
ABSTRACT
Objective: To establish the impact of a gaze-based assistive technology (AT) intervention on activity repertoire, autonomous use, and goal attainment in children with severe physical impairments, and to examine parents’ satisfaction with the gaze-based AT and with services related to the gaze-based AT intervention. Methods: Non-experimental multiple case study with before, after, and follow-up design. Ten children with severe physical impairments without speaking ability (aged 1–15 years) participated in gaze-based AT intervention for 9–10 months, during which period the gaze-based AT was implemented in daily activities. Results: Repertoire of computer activities increased for seven children. All children had sustained usage of gaze-based AT in daily activities at follow-up, all had attained goals, and parents’ satisfaction with the AT and with services was high. Discussion: The gaze-based AT intervention was effective in guiding parents and teachers to continue supporting the children to perform activities with the AT after the intervention program.
Introduction
Using computers as assistive technology (AT) has been found to be an important intervention for children with profound impairments since it can reduce participation restrictions and activity limitations in childhood activities,Citation1,Citation2 especially in the areas of play, education, and communication.Citation3 Cerebral palsy is the most common cause of physical impairments in children, and the prevalence is two per 1000 live births.Citation4 Consequently, children with severe impairments represent a small group among the children with cerebral palsy. Only about one-third of these children have a severe motor impairmentCitation5 and about 25% are nonverbal .Citation6,Citation7 It is known that children with severe physical impairments, without speech, become involved in fewer activities with less diversity, and their activities are most often related to the home.Citation8,Citation9 They tend to have limited opportunities for social interaction.Citation10 Any intervention that will support these children to become active, spend time in a variety of activities, and give them opportunities to explore activities may support the children’s development and therefore needs to be prioritized. An AT has the purpose of increasing the repertoire of activities a person can perform independently or with greater ease,Citation11 which is why AT ought to be an effective intervention for this child group.
In accordance with the well-known definition by the International Organization for Standardization,Citation12 AT can be seen as an assistive product that is used to prevent activity limitations or participation restrictions. Controlling a computer with eye gaze, i.e., a gaze-based AT, may be the only way to operate a computer for children who have such severe physical impairments that they cannot fully control any other body movements than their gaze. Gaze-based AT has the potential to enable these children to perform childhood activities, such as to play and to interact with others. However, there is a dearth of studies investigating this subject area. Only a few case studies have been published concerning children with severe physical impairments and the use of gaze-based AT for daily activities.Citation13–Citation16 For children with profound impairments, user trials have found gaze-based AT to be suitable for activities such as playing music and gamesCitation13,Citation15 and making drawings.Citation17 For example, a child with severe motor impairment could use a gaze-based AT in primary school for music and story activities.Citation14 In a case studyCitation16 gaze-based AT was used for literacy training and for communication among the children involved (aged 7 and 9 years). Activity repertoire or fulfillment of goals for gaze-based AT use was not reported. However, at the 3 months follow-up after provision, it was not used to its full potential in daily life, due to the lack of support in implementing the gaze-based AT in daily activities. The need of support, guidance, and training in adapting the AT to the child’s needs over time, as well as the need of ongoing technical support, has been stressed in research as facilitating factors of service delivery to promote the implementation and use of AT in daily activities.Citation16,Citation18–Citation20
An AT intervention consists of having access to the AT and to services provided by practitioners to integrate and promote the use of the AT in daily life.Citation21 Research has reported that not all AT provided for children with impairments is used in daily life.Citation22,Citation23 It has been pointed out that long-term services are often needed to promote the continued use of AT over time, for example for communication, for children with profound impairments.Citation24,Citation25 The use of AT for communication by children with severe physical impairments has been described as an evolving process over time, with high motivation and use during the initial months, followed by reduced motivation and usage between 3 and 6 months after provision of the AT.Citation25
According to the Human Activity Assistive Technology (HAAT) model, the AT usage will be determined by the dynamic interaction between the human, the activity, and the AT within the specific environment of use. Each of these components has the potential to enable or disable performance with the AT.Citation26 AT usability can be understood as the product of the interplay between these components,Citation27 and usability is defined as the degree to which a user can use an AT to fulfill goals with effectiveness (e.g., completeness of specified goals with AT use), efficiency (e.g., time and effort during performance), and with satisfaction when using the AT in a specific context of use.Citation28
The activity is described as the fundamental element in the HAAT model,Citation26 and in line with this model the present study highlights the relevance of the activity to the person as the paramount and performing activities as the overall goal of using the AT. Thus, the use of the AT, activity repertoire as well as achievement of goals for AT use is important outcomes to measure. AT usage is commonly measured based on the type of activities, frequency, and duration of AT use, in addition to the specific contexts in which it is used.Citation27,Citation29 Continued use of an AT can be predicted by the AT usability, as the AT needs to be usable to have continued use over time.Citation27 Furthermore, a usable AT is a prerequisite to be use-worthy in daily life.Citation11 In accordance with research in other areas of AT,Citation30 usage needs to be measured for a long period of time to capture the longitudinal usability of gaze-based AT.
Most research concerning the use of gaze-based AT for daily activities has been conducted on adults with severe physical impairments, and shows usage for activities such as communication and internet surfing.Citation31–Citation33 These survey studies focused on communication activities, quality of life, and satisfaction with the gaze-based AT mostly with experienced users. In research on children, case studies indicate that gaze-based AT has the potential to support children to perform activities.Citation13,Citation14,Citation16,Citation17 In a longitudinal study by Borgestig et al.,Citation34 the efficiency of gaze-based AT for children with severe physical impairments without speech was measured in a standardized environment. They found eye gaze performance to improve over time with respect to time-on-task and accuracy after long-term practices. In addition, environmental aspects that have an impact on the use of gaze-based AT for children with physical impairments have been investigated.Citation16 However, research that evaluates activity repertoire and the use of gaze-based AT in daily activities over time for children with profound impairments is lacking.Citation15,Citation35 This may be because gaze-based AT is an underutilized AT for children with profound impairments, and until recently, it has been an expensive AT. Researchers have also emphasized the need to investigate what support is required to support its use in daily activities over time.Citation35 The aim of the present study was therefore to establish the impact of a gaze-based AT intervention on activity repertoire, autonomous usage, and goal attainment in children with severe physical impairments. In addition, parents’ satisfaction with the gaze-based AT and with services related to the gaze-based AT intervention was examined.
