
Abstract
Background and purpose — Fractures of the lateral malleolus often require open reduction and internal fixation (ORIF). Despite uneventful fracture healing, many patients will suffer from long-term detriments after ORIF, such as local tenderness that requires hardware removal. In Sweden, there are 2 major fixation methods, either the AO method (plate and screws) or the Cedell method (cerclage wire and staple). The purpose of this study was to establish whether there is a difference in extraction frequency between the 2 methods.
Patients and methods — We performed a retrospective comparative study of all isolated fractures through the lateral malleolus that were operated at Skåne University Hospital, Sweden, during the period January 2007 to December 2010. 347 patients fulfilled the inclusion criteria (dislocated Weber B isolated fractures of the lateral malleolus) and were categorized according to fixation method. The numbers of reoperations, with preceding indication, were established from the charts. The median follow-up time was 59 (38–86) months after the primary surgery.
Results — 22% of the 110 patients treated with the AO method underwent a reoperation, as compared to 8% of the 237 patients treated with the Cedell method (p < 0.001). The median time to extraction was 16 (4–55) months.
Interpretation — Less implant removal is needed with the Cedell method than with the conventional AO method. This favors the use of the Cedell method in uncomplicated Weber B lateral ankle fractures, provided that other clinical parameters are comparable.
Ankle fractures are common, with increasing incidence (Kannus et al. 2002, CitationYang et al. 2010, Thur et al. 2012). If the fracture is dislocated, it is generally treated with open reduction and internal fixation (ORIF) (CitationCedell and Wiberg 1962, CitationMak et al. 1985, CitationOlerud et al. 1986, CitationMakwana et al. 2001). The limited soft tissue coverage of the lateral and medial malleolus makes the ankle susceptible to postoperative infection, skin necrosis, and local tenderness over the osteosynthesis material (CitationPonzer et al. 1999, CitationLash et al. 2002). Consequently, many patients need a reoperation at a later stage, the most common being extraction of the osteosynthesis material (CitationJacobsen et al. 1994, CitationBrown et al. 2001, CitationMinkowitz et al. 2007, Vos and Verhofstad 2013).
In Sweden, there are 2 major methods for operating an acute ankle fracture, the AO method using a plate and screw technique (Müller et al. 1991) and the Cedell method using cerclage wire and staples (CitationCedell and Wiberg 1962, Cedell 1967). Both fixation methods are well documented, and lead to fracture healing (Cedell 1967, CitationOlerud and Molander 1985, CitationAhl et al. 1986, 1987, 1993, CitationEckerwall and Persson 1993).
The AO technique is the method of choice for ankle fractures in most orthopedic centers throughout the world, although the Cedell method is also sufficiently stable for treatment of bimalleolar ankle fractures (CitationOlerud et al. 1986, CitationAhl et al. 1986, 1987, 1993, CitationEckerwall and Persson 1993). The choice of method is widely discussed among orthopedic surgeons in Sweden.
Provided that fracture healing and other clinical parameters are equivalent, the number of secondary surgical procedures is an objective outcome measure of the primary osteosynthesis. Every operative procedure involves risks and discomfort for the patient and also a recovery period. The financial burden is another important factor, as every surgical procedure means additional costs (CitationBöstman and Pihlajamäki 1996, CitationHanson et al. 2008,) We investigated whether there was a difference in the number of reoperations between the AO method and the Cedell method after dislocated lateral malleolar fractures.
Methods
Sampling and data collection
In this retrospective comparative study of surgically treated closed fractures of the lateral malleolus, all patients treated with ORIF at Skåne University Hospital in Malmö and Lund (SUS) between January 1, 2007 and December 31, 2010 were retrieved from the hospital database. The total group consisted of 534 patients with the International Code of Disease, revision 10 (ICD-10) diagnosis code S8260 (closed fracture of the lateral malleolus).
The following information was retrieved from the database: date of birth, sex, and date of surgery. No information was retrieved regarding comorbidity. In order to have comparable fractures, radiographs from all 534 patients were evaluated using our digital imaging archive. Radiographs were first classified preoperatively and after that, the peroperative and postoperative radiographs were checked.
