
Abstract
Background and purpose — Neglected clubfoot deformity is a major cause of disability in low-income countries. Most children with clubfoot have little access to treatment in these countries, and they are often inadequately treated. We evaluated the effectiveness of Ponseti’s technique in neglected clubfoot in children in a rural setting in Ethiopia.
Patients and methods — A prospective study was conducted from June 2007 through July 2010. 22 consecutive children aged 2–10 years (32 feet) with neglected clubfoot were treated by the Ponseti method. The deformity was assessed using the Pirani scoring system. The average follow-up time was 3 years.
Results — A plantigrade functional foot was obtained in all patients by Ponseti casting and limited surgical intervention. 2 patients (4 feet) had recurrent deformity. They required re-manipulation and re-tenotomy of the Achilles tendon and 1 other patient required tibialis anterior transfer for dynamic supination deformity of the foot.
Interpretation — This study shows that the Ponseti method with some additional surgery can be used successfully as the primary treatment in neglected clubfoot, and that it minimizes the need for extensive corrective surgery.
Many children with congenital talipes equino varus (CTEV) in low-income countries end up with neglected clubfoot deformity (untreated children > 2 years) because of the lack of treatment capacity. In Ethiopia, it is estimated that there are 3,000–5,000 new CTEV cases per year, but there are no reliable data available.
Neglected clubfoot is a common, disabling problem in Ethiopia. For many years, the treatment for clubfoot in Ethiopia has been nonoperative treatment with Kite’s technique, followed by a posteromedial release, with significant surgical complications and poor results (personal observations by the authors). A dramatic reduction in radical clubfoot operation has been reported in parts of the world where Ponseti treatment has been introduced (Morquende et al. 2004, Zionts et al. Citation2010). We have the same subjective impression in Ethiopia, but there are no published data.
Ponseti treatment was introduced in Ethiopia in June 2005 at the Orthopaedic Department, Black Lion Hospital (BLH), University of Addis Ababa. It has gradually been adopted in several places in a cooperation between BLH and Cure International, Ethiopia. Several thousand children have been involved.
In the past decade, the Ponseti method has become recognized globally as the gold standard for clubfoot treatment in younger children (< 2 years old) (Cooper et al. Citation1995, Bor et al. Citation2009, Pirani et al. Citation2009, Sætersdal et al. Citation2012).
There have been some reports of Ponseti treatment being given successfully to children with neglected clubfoot (Verma et al. Citation2012, Laurenco et al. 2007, Alves et al. Citation2009), but there has been no general acceptance of treating children older than 2 years with this method. Today, these children are probably treated with radical operations or left untreated (De Rosa and Norrish Citation2012).
Inspired by the results of A. F. Laurenco, which were communicated personally before his article was published in 2007, we treated some neglected children over the age of 2 years when the Ponseti treatment was started in Addis Ababa (at BLH), and the initial results were encouraging.
The objective of this study was to prospectively evaluate the short-term results of using the Ponseti technique for treatment of children with neglected clubfoot deformity in a rural hospital in Ethiopia.
Patients and methods
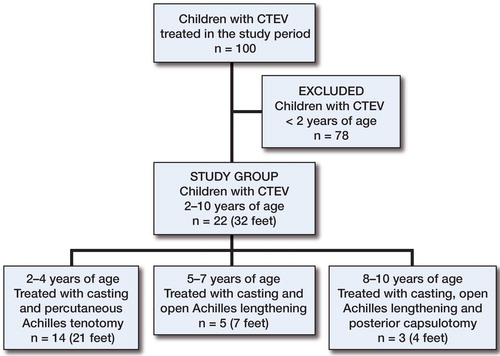
The patients in the present study were all treated at St. Luke Catholic General Hospital, Wolliso, a rural hospital situated 120 km outside Addis Ababa. Between June 2007 and July 2010, 22 consecutive children (17 boys) older than 2 years with 32 neglected idiopathic clubfeet were treated using the Ponseti method. These 22 children represent all the children older than 2 years with neglected clubfoot seen during the study period, as none were left untreated or taken directly to surgery. The age is estimated, since most of the parents did not know the exact age.
At the same time, 78 children below the age of 2 years with CTEV were treated successfully with the Ponseti method, but they were not included in this study group ().
Figure 1. Flow chart of the patients.
There is no reliable registration of deformities at birth and no functioning referral system for children with clubfoot, so we have no information on how many children with clubfoot were left untreated, and the size of the population base for these children cannot be established.