Materials and methods
This nonexperimental multiple case study used a before, after, and follow-up designCitation36 including 10 children with severe physical impairments without speaking abilities. The data were collected daily during a 14-day period at baseline (A), post-intervention (B1), and at follow-up (B2) for the computer-use variables (activity repertoire, duration of use, percentage of days with use, and number of performed activities). Intervention lasted for 9–10 months, and follow-up was conducted 5–10 months after withdrawal of the services related to the gaze-based AT intervention, as shown in .
Figure 1. Format of gaze-based AT intervention, and time points for data collection (in months), DI (during intervention), B1 (post-intervention), and B2 (follow-up). As expected, the children were provided with local services between B1 and B2, 0–5 occasions to parents (mean 1.9), 1–10 occasions to teachers (mean 3.8).
Study context
A regional pediatric rehabilitation center (RPC) in Sweden has a multi-professional communication (MPC) team specializing in the use of AT, such as gaze-based AT. Local services, such as local pediatric rehabilitation centers, can refer children up to 18 years with physical impairments and complex communication needs to receive support in assessment, training, and adaptation of gaze-based AT usage and to take part in the specific gaze-based AT intervention under study, with the purpose of integrating the gaze-based AT in the children’s everyday life. The MPC team consisted of an occupational therapist, speech and language pathologist, special education teacher, and IT support person. All were well-trained in the adaptation and usage of gaze-based AT. A pediatric neurologist was involved as a medical expert. The speech and language pathologist and the special education teacher both had more than 10 years of experience in servicing the target group.
Participants
A total of 10 children were referred to the regional pediatric center in 2010–2013 with requests for support of the children’s use of gaze-based AT. Inclusion criteria for the current study were: (a) children with severe physical impairments without speaking ability, (b) up to 18 years, (c) with access to gaze-based AT, and (d) whose parents and teacher agreed to participate in the gaze-based AT intervention and in data collection. All parents of the 10 children consented to participation, and all children were recruited. One teacher of each child was invited to participate and all consented to participation. Participating children are described in . All children communicated with facial expressions and eye-pointing (e.g., point to show interests or to request items, some could express yes/no by for example look up/down) as no one could speak or communicate with sign language. The children had access to low-tech communication boards (n = 4) or single pictures (n = 4) for communication, but they were reported to be seldom used. Some children also had additional impairments, such as unspecified cognitive impairments (five children), strabismus (two children), and epilepsy (four children). Among the seven children with unknown cognitive level or with unspecified cognitive impairment, three could clearly express yes/no by eye-pointing (children 3, 5, 8), three were unclear in this (children 4, 6, 10) whereas one child could not (child 7). The teacher to this child (7) used real objects as symbols and the child was in the beginning of learning to use pictures for communication. The other children used pictures for communication.
Table 1. Background variables for participating children.
Seven children were provided with a gaze-based AT at baseline. Three children already had access to a gaze-based AT and needed support to start to use it. Two had had other computer access methods at baseline but were assessed not to be able to develop more with the hand switch (child 10) or the head-controlled mouse (child 5) due to their profound motor impairment. The mean age of the parents was 40.7 years (SD 4.9). Parents to three children had another native language than Swedish but all could understand and speak some Swedish. However, interpreters were used during the whole process for these three settings. Teachers had between nine and 39 years of experience in the profession (mean 20, SD 9) (eight women, two men). The children are identified in the results with numbers (1) to (10) or fictional names.
The gaze-based AT intervention
The gaze-based AT intervention consisted of two parts: having access to gaze-based AT and having access to the services from the MPC team. When the gaze-based AT intervention ended (after 9–10 months), the services of the MPC team were terminated. The children then continued to have full access to the gaze-based AT in their daily lives.
The gaze-based AT
The children had access to the gaze-based AT Tobii C12 (nine children) or P10 (one child) (built-in gaze devices).37 Both devices are portable and were mounted on a floor stand, table stand, or on the wheelchair. The gaze-based AT was transported with the child between home and school. During the intervention program, the software in the gaze-based AT was adapted to include dynamic communication pages with pictures, symbols, and speech output, to meet each child’s individual needs at home and/or at school. Due to different ages and cognitive levels, pages were developed for play and leisure, for educational tasks, and to communicate. The number of pictures on a page varied between 3 and 25, with a variation of between 60 and 800 pictures in total when the children ended the intervention program (for an example of a page, see ).
Figure 2. A personalized first page in the gaze-based AT, from which the child can select a picture with eye gaze to reach more pages with pictures and activities.

The services
The services were based upon the same research-based key elements (increase knowledge among teachers, collaboration between key persons, child’s preferences for usage, and goal setting), format (course day and planning meeting), and modular content areas, as in a previous study by Borgestig, Falkmer, and Hemmingsson.Citation38 The measures used for the evaluation of computer usage were also tested in that study (e.g., computer use diaries, goal attainment with computer use). Due to the children’s profound impairments, the current study added individual support.
