Abstract
Coronary arterial obstruction associated with congenital aortic valve disease is rare in childhood, and has not been reported in adult. Here we reported a 49-year-old healthy woman with hypoplastic left coronary cusp resulting in myocardial ischemia in the territory of left main coronary artery.
A 49-year–old healthy woman presented with incidental finding of a diastolic murmur during routine medical check-up. The chest X-ray and resting electrocardiography were normal. Transthoracic echocardiography showed satisfactory left ventricular systolic function but severe aortic regurgitation. Subsequent trans-esophageal echocardiography revealed tricuspid aortic valve structure with hypoplastic left coronary cusp (). Aortic root angiogram revealed a hypoplastic left coronary cusp with dynamic obstruction to the left main coronary ostium (). In fact, the left coronary ostium cannot be cannulated during cardiac catheterization. Selective right coronary angiography, however, showed normal right coronary artery with retrograde filling of the left anterior descending coronary artery and circumflex artery up to the proximal left main coronary artery (). Subsequently, thallium scan showed reversible perfusion abnormalities in extensive area of the left anterior descending coronary artery and circumflex artery territories. Aortic valve replacement was offered as definite treatment for both severe aortic regurgitation and myocardial ischemia. However, the patient refused, as she was rather asymptomatic. Coronary arterial obstruction associated with congenital aortic valve disease is rare in childhood, and has not been reported in adult.
Figure 1. Trans-esophageal echocardiography at short axis view of the basal structure (58° at mid-esophagus). The hypoplastic left coronary cusp (arrows) fails to co-apt during the diastole resulted in aortic regurgitation. LA, left atrium; N, non-coronary cusp; R, right coronary cusp; RVO, right ventricular outflow.
Figure 2. Aortic root angiogram reveals a membrane-like structure partially occluding the left coronary ostium (arrows).
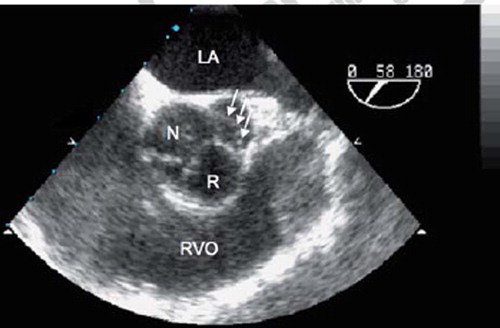
Figure 3. Selective right coronary angiogram reveals normal right coronary artery (RCA) with retrograde filling of the left circumflex artery (LCX) and up to ostium of the left main coronary artery (LMCA).
Declaration of interest: The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.