The mean age of the 22 children in the study group at the start of treatment was 4.4 (2–10) years. The deformity was bilateral in 11 of 22. The severity of deformity was assessed using Pirani scoring (Pirani Citation2003, Dyer and Davis Citation2006). The feet were documented with photographs and Pirani scoring before and after treatment. None of the children had a history of previous treatment, except for 2 children who had been on Kite casting before Ponseti treatment was started. The procedure was explained to the parents to create awareness and to give them an understanding of the importance of regular follow-up. The treatment was free, but most parents had to provide their own transport. A counselor was responsible for additional counseling of the families, also emphasizing the importance of follow-up.
The manipulation and plastering technique strictly followed the original protocol described by Dr Ponseti (Ponseti Citation1992, Staheli Citation2003), except that the long leg cast was applied every 2 weeks instead of every week. All components of the deformity were corrected by serial manipulation and casting, except the equinus deformity. The equinus deformity was corrected by percutaneous Achilles tenotomy (PAT) or open lengthening of Achilles tendon (ATL)—alone or in combination with posterior capsulotomy. All treatment, including both the casting and limited surgical intervention, was performed by the first author. Following tenotomy or limited surgery, long leg casts were applied for 4 weeks. After removal of the casts, the correction was maintained with an abduction brace. For patients up to 4 years of age, the brace was used for 2–3 months, 24 hours a day, and after that during the night for 1 year. Ankle-foot-orthoses (AFOs) were applied for patients above 4 years of age, for 1 year full time. All feet in this study were followed clinically for an average period of 3 years (range 2–4 years).
Results
All patients had severe deformity corresponding to a Pirani score of 4–6, with mean score of 5. The deformities of the clubfoot were corrected by the casts, except equinus deformity. shows a 3-year-old boy and shows a 4-year-old boy before and after treatment.
Figure 2. 3-year-old boy before treatment. After 5 casts.The sixth cast. After PAT.

Figure 3. 4-year-old boy before treatment. After treatment.

The midfoot was corrected to Pirani 0 in all feet after the casts. The correction was obtained with an average of 8 (6–10) casts, the number of casts increasing with age. In patients up to the age of 4 years, hyperabduction up to 60–70 degrees was achieved in the final cast. In the older children, abduction was only possible up to 30–40 degrees, but this did not appear to reduce the final walking ability. shows how the residual equinus was treated. All the children who had open procedures were 5 years old or more. Postoperatively, a long leg cast was applied and kept on for 4 weeks. The 3 children who had ATL and posterior capsulotomy were the 3 oldest: at 8, 9, and 10 years of age. There were no major complications during cast application or during the limited surgical interventions. No extensive soft tissue releases or corrective bony procedures were required to obtain correction. The equinus was corrected to above neutral in dorsiflexion. All the children obtained a corrected, plantigrade, flexible, pain free-foot. The latter was based on clinical judgment, and no detailed pain scoring was done. They could all walk and run. A significant improvement in the cosmetic appearance was observed in all children. They could perform their normal daily activities and were all able to wear normal shoes for the first time in their lives.
2 patients (4 feet) required re-manipulation and casting and a new ATL for recurrent deformity. Neither child had used the orthosis as planned. The first child was 5 years old when the first treatment was started, and at first had 6 casts and ATL. Recurrence came 8 months later. The second child was 8 years old (see ) when the first treatment was started, and at first he had 8 casts and ATL with posterior capsulotomy bilaterally. There was then a recurrence 1 year later. Both children were treated with recasting and a new ATL.
Figure 4. 8-year-old boy before treatment. After treatment.

1 patient was lost to follow-up after 2 regular post-casting follow-up visits. He was given a foot abduction brace when he was 3.5 years old, but the parents gave up the abduction brace and he was then given an AFO, but after that there were no new contacts. However, at the last visit the foot was well corrected. Except for these 3 children, the rest of the children used their orthoses as planned.
Dynamic supination was found in 1 child. The first treatment of this child was started at the age of 4 years with casting and PAT, and recurrence was recognized after 3 years. It was a bilateral CTEV, but the recurrence came in 1 foot and at the age of 7 years; tibialis anterior was transferred to the lateral cuneiforme bone on the recurrent side. This operation was performed in another hospital.
Discussion
The study shows that children with neglected clubfoot can be treated successfully with the Ponseti method and that the need for extensive radical operations can be greatly reduced. Still, we know that recurrence might occur with longer follow-up.
We experienced that the Pirani score of the hindfoot was difficult to evaluate in older children, both before and after the treatment. At the start we got a lower Pirani score in the oldest children. According to our observations, the posterior crease and the calcaneal fat pad change as the child grows, so that the bony parts of calcaneus are more prominent and the posterior crease can be normalized even in a severe equinus. Thus, the sign of empty heal and the posterior crease might be less reliable in older children.