The services were provided by the MPC team over a period of 14 days, spread across 9–10 months. The purpose of the services was to optimize the implementation and use of gaze-based AT in daily activities. The current study involved parents and all key persons (i.e., all that played a role in the child’s use of gaze-based AT in daily life) in joint goal-setting, planning, and jointly reviewing the progress of the use of gaze-based AT at home and at school. The intervention program was provided in groups of two to five children at the same time. Services provided on a group level were course days for parents, teachers, and children, respectively. This was combined with individual meetings and support for each child. gives an overview of the three steps included in the gaze-based AT intervention. All children, regardless of earlier AT experiences, were provided with the same service in the intervention program. Step 1 started with an introduction lasting two days, which consisted of education (how to create pages, make adaptations to the software, and handle the gaze-based AT) for stakeholders (e.g., parents, teachers, and assistants). Furthermore, the introduction included initial adaptation of the software in the gaze-based AT, and training for the child in how to gaze control and use the AT. For the three children that already had access to gaze-based AT at baseline the software was revised to match their abilities and needs. At the planning meeting (step 1) each child’s prerequisites (e.g., gaze control skills, communication) and motivation for activities were on the agenda. Furthermore, prioritized participatory problems were identified (e.g., not being able to comment or answer questions during circle time in school), goals for gaze-based AT usage in daily activities were collaboratively formulated, and gaze-based AT strategies developed. After the planning meeting a goal planning document was established by the MPC team to ensure a shared focus on the goals. The course days for teachers and parents (parents meeting parents; teachers meeting teachers) (steps 2 and 3) involved the exchange of experiences of the children’s gaze-based AT use in daily activities at home/in school, demonstration of pages in the software for different activities by the MPC team, and further adaptation of the gaze-based AT for each child’s needs. During the course day for children (step 3), children played games and music together by using their gaze-based AT to gain positive experiences from the use and to practice how to use the gaze-based AT. The individual planning and follow-up meetings (steps 1–3) were provided for all stakeholders for each child (parents, teacher, assistants, local services such as members from the AT center and the local pediatric rehabilitation team, in total 5–14 individuals for each child). During the follow-up meetings, the goals were evaluated, and strategies adapted if needed (steps 2–3). In all steps, individual support was provided when needed, for five occasions for each child. It consisted of home or/and school visits by members of the MPC team to provide direct or indirect support to the child, parents and/or teacher, and assistants, such as in adaptation of the software, in the usage of gaze-based AT in daily activities, and support with gaze control.
Outcome measurements
Computer usage diaries
Through direct observation by parents, teachers, or assistants, usage of gaze-based AT was measured in a computer use diary:Citation38 one concerning the daily usage in school and the other one the daily usage at home. Each day the following were noted: 1) type of computer activities per day noted by one or more of the predefined activities, with the possibility to add activities. For example, in school there were 10 predefined activities (e.g., to make presentations or to talk with someone), and 2) duration of use for each activity per day (in minutes) with individual responses estimated after each activity throughout the day.
Goal attainment scaling
To formulate and evaluate the goals of meaningful use in school and at home with gaze-based AT, the Goal Attainment Scaling, GAS,Citation39 was used. The instrument has a five-point scale, from −2 (starting level) to +2 (more than expected) with zero as the expected level of success. Each goal is described with five levels including somewhat more (+1) and somewhat less (−1) than expected, and much more (+2) and much less (−2) than expected in relation to the expected outcome (0).Citation39 The instruction was to set −2 as the current individual level at baseline. GAS has shown good responsiveness in detecting clinically relevant changeCitation40,Citation41 and content validity according to determining goals that represent important progress.Citation42
The Quebec User Evaluation of Satisfaction with Assistive Technology (QUEST 2.0)
Quest 2.043 was used to evaluate parents’ satisfaction with the gaze-based AT as an assistive device and with the service provided related to the gaze-based AT. The instrument included eight satisfaction items concerning the device (e.g., ease in adjusting, easy to use) and four items concerning the service (e.g., professional services, follow-up services, repairs and servicing). The instrument includes the same question for each item: “How satisfied are you with..?” (e.g., professional services). All items had five graduations (1–5) from “Not satisfied at all” to “Very satisfied”. Mean scores were calculated for rated items corresponding to the device scale, the service scale, and all items together (Total scale). Higher values represent higher satisfaction. The instrument has shown good test-retest stability (0.82–0.91), good interval consistency, and validity.Citation43
Procedure
shows the time points and measurements for data collection. At baseline, the research group met the parents at the RPC and they were provided with information about the study. During baseline, parents and teachers observed and documented the child’s use of the computer as AT (gaze-based AT or, e.g., head-controlled mouse or switch) each day for a 14-day period in the home diary and school diary. The period that followed after baseline children participated in gaze-based AT intervention together with their parents and teachers. Eight children used their gaze-based AT at home and at school, and two children either at school (7) or at home (1).
Table 2. Instruments for data collection.
During the intervention, the GAS was administered by the MPC team at the planning meeting, and subsequently the research team checked goals so that they were measurable and relevant. The MPC team was well-trained in using GAS collaboratively together with other parents and teachers since several years before start of this study.
At the time point “during intervention” (DI), computer diaries were posted to parents and teachers. They observed and noted the children’s use of gaze-based AT each day during the 14-day period in the home diary (14 days) and school diary (10 days). All were contacted by phone so parents and teachers were able to ask questions about the diaries. Goals were evaluated at the first and second follow-up meeting as part of the gaze-based AT intervention. The intervention lasted between 9 and 10 months for all.
At post-intervention and at follow-up, the computer diary and Quest 2.0 were posted to parents, and the computer diary to teachers. Computer diaries were again filled in each day during a 14-day period and Quest 2.0 was completed by parents. At follow-up, parents were instructed to think of the period between post-intervention and follow-up when rating three of the items (professional service, follow-up, repairs and servicing) in the service dimension in Quest 2.0.
