in femoroacetabular impingement. Arthroscopy 2008; 24 (6): 669-75.
- Meyer DC, Beck M, Ellis T, Ganz R, Leunig M. Comparison of six radiographic projections to assess femoral head/neck asphericity. Clin Orthop 2006; (445): 181-5.
- Murray RO, Duncan C. Athletic activity in adolescence as an etiological factor in degenerative hip disease. J Bone Joint Surg (Br) 1971; 53 (3): 406-19.
- Nicholls AS, Kiran A, Pollard TC, Hart D, Arden CP, Spector T, et al. The association between hip morphology parameters and 19-year risk of end-stage osteoarthritis in the hip: A nested case-control study. Arthritis Rheum 2011; 63 (11): 3392-400.
- Nötzli HP, Wyss TF, Stoecklin CH, Schmid MR, Treiber K, Hodler J. The contour of the femoral head-neck junction as a predictor for the risk of anterior impingement. J Bone Joint Surg (Br) 2002; 84 (4): 556-60.
- Pollard TC, Villar RN, Norton MR, Fern ED, Williams MR, Simpson DJ, et al. Femoroacetabular impingement and classification of the cam deformity: the reference interval in normal hips. Acta Orthop 2010; 81 (1): 134-41.
- Steiger JH. Tests for comparing elements of a correlation matrix. Psychol Bull 1980; 87 (2): 245-51.
- Toogood PA, Skalak A, Cooperman DR. Proximal femoral anatomy in the normal human population. Clin Orthop 2009; (467) (4): 876-85.