Laurenco et al. (2007) described successful results from Brazil after Ponseti treatment in 17 children (24 feet) with an average age at presentation of 3.9 (1.2–9.0). A painless plantigrade foot was achieved in 16 feet without the need for extensive surgery and those who eventually needed surgery ended up with a lesser surgical intervention. One-third of the pataients had recurrence. The best results were achieved in the youngest group. The authors also achieved only 40 degrees of abduction in the older group, which was the same as we observed.
Other studies conducted in low income countries (LIC) have found good results for Ponseti treatment of neglected clubfoot children. In Malawi, adequate correction was achieved in 98 of 100 feet (in 75 children). The mean age at presentation was 11.5 weeks. 19 patients (25%) were in the age group between 18 and 48 months, so some of these children must have been neglected even though they were much younger than our patients (Tindall et al. Citation2005).
We had similar findings to those of Verma et al. (Citation2012) from India. They had 37 patients with idiopathic clubfoot (55 clubfeet). Mean age at presentation was 2 (1–3) years. After a Ponseti trial, 4 patients (6 feet) were considered unfit for Ponseti treatment and posteromedial release. The 33 patients who continued Ponseti treatment (49 feet) all had a satisfactory outcome. The patients were generally younger than our patients. One important difference is that we did not include children younger than 2 years.
From Istanbul, Turkey, Yagmurlu et al. (Citation2011) reported 31 feet (27 patients)—mean age 2 (1–6) years—treated with the Ponseti method. They divided the patients into 2 age groups, younger than 20 months and older than 20 months. They concluded that the Ponseti method is effective in correcting the deformities of clubfoot, even in children of walking age, but the treatment may be less effective with increasing age. They recommended that the Ponseti method should be used even though full correction cannot always be achieved, as a subsequent surgical intervention—if needed—would be much less invasive.
From Nepal, Spiegel et al. (Citation2009) reported the use of Ponseti treatment in untreated children between the age of 1 and 6 years. In 260 feet, extensive soft tissue release was avoided in 94%. 83% only had casting and PAT. They changed casts every week. A survey from Zambia concluded that only 23% of the clubfoot children coming to district hospitals were suitable for Ponseti treatment. In central hospitals, the figure was 65% (De Rosa, Citation2012). This suggests a great need for many extensive surgeries in a country where there is a shortage of surgical capacity. In the report, the criteria for not being fit for Ponseti treatment were not mentioned, except for a short comment that in Zambia, in practice Ponseti was only used during the first year.
The standard treatment for neglected clubfoot has been extensive surgical intervention—which is technically demanding, is costly, and has a significant rate of complications even in the best hands (Penny Citation2005). The Ilizarow technique has been used for recurrent clubfoot and for neglected clubfoot. It is considered to be a salvage procedure in older children (Wallander et al. Citation1996). In our context, there is no Ilizarow equipment available or knowledge of how to use it. The technique is demanding, time consuming, and is associated with complications. There would be a need for reliable logistics and thorough teaching and follow-up if this technique were to be used in Ethiopia.
We used longer intervals between the casts than in the standard method. This may allow stretching of the soft tissues, which might be less elastic in older children. The manipulation and casting were performed every 2 weeks to allow remodeling and to hinder soft tissue edema. Since Spiegel got good results with a 1-week interval, this should be studied further. In our cases, the Ponseti method proved to be more effective in correcting deformities of the forefoot and midfoot than deformities of the hindfoot in the oldest group, as demonstrated by the need for a minor posterior release in 3 children (8, 9, and 10 years old; 4 feet). None of the feet required a medial or lateral release, or corrective bony procedure.
In cases of recurrence we used recasting, and we believe that one should be quick in doing that—with or without re-tenotomy of the Achilles tendon. If further surgical services are available, one should consider transfer of the tibialis anterior tendon to probably reduce later recurrences, especially if adequate orthoses cannot be found or will not be used because of poor compliance.
We believe that we achieved good results because the treatment was given by a skilled person with a proper understanding of the Ponseti method and commitment to the children. BA is an Ethiopian-trained orthopedic surgeon who has had special interest in clubfoot treatment. The presence of a counselor might also have been beneficial. The regular supply of casting material has also been essential. The latter is a common problem in many hospitals in LIC.
The study had some obvious limitations. The sample size was small, but considering the pathology being described this is a fairly large series. Even longer follow-up would have been ideal, but considering the difficulties in obtaining follow-up in LIC with high costs of transport (Young et al. Citation2013), we achieved fairly good long-term follow-up and a very good follow-up rate. We believe that our work at St. Luke Hospital in 2007–2010 is very encouraging and contributes useful information to the field of clubfoot treatment both in low- and high-income countries.