Medical records showed hospital stays with operations, or sickness periods for two children (2, 5) which caused them to be absent from school/preschool for at least 2 months during the intervention period. One of these children developed a severe form of therapy-resistant epilepsy during the study (2). Two children changed school (3) or assistants (2, 3) during the intervention. No concurrent interventions, such as medical treatments or other professional services that may have a potential positive influence on children’s use of gaze-based AT, were monitored during the study.
Data analyses
The repertoire of activities was calculated by counting all activities, documented in home and school diaries, for each time point. The variables in computer diaries were calculated in each phase (each 14-day period), for home and school together, as follows: (a) number of activities/day, (b) duration of usage (min/day), and (c) percentage of user days (%), referring to the number of days with usage from the total number of days noted. In addition, the percentage of user days (%) was calculated for each activity in each diary (school and home diaries, respectively) for baseline and follow-up. Diaries were returned with 25 missing days in total in both the school and home diaries (B1: 18 days, B2: 7 days) out of 420 days in the diaries. Three new activities were filled in as individual responses under “type of activities” and these were included as separate activities (to choose activities, to participate in circle time in school, to look at the schedule to be informed of the day’s activities).
To determine if there were any improvements between phases (A, B1, B2) in the computer use variables, the data were presented as graphs (number of activities/day, duration, % of user days) to be visually inspected regarding change of data pattern across phases, such as change between phases and trends within phases.
Formulated goals with GAS were evaluated for each child, and categorized to describe their content. Concerning Quest 2.0, median values and inter-quartile range were calculated on a group level for the device scale, service scale, and the total scale. To examine on an item level in Quest 2.044 was parents’ scoring for each item grouped in being satisfied (4 “quite satisfied” and 5 “very satisfied”), and being less satisfied (1 “not satisfied at all”, 2 “not very satisfied”, and 3 “more or less satisfied”).
Ethical considerations
On behalf of the children, written informed consent was obtained from both parents of each child participating in the study. The parents and teachers were informed that they could withdraw from the study at any time, without affecting the services given to them or the children in the gaze-based AT intervention. The study received ethical approval from the Regional Ethical Review Board in Uppsala, Sweden (2010/316).
Results
Repertoire of computer activities in home and in school
As shown in , all 10 children performed computer activities at home and/or in school at follow-up, whereas only five of the children (5, 6, 8–10) did so at baseline. Seven children increased the repertoire of activities from baseline to follow-up. On a group level, the mean value increased from baseline (mean = 1.8) to follow-up (mean = 3.8).
Table 3. Computer activities children performed in home and at school.
At follow-up, the computer activity most children performed was to talk with someone, in school (3–4, 6–10), as well as at home (2, 4–6, 9–10). However, it was only for the two oldest children (9–10) that this was the most frequently performed activity across the days (21–71%) at home, whereas the six youngest children (1–6) most frequently performed activities such as playing games, watching photos, or listening to music across the days at home (14–71%).
Change in number of computer activities and duration of use
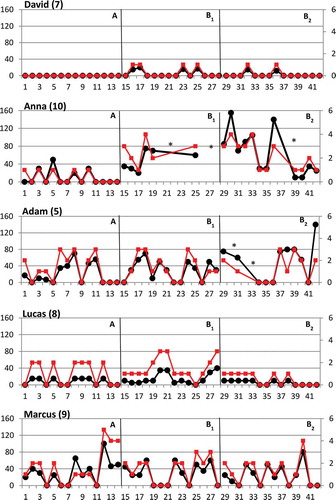
and show graphic presentations of data on the number of performed computer activities per day and duration of computer activities (min/day) over time. Visual inspection of the data show an overall positive effect post-intervention (B1) that was maintained at follow-up (B2) for Emma, Jacob, Daniel, Max, Isaac, David, and Anna in both the number of performed activities and in duration of use (see and ). Six of these children’s data show a distinct positive change over time, whereas David’s data show a pattern with a small positive change over time. On the other hand, as shown in , the data of Adam, Lucas, and Marcus show no effect at B2, although one of these children, Lucas, had a small positive effect at B1 in both number of activities and duration of use. When inspecting the trends within phases, increasing trends were found within B1 for both duration of use and number of computer activities for three children (Emma, Jacob, Anna). Within phase B2, decreasing trends were found in number of computer activities (Emma, Jacob, Daniel, Anna) and in duration of use (Jacob, Max, Anna).
Figure 3a. Five of the children with positive change from baseline (A) to post-intervention (B1) and with maintained effect at follow-up (B2), in duration of computer use (black line) and in number of computer activities (red line). Missing days: # due to broken gaze-based AT, * due to that the child was sick.
Primary Y-axis: minutes; secondary Y-axis: number of activities. Black line: duration of computer use. Red line: number of computer activities.
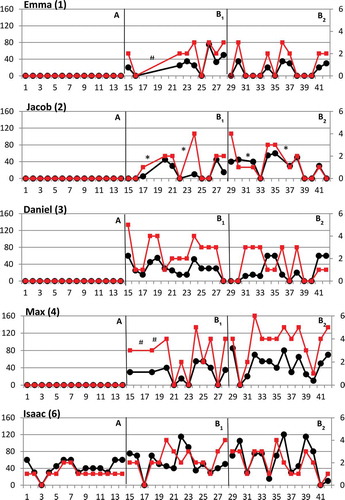
Figure 3b. Two of the children with positive change from baseline (A) to post-intervention (B1) and with maintained effect at follow-up (B2) (7, 10), and three children with no effect over time (5, 8, 9), in duration of computer use (black line), and in the number of computer activities (red line). * Missing days due to that the child was sick.
Primary Y-axis: minutes; secondary Y-axis: number of activities. Black line: duration of computer use. Red line: number of computer activities.
Change in percentage of days
As shown in , seven children both increased in percentage of days from A to B1, and maintained a positive change from A to B2 (1–5, 7, 10), even though some children decreased at B2 compared to B1 (1, 3, 5, 7). From A to B2, the three remaining children had no change or a decreased percentage of days over time. Isaac (6) already had a high percentage of days at A, and maintained this level with no change over time. Marcus (9) decreased in percentage of days over time, and Lucas (8) did not maintain the increased percentage of days from B1 to B2.