Classification of ankle fractures was done using the AO/Weber classification
To avoid selection bias, where more unstable and comminuted fractures would possibly be operated with the AO technique, we included only patients with an isolated AO/Weber type-B fracture of the lateral malleolus. Thus, processus posterior, bimalleolar, trimalleolar, and comminuted fractures were excluded. All fractures above the lateral malleolus, described as proximal to the syndesmosis, AO/Weber C, were also excluded since they are not operated on with the Cedell method at Skåne University Hospital. Other techniques and combinations of the 2 methods were only used sporadically, and they were excluded in this material. Of the 534 patients, 347 met the inclusion criteria ().
Figure 1. Flow chart showing the numbers of patients treated with each method, exclusion criteria, and numbers of reoperations in each group
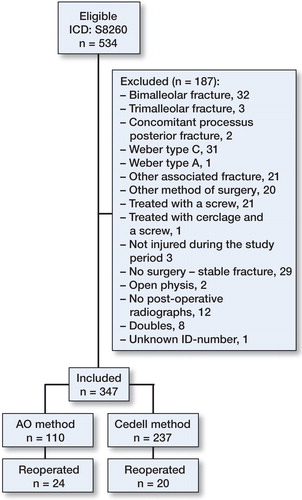
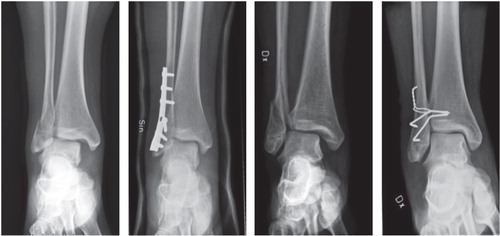
The patients were divided into 2 groups based on the fixation method: (1) the AO group, where patients were treated with a plate and screw fixation with or without trans-syndesmotic screw(s) according to AO principles (Müller et al. 1991); (2) the Cedell group, where patients were treated with cerclage wire on the distal fibula and/or staples between tibia and fibula (CitationCedell and Wiberg 1962, Cedell 1967) (). The surgical method was chosen by individual surgeons based on personal preferences. All patients were identified in the hospital database, to find the patients who had undergone another surgery on the same ankle. February 28, 2014 was defined as the deadline for reoperation. The surgical report and medical chart were studied in order to find out the indication for reoperation.
Figure 2. Typical fractures and treatment with the AO method (left panels) and the Cedell method (right panels).
Statistics
Differences between groups were evaluated using the chi-squared test. Student’s t-test was used to evaluate differences in age between groups. Any p-values < 0.05 were considered statistically significant. Statistical calculations were done using SPSS.
Ethics
The study was approved by the local ethics committee (registration number 2014/03).
Results
347 patients (177 of them men) were identified with an isolated lateral malleolar fracture, with a median age of 51 (19–92) years. 237 were treated with the Cedell method and 110 were treated with the AO method (). 44 patients underwent reoperation with extraction of the osteosynthesis material. Another 5 patients, 3 from the AO group and 2 from the Cedell group, were excluded from the comparison due to reoperations other than extractions. These operations included 3 arthroscopies, 1 arthrodesis, and 1 early reoperation due to postoperative incongruence (initially operated with the AO technique).
20 of the 237 patients in the Cedell group (8%) underwent a reoperation, as compared to 24 of the 110 patients in the AO group (22%) (p < 0.001). In the AO group, 6 patients were reoperated with a planned extraction of a trans-syndesmotic screw. Even when these 6 patients were excluded from the comparison, the statistical difference remained significant, with a reoperation rate of 19%.
There was no statistically significant difference between men and women. However, younger patients were more often treated with the Cedell method (median age 47 (19–92) years) than the AO method (median age 60 (19–89) years) (p < 0.001). The median age for reoperation was 34 (19–65) years in the Cedell group and 55 (19–77) years in the AO group (p < 0.01).
Excluding the 6 planned extractions of a trans-syndesmotic screw, the median time from primary osteosynthesis to hardware removal was 16 (4–55) months and there was no significant difference between the Cedell group and the AO group. The indication for reoperation varied, and some patients had several reasons for wanting a reoperation ().
The most frequent complaint in the Cedell group was local pain and tenderness on palpation (reported by 9 of 20 patients), followed by more diffuse strain-related pain in 7 patients. In the AO group, 10 patients reported mechanical issues with the osteosynthesis material, such as ulceration, chafe from socks, and local swelling while 11 patients reported strain-related pain. There were no postoperative infections requiring debridement.
