
Sir–With great interest we read the article entitled “Cross sectional imaging of metal-on-metal hip arthroplasties. Can we substitute MARS MRI with CT?” (CitationRobinson et al. 2014). We believe that the comparison between MARS-MR and CT and the conclusions that are drawn by this comparison do not consider the CT developments over the last few years, especially those that deal with metal artefacts.
First, the image quality of the provided CT-images is poor and not representative for a proper comparison between current state-of-the-art MRI and CT. Without quantifying the presented image quality parameters, it can be easily observed that standard noise values are high and contrast-to-noise-ratio (CNR) is poor. Besides the poor image quality, the CT images presented in the article seem not to be subject to dedicated metal artefact reduction. Moreover, the information provided for the CT acquisitions, in stark contrast to that provided for MR acquisitions, lack details: the only scan-parameter mentioned in the article is the use of a 64-slice CT scanner and the use of metal artefact reduction (MAR). Important variables in CT imaging regarding metal hip prosthesis were not mentioned at all. This lack of detail regarding the CT acquisition precludes any attempt at reproducing the results presented by Robinson and colleagues.
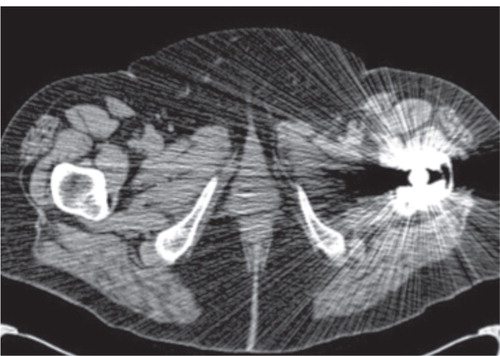
Second, no attention is given to the drastic improvement of CNR by partial, or even full iterative reconstruction techniques compared with the formerly used Filtered Back Projection (FBP). For comparison, we provide full iterative axial images with dedicated orthopedic metal artefact reduction from our institute () for comparison next to the article’s CT images () of bilateral hip prostheses including a large head metal-on-metal (MOM) hip prosthesis.
Figure 2. Images in current clinical practice at the same location. Axial CT image, 256-slice CT scanner, soft tissue window width and window level (40 400). Model-based iterative reconstruction with O-MAR at level of the prosthetic stem post-processing techniques are applied.
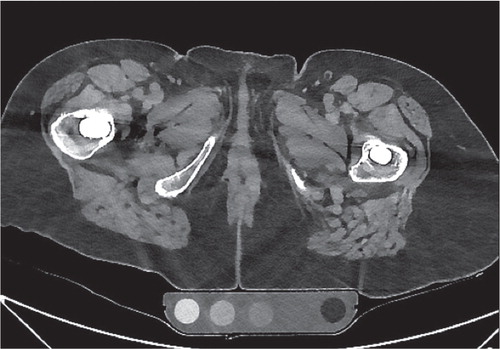
Figure 1. Image used in CitationRobinson et al. 2014. Axial CT image, 64 slice CT scanner, at the level of the prosthetic stem.
The use of up-to-date model-based iterative reconstruction techniques allows significant dose reduction while maintaining and even increasing image quality. In addition reconstructions with the use of state-of-the-art dedicated orthopedic metal artefact reduction techniques can be applied. In favour of CT Nam et al. (2014) recently mentioned the additional value in addressing the inclination and anteversion of the prosthesis components (Nam et al. 2014). In addition CT shows potential to estimate bone stock in the acetabulum which is of importance in estimating bone stock prior to revision surgery. (Boomsma et al., unpublished observations).
Finally, on the matter on modality choice, in a recent blinded prospective study a validation of USS is made and compared to MARS MRI in patients with MOM hips (CitationSiddiqui et al. 2014). A poor agreement was found between these modalities for the detection of pseudotumors, muscle atrophy, and joint effusion. USS had a poor sensitivity for pseudotumors, detecting only two-thirds of lesions. The choice of CT in our institute was based on our first study in which we also investigated the additional value of MR without MARS on detecting capsular reactions. In this study all positive CT scans were additionally scanned by MR, as well as all symptomatic patients. No additional pathology was found in our population by MR over CT (CitationBosker et al. 2012).
Sir–We thank you for your response to our paper ‘Cross sectional imaging of metal-on-metal hip arthroplasties. Can we substitute MARS MRI with CT?’ (CitationRobinson et al. 2014). We would like to acknowledge the comments of Wellenberg et al. and agree that the CT protocol used does not represent the latest developments in metal artefact reduction for CT over the last few years. Alternatively, we demonstrate the merits of using technology which is widely available to centres across the UK. With over 67,000 hips implanted in the UK alone (National Joint Registry 2014), the need for follow-up is a nationwide problem and not limited to isolated centres. The protocol that we used on the patients in this study is a low dose protocol that was advocated to look at prosthesis position. We know that this is used by many centres who do not necessarily have a multi detector CT or the ability to perform the newer MARS CT or dual energy techniques. For centres across Europe that may not be able to access MRI scanners then there was a question if these low dose protocols can be used to look for the features essential for the orthopaedic team to know in managing this set of patients.
Similarly, we also acknowledge that this study does not illustrate the latest progress in MRI with MAVRIC (CitationHayter et al. 2011) and SEMAC sequences (CitationSutter et al. 2012). This is a continually evolving field in which we have illustrated the merits of technology available in a typical UK centre at one point in time. We hope continued debate and interest in improving metal artefact on images will fuel further improvements in patient care.
- Bosker BH, Ettema HB, Boomsma MF, Kollen BJ, Maas M, Verheyen CC. High incidence of pseudotumour formation after large-diameter metal-on-metal total hip replacement: a prospective cohort study. J Bone Joint Surg (Br) 2012; 94 (6): 755–61.
- Hayter CL, Koff MF, Shah P, Koch KM, Miller TT, Potter HG. MRI after arthroplasty: comparison of MAVRIC and conventional fast spin-echo techniques. AJR Am J Roentgenol 2011; 197: W405-11.
- Nam D, Barrack RL, Potter HG. What are the advantages and disadvantages of imaging modalities to diagnose wear-related corrosion problems?. Clin Orthop 2014. [ahead of print]
- National Joint Registry: 11th annual report 2014 [Online] [Cited 14 January 2015] Available from: http://www.njrreports.org.uk/Portals/0/PDFdownloads/NJR%2011th%20Annual%20Report%202014.pdf
- Robinson E, Henckel J, Sabah S, Satchithananda K, Skinner J, and Hart A. Cross-sectional imaging of metal-on-metal hip arthroplasties: can we substitute MARS MRI with CT? Acta Orthop 2014; 85(6): 557-584
- Siddiqui IA, Sabah SA, Satchithananda K, Lim AK, Cro S, Henckel J, Skinner JA, Hart AJ. A comparison of the diagnostic accuracy of MARS MRI and ultrasound of the painful metal-on-metal hip arthroplasty. Acta Orthop 2014; 85(4): 375-82.
- Sutter R, Ulbrich EJ, Jellus V, Nittka M, Pfirrmann CW. Reduction of metal artifacts in patients with total hip arthroplasty with slice-encoding metal artifact correction and view-angle tilting MR imaging. Radiology 2012; 265: 204–14.