Figure 4. Percentage of days with computer use (%) over time for each child. Three children used a gaze-based AT at baseline (6, 8, 9), one child a head-controlled mouse (5), and one child a switch (10).
Goal attainment
A total of 58 goals were formulated at baseline for the 10 children (mean = 6 goals, median = 6 goals, range 3–9 goals/child), for gaze-based AT usage in school (37 goals), and/or at home (21 goals). The formulated goals considered using the gaze-based AT to communicate with others (20 goals), to interact with others (seven goals), learning to use and regular usage of the gaze-based AT (13 goals), to make choices (12 goals), and to do school tasks (six goals). Achieved goals are shown in .
Table 4. Description of attained goals for each child.
All children attained goals, and the number of attained goals (scoring zero or higher) increased over time, with 55% attaining goals during the intervention (32/58), and 60% post-intervention (35/58). Post-intervention, 22 goals were attained in school (22/37) and 13 goals at home (13/21). Eight children attained between half of the goals to all goals post-intervention, whereas two children attained less than half of the goals (2, 5) (see ). Each child with unattained goals (six children, 23 goals) had at least one goal (1–4 goals) that showed progress post-intervention (14 goals scoring −1). Three children had unattained goals only in school (4–6). Unattained goals with no change as well as with progress were found in all different areas of use (communication, interaction, regular use, choices, and school tasks).
Satisfaction of gaze-based AT and services
Post-intervention the parents gave a high satisfaction rating for the gaze-based AT (Device median: 3.9, q1–q3: 3.4–4.2) and for the service delivery (median: 4.3, q1–q3: 4.3–4.4). At post-intervention the median value of the total scale was 4.0 (q1–q3: 3.7–4.2). The parents gave a somewhat lower satisfaction at follow-up (Device: median, 3.4; q1–q3: 3.0–4.1; Service median 3.1, q1–q3: 2.8–4.3; Total scale median 3.5, q1–q3: 3.0–3.9). On an item level for the eight Device items most parents (6/10 to 8/10) were satisfied (scoring 4 or 5) at post-intervention with all items except for the items durability (5/10) and comfort (5/10). At follow-up most parents (6/10 or 7/10) were still satisfied with four out of eight Device items (dimensions, safety, ease of use, and effectiveness). Concerning the four Service items, a majority of the parents were satisfied with all items at post-intervention (B1) while a majority were satisfied only with professional services at follow-up (B2) as follows: service delivery (B1 8/10; B2, 5/10), repairs & services (B1: 10/10; B2 4/10), professional services (B1: 9/10; B2 6/10), and follow-up services (B1 9/10; B2 3/10). At time point for follow-up the three most important items identified were as ease of use (7/10), effectiveness (6/10), and follow-up (3/10).
Discussion
This study shows that children with a severe physical impairment without speaking ability can increase their repertoire of doable computer activities with a gaze-based AT. Seven children, of different ages, increased the number of performed computer activities from baseline to follow-up. Thus, these results were consistent even after withdrawal of services related to the gaze-based AT intervention. Research indicates that children with the most severe motor impairments (GMFCS IV or V) are those that have the lowest level of participation in activities,Citation45,Citation46 and are therefore the ones most likely to need a computer to be able to perform activities. Research indicates that these children need a high level of support from others to participate in activities.Citation10,Citation23 Among children with such profound impairments, every computer activity that expands the repertoire of doable activities may therefore be a significant contribution for the specific child to explore childhood activities. In the present study, the MPC team collaborated with parents and teachers to promote the implementation of gaze-based AT in daily activities. The need for collaboration between professionals and parents and teachers has been highlighted by previous research,Citation16 which found that absence of guidance to parents and teachers in how to expand the repertoire of activities with the gaze-based AT led to a limited repertoire of doable activities for the children.
The visual analysis of data shows that post-intervention, eight children increased their computer usage either regarding the number of performed activities per day, time spent performing activities per day, and/or the percentage of days with gaze-based AT use, and the effect was maintained at follow-up. However, due to the nonexperimental design the internal validity may be compromised in this studyCitation47 and the results with increased computer usage over time therefore need to be interpreted carefully.
The results also reveal that all children achieved goals with the use of gaze-based AT, and eight children completed between half to all of the goals. The completeness of goals thereby shows the effectiveness of gaze-based AT and how it differed among the children themselves. A reason for unattained goals could be that the children did not formulate the goals due to their communication difficulties. Although the children’s motivation for specific activities was considered by adults, unattained goals may be due to the lack of or decreased motivation from the child to perform a certain activity. Another reason for unattained goals might be that too many goals were formulated at a time. Most children achieved three to four goals, which might be a reasonable number to work with at a time. At least three goals are recommended for the GAS.Citation39 However, as the gaze-based AT was implemented in two settings at the same time (school and home), several goals were formulated for each setting. The results indicate that when formulating goals both for home and for school, everyone involved needs to be aware that too many goals might be set. Another explanation for unattained goals is special events, such as sickness periods, that may have hindered the achievement of goals for the two children that achieved less than half of the goals (children 2 and 5).
The results show that children mostly used the gaze-based AT for up to 1 hour per user day. However, it remains unknown whether the children in the present study were satisfied with the amount of usage, or whether they would have liked to perform more activities or spend more time using the gaze-based AT. The AT usage will be determined by the interplay between the child, the activity, the AT, and the specific environment.Citation26 Although these children with a gaze-based AT can perform activities without support from others, they will still be dependent on a supportive environment for setting up the system and positioning the child at the computer, after which they will be free to explore computer activities.