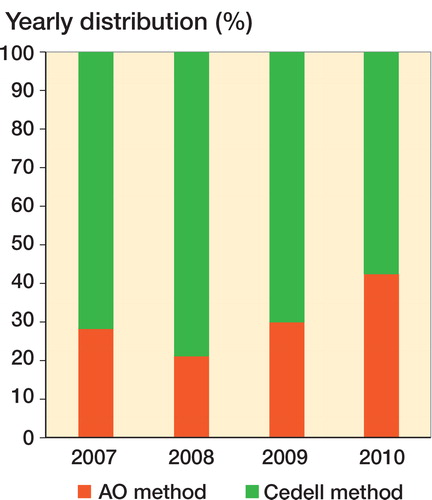
The Cedell method was still the most common method of fixation for lateral malleolar fractures in 2010, but in 4 years the relative use of the AO method had increased ().
Table 1. Indications for reoperation as noted in the patients’ journals. Some patients gave several reasons for hardware removal
Figure 3. Distribution of each surgical procedure.
Discussion
We found that the AO method leads to more extractions than the Cedell method after surgical treatment of dislocated fractures through the lateral malleolus. Our results have led to a change in treatment protocol at SUS University Hospital in Malmö and Lund, with the Cedell method now being recommended for surgical treatment of uncomplicated dislocated ankle fractures.
CitationBrown et al. (2001) found an osteosynthesis extraction rate of 24% in patients treated with the AO method for ankle fractures, which is similar to our findings (22%). We are not aware of any studies on the extraction rate after fixation with the Cedell method. Our results, with an extraction rate of only 8%, indicate that the Cedell method—including less osteosynthesis material—also leads to less mechanical issues.
Through the years, many studies have confirmed that the Cedell method is stable enough for this type of fracture (CitationOlerud and Molander 1985, CitationAhl et al. 1986, 1987). In the present study, with patients operated at Skåne University Hospital, the Cedell method was still the most common, but the use of the AO method increased during the study period—perhaps due the more widespread use of the AO method internationally. Considering the rates of reoperation for each method, we estimate that another 32 patients would have needed secondary surgery if the AO method had been used exclusively during the 4-year study period. The choice of method will of course have large economic consequences. Furthermore, the average cost of an AO implant is 50% higher than that of a Cedell implant (at Skåne University Hospital, as of December 9, 2013).
6 of 40 patients had their trans-syndesmotic screw extracted as a routine procedure (no staples were removed as a routine), contrary to the recommendations in several studies (CitationBrown et al. 2001, CitationHanson et al. 2008, Vos and Verhofstad 2013). Again, it should be pointed out that even when the patients who had their trans-syndesmotic screw removed according to the treatment plan were excluded from the comparison, the higher reoperation rate in the AO group remained statistically significant.
The patients treated with the AO method were generally older than the patients treated with the Cedell method. However, when looking at the reoperated patients, young age tended to increase the likelihood of reoperation. It can be speculated that younger patients have higher demands and are more likely to want their hardware removed than older patients. With this in mind, the lower reoperation rate in the Cedell group, despite younger age, further supports our main finding.
The time period January 2007 to December 2010 was chosen because all the data were reported electronically, the surgical procedures were unchanged during that time, the data were large enough to give statistical power, and the length of time from the first ORIF was adequate to allow sufficient time for reoperation.
It may be argued that the limited follow-up time (38–89 months) was a weakness of the study, because some patients were reoperated later than 38 months after the primary operation. However, we have no reason to believe that this influenced the results since the median time for reoperation was only 16 (4–55) months. None of the patients in the study underwent a reoperation later than the median follow-up time of 59 months, and only 4 patients were reoperated later than the shortest follow-up time of 38 months. Estimating that as many as 4 patients would be reoperated later and that all would be derived from the Cedell group, which is unlikely, there would still be a statistically significant difference between the 2 groups, with fewer reoperations in the Cedell group.
As far as we know, this is the first study to compare reoperation frequency between the 2 operation techniques for this this type of fracture. In the future, it would be interesting to conduct a prospective randomized study that examines differences in clinical scores and complications between the 2 methods. Furthermore, it would be interesting to determine whether the extraction of the osteosynthesis material satisfies the expectations of the patient, or whether there are explanations for pain and discomfort other than mechanical issues.
In conclusion, provided that other clinical parameters are comparable, the lower extraction rate favors the Cedell method rather than the AO method when treating uncomplicated Weber type-B lateral ankle fractures.
CJT designed the study and SSB was responsible for data collection and analysis of radiographs. Statistical evaluation and writing of the manuscript were done by both authors together.