In conclusion, the Ponseti method can be used successfully to treat neglected clubfoot in older children than is traditionally recommended. If the treatment is done properly, it will significantly reduce the need for surgical intervention.
BA: idea, protocol, treatment, data collection, and writing. (His present working place is Orthop Dept, Black Lion Hospital, Unversity of Addis Ababa). PK idea and writing (who worked at St. Luke Catholic General Hospital, Black Lion Hospital, Unversity of Addis Ababa).
We thank Paul Saunderson and Sven Young for valuable comments and corrections.
No competing interests declared.
- Alves C, Escalda C, Fernandes P, Tavares D, Cassiano Neves M. Ponseti Method: Does age at the beginning of treatment make a difference? Clin Orthop 2009; (467): 1271–7
- Bor N, Coplan JA, Herzenberg JE. Ponseti treatment for idiopathic clubfoot:Minimum 5-year followup. Clin Orthop 2009; (467): 1263–70
- Cooper DM, Dietz FR. Treatment of idiopathic clubfoot: A thirty-year follow-up note. J Bone Joint Surg (Am) 1995; 77: 1477-89.
- De Rosa A, Norrish A. The need for early treatment of clubfeet in peripheral hospitals in sub-Saharan Africa: a survey of clubfoot management in Zambia. Trop Doctor 2012; 42 (2): 125-6.
- Dyer PJ, Davis N. The role of the Pirani scoring system in the management of club foot by the Ponseti method. J Bone Joint Surg (Br) 2006; 88: 1082-4.
- Lourenço AF, Morcuende JA. Correction of neglected idiopathic club foot by the Ponseti method. J Bone Joint Surg (Br) 2007; 89: 378-81.
- Morcuende JA, Dolan LA, Dietz FR, Ponseti IV. Radical reduction in the rate of extensive corrective surgery for clubfoot using the Ponseti method. Pediatrics 2004; 113; 376-80.
- Penny JN. The neglected clubfoot. Techniques in Orthopaedics, Vol. 20, No. 2, 2005.
- Pirani S. Pirani severity scoring. In: Clubfoot; Ponseti management (ed Staheli L). Global-HELP 2003: 22-3.
- Pirani S, Naddumba E, Mathias R, Konde-Lule J, Penny JN, Beyeza T, Mbonye B, Amone J, Franceschi F. Towards effective Ponseti clubfoot care: the Uganda Sustainable Clubfoot Care Project. Clin Orthop 2009; (467) (5): 1154-63.
- Ponseti IV. Treatment of congenital clubfoot. J Bone Joint Surg (Am) 1992; 74: 448-54.
- Spiegel DA, Shrestha OP, Sitoula P, Rajbhandary T, Bijukachhe B, Banskota AK. Ponseti method for untreated idiopathic clubfeet in Nepalese patients from 1 to 6 years of age. Clin Orthop 2009; (467) (5): 1164-70.
- Staheli L (Ed.) Ponseti management of clubfeet. Seattle: Global-HELP.org. 2003.
- Sætersdal C, Fevang JM, Fosse L, Engesæter LB. Good results with the Ponseti method: a multicenter study of 162 clubfeet followed for 2-5 years.Acta Orthop. 2012; 83 (3): 288-93
- Tindall AJ, Steinlechner CW, Lavy CB, Mannion S, Mkandawire N. Results of manipulation of idiopathic clubfoot deformity in Malawi by orthopaedic clinical officers using the Ponseti method: a realistic alternative for the developing world? J Pediatr Orthop 2005; 25 (5): 627-9.
- Verma A, Mehtani A, Sural S, Maini L, Gautam VK, Basran SS, Arora S. Management of idiopathic clubfoot in toddlers by Ponseti’s method. J Pediatr Orthop B 2012; 21 (1): 79-84.
- Wallander H, Hansson G, Tjernstrom B. Correction of persistent clubfoot deformities with the Ilizarov external fixator. Experience in 10 previously operated feet followed for 2-5 years. Acta Orthop Scand 1996; 67 (3): 283-7.
- Yagmurlu MF, Ermis MN, Akdeniz HE, Kesin E, Karakas ES. Ponseti management of clubfoot after walking age. Pediatr Int 2011; 53 (1): 85–9.
- Young S, Banza LN, Hallan G, Beniyasi F, Manda KG, Munthali BS, Dybvik E, Engesæter LB, Havelin LI. Complications after intramedullary nailing of femoral fractures in a low-income country. Acta Orthop 2013; 84 (5): 460-7.
- Zionts LE, Zhao G, Hitchcock K, et al. Has the rate of extensive surgery to treat idiopathic clubfoot declined in the United States? J Bone Joint Surg (Am) 2010; 92+: 882–9.