The current study confirms the need of longitudinal measures of the use and usability of AT to understand its effect in daily activities, as suggested in the literature.Citation30 Although children maintained a positive change at follow-up compared to baseline, the results also demonstrate that for some children there were decreased changes between post-intervention and follow-up. This result indicates a need for recurring support to maintain a high level of long-term use. In addition to ongoing technical support, children, parents, and teachers will need follow-up services to continue to adapt the gaze-based AT to the children’s changing needs and accommodate their development. Based on the current study’s results, a recommendation is to offer follow-up services (e.g., one or two days), from an MPC team once a year after the gaze-based AT intervention, to promote sustained high use of the gaze-based AT.
The results indicate high satisfaction of parents with the gaze-based AT, and with services related to the gaze-based AT intervention. High satisfaction with the AT is in line with results from a survey study among adults with severe physical impairments using gaze-based AT in daily life.Citation32 On the other hand, in contrast to the current study’s finding, dissatisfaction with professional services has been found among parents of children with physical impairments using different ATs.Citation18,Citation20 In addition, a survey study of adult users of AT found low satisfaction to be related to the abandonment of AT.Citation48 Therefore, the high satisfaction both with the gaze-based AT and with the services among parents found in this study at post-intervention might be a prerequisite for the results with sustained use of gaze-based AT over time. Nevertheless, a majority of parents were satisfied with all services at the end of gaze-based AT intervention, but only with the professional services at follow-up. For example, the results show that few parents were satisfied with the technical support and follow-up services for the period from the end of gaze-based AT intervention to the time point for follow-up. It would be interesting to further investigate in a future study what made these changes. Measuring parents’ satisfaction is important, as they are the ones that primarily implement interventions in the families’ routines and daily life for children with impairments.Citation24
The present study indicates that the gaze-based AT intervention supported use of gaze-based AT over time, after withdrawal of services related to the gaze-based AT intervention. It appears that the intervention program empowered parents and teachers to support the child in the use of AT with less support from professionals over time. This finding is in line with research that indicates that involving key persons in decision-making and goal formulation and empowering key persons with knowledge and skills needed (e.g., handling technology, adapting the content, supporting the child in the use) are necessary to achieve sustained use of AT over time.Citation16,Citation19,Citation24,Citation49,Citation50 As pointed out by previous research,Citation51 to achieve good outcomes for students with severe impairments, extended time is needed as well as opportunities to develop mutual understanding and joint efforts among multiple key persons.
The current study suggests that introducing gaze-based AT in daily activities together with receiving the services spread out during a time period of 10 months is related to the goal achievement of gaze-based AT usage for nonspeaking children with severe physical impairments. More goals were also achieved at 9–10 months after the start of the intervention program, than at 5 months. Several children had health-related issues during the gaze-based AT intervention, which is common in this child group.Citation52 Therefore, the time frame needs to allow for these extraordinary events during the implementation of the gaze-based AT in daily activities. In addition, case studies suggest that gaze-based AT needs to be implemented over an extended time to maintain motivation and interest for individuals with profound impairments.Citation14 Such a time frame also allows the content in the communication pages in gaze-based AT to be gradually increased over time in response to the changing needs and abilities of the user.Citation14
The service in the gaze-based AT intervention is based on several interacting key elements (increase knowledge, collaboration between key persons, child’s preferences for usage, and goal setting). Whether some key elements are more influential than others in maintained use of gaze-based AT cannot be concluded from this study. Nevertheless, previous research indicates these key elements to be of significance in intervention studies with children with physical impairments.Citation38,Citation51,Citation53
A strength of this study is its daily measures of gaze-based AT usage over 14-day periods, which allowed any fluctuations in usage during each of these periods to be tracked. A limitation of the study is that only 10 children participated and therefore the results need to be interpreted carefully. Representing a small group of children, all children that were referred to one regional pediatric center in Sweden over a period of 3 years were included in this study. However, a larger group of children might have revealed a more varied use of the gaze-based AT after the gaze-based AT intervention. The limited information of children’s cognitive level is also a limitation in the study. Assessing cognitive level in children with both severe motor and communicative impairment is difficult due to their restricted ability to participate in a standardized assessment situation.Citation54 Notwithstanding, population-based studies show that cognitive impairment correlates with the severity of motor impairmentCitation5 and is more common among children with low functional level in communication,Citation55 such as in the present study.
The responsiveness of GAS depends on the professionals’ knowledge in selecting goals and levels representing important change.Citation40,Citation56 The MPC team in this study was educated in using GAS. In addition, research team also checked goals for relevance and measurability. A potential response bias is that the computer use diaries with estimations of gaze-based AT usage were filled in by parents, teachers, and assistants. It is known that familiar partners may have a tendency to present a more favorable image of a situation,Citation47 such as overestimation of the duration of gaze-based AT usage due to expectations. This needs to be considered when interpreting the results. To reduce the recall bias, they were instructed to note the minutes of use directly after each activity throughout each day. Furthermore, none of the researchers, parents, teachers, or assistants involved in measuring outcomes was blind to the intervention. Blinding to type of AT is not possible if the purpose is to observe AT usage. Due to ethical considerations blinding to receiving service or not is difficult. For example, it cannot be recommended to give service only to some of the children who are provided with gaze-based AT.
The results in this study are based upon measurements. The study does not include qualitative information from parents or teachers on functional changes and experiences of gaze-based AT usage in daily life. Parents’ and teachers’ experiences will be reported in two forthcoming studies.
Declaration of interest
The authors report no conflicts of interest.
Acknowledgments
The authors would like to thank the participating children, parents, and school personnel for taking part in the data collection, and Tobii Technology for lending some of the equipment.
Funding
This study was funded by the Swedish Research Council, Jimmy Dahlstens Fond, and Stiftelsen Sunnerdahls Handikappfond.