No competing interests declared. The study was funded by the Medical Faculty of Lund University.
- Ahl T, Dalen N, Holmberg S, Selvik G. Early weight bearing of malleolar fractures. Acta Orthop Scand 1986; 57(6): 526-9.
- Ahl T, Dalen N, Holmberg S, Selvik G. early weight bearing of displaced ankle fractures. Acta Orthop Scand 1987; 58(5): 535-8.
- Ahl T, Dalen N, Lundberg A, Bylund C. Early mobilization of operated on ankle fractures. Prospective,controlled study of 40 bimalleolar cases.Acta OrthopScand 1993; 64(1): 95-9.
- Brown OL, Dirschl DR, Obremskey WT. Incidence of hardware-related pain and its effect on functional outcomes after open reduction and internal fixation of ankle fractures. J Orthop Trauma 2001; 15(4): 271-4.
- Böstman O, Pihlajamäki H. Routine implant removal after fracture surgery: a potentially reducible consumer of hospital resources in trauma units. J Traum 1996; 41(5): 846-9.
- Cedell CA, Wiberg G. Treatment of eversion-supination fracture of the ankle (2d degree). Acta Chir Scand 1962; 124: 41-44.
- Cedell CA. Supination-outward rotation injuries of the ankle. A clinical and roentgenological study with special reference to the operative treatment. Acta Orthop Scand 1967: Suppl 110: 3.
- Eckerwall G, Persson BM. Fracture of the lateral malleolus: Comparison of 2 fixation methods in cadavers. Acta Orthop Scand 1993; 64(5): 595-7.
- Hanson B, van der Werken C, Stengel D. Surgeons’ beliefs and perceptions about removal of orthopaedic implants. BMC Musculoskelet Disord 2008; 9: 73.
- Jacobsen S, Honnens de Lichtenberg M, Jensen CM, Torholm C. Removal of internal fixation--the effect on patients’ complaints: a study of 66 cases of removal of internal fixation after malleolar fractures. Foot Ankle Int 1994; 15(4): 170-1.
- Kannus P, Palvanen M, Niemi S, Parkkari J, Järvinen M. Increasing number and incidence of low-trauma ankle fractures in elderly people: finnish statistics during 1970–2000 and projections for the future. Bone 2002; 31(3): 430-3.
- Mak K, Chan K, Leung P. Ankle fracture treated with the AO principle—an experience with 116 cases. Injury 1985; 16(4): 265-72.
- Lash N, Horne G, Fielden J, Devane P. Ankle fractures: functional and lifestyle outcomes at 2 years. ANZ J Surg 2002; 72(10): 724-30.
- Makwana NK, Bhowal B, Harper WM, Hui AW. Conservative versus operative treatment for displaced ankle fractures in patients over 55 years of age. A prospective, randomised study. J Bone Joint Surg Br 2001; 83(4): 525-9.
- Minkowitz RB, Bhadsavle S, Walsh M, Egol KA. Removal of painful orthopaedic implants after fracture union. J Bone Joint Surg Am 2007; 89(9): 1906-12.
- Müller ME, Perren SM, Allgöwer M. Manual of internal fixation: techniques recommended by the AO-ASIF group: Springer; 1991.
- Olerud C, Molander H. Surgical treatment of ankle fractures. A comparison of 2 osteosynthesis technics. Lakartidningen 1985; 82(40): 3378-9.
- Olerud C, Molander H, Olsson T, Hagstedt B. Ankle fractures treated with non-rigid internal fixation. Injury 1986; 17(1): 23-7.
- Ponzer S, Nasell H, Bergman B, Tornkvist H. Functional outcome and quality of life in patients with Type B ankle fractures: a two-year follow-up study. J Ortoph Trauma 1999; 13(5): 363-8.
- Thur CK, Edgren G, Jansson K-Å, Wretenberg P. Epidemiology of adult ankle fractures in Sweden between 1987 and 2004. Acta Orthop 2012; 83(3): 276-81.
- Vos DI, Verhofstad MHJ. Indications for implant removal after fracture healing: a review of the literature. Eur J Trauma Emerg Surg 2013; 39(4): 327-37.
- Yang NP, Chan CL, Yu IL, Lee CY, Chou P. Estimated prevalence of orthopaedic fractures in Taiwan--A cross-sectional study based on nationwide insurance data. Injury 2010; 41(12): 1266-72.