Additional information
Funding
References
- Henderson S, Skelton H, Rosenbaum P. Assistive devices for children with functional impairments: impact on child and caregiver function. Developmental Medicine & Child Neurology 2008;50(2):89–98.
- Berry BE, Ignash S. Assistive technology: providing independence for individuals with disabilities. Rehabilitation Nursing 2003;28(1):6–14.
- Chantry J, Dunford C. How do computer assistive technologies enhance participation in childhood occupations for children with multiple and complex disabilities? A review of the current literature. British Journal of Occupal Therapy 2010;73(8):351–365.
- Himmelmann K, Hagberg G, Beckung E, Hagberg B, Uvebrant P. The changing panorama of cerebral palsy in Sweden. IX. Prevalence and origin in the birth‐year period 1995–1998. Acta Paediatrica 2005;94(3):287–294.
- Himmelmann K, Uvebrant P. Function and neuroimaging in cerebral palsy: a population‐based study. Developmental Medicine & Child Neurology 2011;53(6):516–521.
- Fauconnier J, Dickinson HO, Beckung E, Marcelli M, McManus V, Michelsen SI, et al. Participation in life situations of 8–12 year old children with cerebral palsy: cross sectional European study. British Medical Journal 2009;338(24):b1458.
- Novak I, Hines M, Goldsmith S, Barclay R. Clinical prognostic messages from a systematic review on cerebral palsy. Pediatrics 2012;130(5):e1285–e1312.
- Majnemer A, Shevell M, Law M, Birnbaum R, Chilingaryan G, Rosenbaum P, et al. Participation and enjoyment of leisure activities in school‐aged children with cerebral palsy. Developmental Medicine & Child Neurology 2008;50(10):751–758.
- Raghavendra P, Virgo R, Olsson C, Connell T, Lane AE. Activity participation of children with complex communication needs, physical disabilities and typically-developing peers. Developmental Neurorehabilitation 2011;14(3):145–155.
- Raghavendra P, Olsson C, Sampson J, Mcinerney R, Connell T. School participation and social networks of children with complex communication needs, physical disabilities, and typically developing peers. Augmentative and Alternative Communication 2012;28(1):33–43.
- Krantz O. Assistive devices utilisation in activities of everyday life–a proposed framework of understanding a user perspective. Disability and Rehabilitation: Assistive Technology 2012;7(3):189–198.
- ISO 9999:2011. Assistive products for persons with disability - classification and terminology [Internet]. International Organization for Standardization; 2011 – [cited 2014 Dec 19]. Available from: http://www.iso.org/iso/home.html
- Donegan M, Morris JD, Corno F, Signorile I, Chió A, Pasian V, et al. Understanding users and their needs. Universal Access in the Information Society 2009;8(4):259–275.
- Donegan M. Participatory design: the story of Jayne and other complex cases. In Majaranta P, Aoki H, Donegan M, Hansen DW, Hansen JP, Hyrskykari A, Räihä K (Eds). Gaze Interaction and Applications of Eye Tracking: advances in assistive technologies (pp. 55–61), 2012.
- Lariviere JA. Eye tracking: eye-gaze technology. In Soderback I (Ed). International Handbook of Occupational Therapy Interventions (pp. 339–362), 2014.
- van Niekerk K, Tönsing K. Eye gaze technology: a South African perspective. Disability and Rehabilitation: Assistive Technology 2014(0):1–7.
- Hornof AJ, Cavender A. EyeDraw: enabling children with severe motor impairments to draw with their eyes. Conference on Human Factors in Computing Systems (pp. 161–170), 2005.
- Anderson K, Balandin S, Stancliffe R. Australian parents’ experiences of speech generating device (SGD) service delivery. Developmental Neurorehabilitation 2014;17(2):75–83.
- Baxter S, Enderby P, Evans P, Judge S. Barriers and facilitators to the use of high‐technology augmentative and alternative communication devices: a systematic review and qualitative synthesis. International Journal of Language & Communication Disorders 2012;47(2):115–129.
- Desideri L, Stefanelli B, Bitelli C, Roentgen U, Gelderblom G, de Witte L. Satisfaction of users with assistive technology service delivery: an exploratory analysis of experiences of parents of children with physical and multiple disabilities. Developmental Neurorehabilitation 2014(30):1–12.
- Lenker JA, Fuhrer MJ, Jutai JW, Demers L, Scherer MJ, DeRuyter F. Treatment theory, intervention specification, and treatment fidelity in assistive technology outcomes research. Assistive Technology 2010;22(3):129–138.
- Hemmingsson H, Lidstrom H, Nygard L. Use of assistive technology devices in mainstream schools: Students’ perspective. The American Journal of Occupational Therapy 2009;63(4):463–472.
- Østensjø S, Carlberg EB, Vøllestad NK. The use and impact of assistive devices and other environmental modifications on everyday activities and care in young children with cerebral palsy. Disability and Rehabilitation 2005;27(14):849–861.
- Granlund M, Bjorck-Akesson E, Wilder J, Ylven R. AAC interventions for children in a family environment: implementing evidence in practice. Augmentative Alternative Communication 2008;24(3):207–219.
- Salminen A, Ryan S, Petrie H. Impact of computer augmented communication on the daily lives of speech-impaired children. Part II: services to support computer augmented communication. Technology & Disability 2004;16(3):169–177.
- Cook AM, Polgar JM, Hussey SM. Cook & Hussey’s Assistive Technologies: Principles and Practice. 3rd ed., 2008.
- Lenker JA, Paquet VL. A new conceptual model for assistive technology outcomes research and practice. Assistive Technology 2004;16(1):1–10.
- ISO 9241-11: Ergonomic requirements for office work with visual display terminals (VDTs): Part 11: Guidance on usability [Internet]. International Organization for Standardization; 1998 – [cited 2015 June 25]. Available from: http://www.iso.org/iso/home.html
- Lenker JA, Scherer MJ, Fuhrer MJ, Jutai JW, DeRuyter F. Psychometric and administrative properties of measures used in assistive technology device outcomes research. Assistive Technology 2005;17(1):7–22.
- Arthanat S, Nochajski SM, Lenker JA, Bauer SM, Wu YWB. Measuring usability of assistive technology from a multicontextual perspective: the case of power wheelchairs. The American Journal of Occupational Therapy 2009;63(6):751.
- Ball L, Nordness A, Fager S, Kersch K, Pattee G, Beukelman D. Eye-gaze access of AAC technology for persons with amyotrophic lateral sclerosis. Journal Medical Speech Language Pathology 2010;18:11–23.
- Caligari M, Godi M, Guglielmetti S, Franchignoni F, Nardone A. Eye tracking communication devices in amyotrophic lateral sclerosis: impact on disability and quality of life. Amyotrophic Lateral Sclerosis and Frontotemporal Degeneration 2013;14(7–8):546–552.
- Spataro R, Ciriacono M, Manno C, La Bella V. The eye‐tracking computer device for communication in amyotrophic lateral sclerosis. Acta Neurologica Scandinavica 2014;130(1):40–45.
- Borgestig M, Sandqvist J, Parsons R, Falkmer T, Hemmingsson H. Eye gaze performance for children with severe physical impairments using gaze-based assistive technology - a longitudinal study. Assistive Technology 2015. Advanced online publication.
- Fager S, Beukelman DR, Fried-Oken M, Jakobs T, Baker J. Access interface strategies. Assistive Technology 2012;24(1):25–33.
- Eccles M, Grimshaw J, Campbell M, Ramsay C. Research designs for studies evaluating the effectiveness of change and improvement strategies. Quality and Safety in Health Care 2003;12:47–52.
- Assistive Technology Products (AAC) [Internet]. Tobii Technology; 2013 - [cited 2014 Dec 22]. Available from: http://www.tobii.com/en/assistive-technology/global/products/old-or-discontinued-products/.
- Borgestig M, Falkmer T, Hemmingsson H. Improving computer usage for students with physical disabilities through a collaborative approach: a pilot study. Scandinavian Journal of Occupational Therapy 2013;20(6):463–470.
- Kiresuk TJ, Smith A, Cardillo JE. Goal attainment scaling: applications, theory, and measurement. 1994.
- Sakzewski L, Boyd R, Ziviani J. Clinimetric properties of participation measures for 5‐to 13‐year‐old children with cerebral palsy: a systematic review. Developmental Medicine & Child Neurology 2007;49(3):232–240.
- Steenbeek D, Gorter JW, Ketelaar M, Galama K, Lindeman E. Responsiveness of goal attainment scaling in comparison to two standardized measures in outcome evaluation of children with cerebral palsy. Clinical Rehabilitation 2011;25(12):1128–1139.
- Palisano RJ. Validity of goal attainment scaling in infants with motor delays. Physical Therapy1993; 73(10):651–658.
- Demers L, Weiss-Lambrou R, Ska B. The Quebec user evaluation of satisfaction with assistive technology (QUEST 2.0): an overview and recent progress. Technology and Disability 2002;14(3):101–105.
- Demers L, Weiss-Lambrou R, Ska B. Quebec User Evaluation of Satisfaction with Assistive Technology QUEST version 2.0. An outcome measure for assistive technology devices. [Internet]. MIDSS; [cited 2015 Nov 03]. doi:10.13072/midss.298
- King G, Imms C, Palisano R, Majnemer A, Chiarello L, Orlin M, et al. Geographical patterns in the recreation and leisure participation of children and youth with cerebral palsy: a CAPE international collaborative network study. Developmental Neurorehabilitation 2013;16(3):196–206.
- Orlin MN, Palisano RJ, Chiarello LA, Kang LJ, Polansky M, Almasri N, et al. Participation in home, extracurricular, and community activities among children and young people with cerebral palsy. Developmental Medicine & Child Neurology 2010;52(2):160–166.
- Polit DF, Beck CT. Nursing research: generating and assessing evidence for nursing practice. 9th ed. 2008.
- Federici S, Borsci S. Providing assistive technology in Italy: the perceived delivery process quality as affecting abandonment. Disability and Rehabilitation: Assistive Technology 2014;17:1–10.
- Hasselbring TS, Glaser CHW. Use of computer technology to help students with special needs. The Future of Children 2000;10:102–122.
- Copley J, Ziviani J. Barriers to the use of assistive technology for children with multiple disabilities. Occupational Therapy International 2004;11(4):229–243.
- Villeneuve M. A critical examination of school-based occupational therapy collaborative consultation. Canadian Journal of Occupational Therapy 2009;76 Spec No:206–218.
- Beckung E, White‐Koning M, Marcelli M, McManus V, Michelsen S, Parkes J, et al. Health status of children with cerebral palsy living in Europe: a multi‐centre study. Child: Care, Health and Development 2008;34(6):806–814.
- Hoppestad BS. Inadequacies in computer access using assistive technology devices in profoundly disabled individuals: an overview of the current literature. Disability & Rehabilitation: Assistive Technology 2007;2(4):189–199.
- Yin Foo R, Guppy M, Johnston LM. Intelligence assessments for children with cerebral palsy: a systematic review. Developmental Medicine & Child Neurology 2013;55(10):911–918.
- Himmelmann K, Lindh K, Hidecker MJ. Communication ability in cerebral palsy: a study from the CP register of western Sweden. European Journal of Paediatric Neurology 2013;17(6):568–574.
- Steenbeek D, Ketelaar M, Galama K, Gorter JW. Goal attainment scaling in paediatric rehabilitation: a critical review of the literature. Developmental Medicine & Child Neurology 2007;49(7):550–556.