
Abstract
This study evaluates perceptual changes in speech production accuracy in six children (3–11 years) with moderate-to-severe speech impairment associated with cerebral palsy before, during, and after participation in a motor-speech intervention program (Prompts for Restructuring Oral Muscular Phonetic Targets). An A1BCA2 single subject research design was implemented. Subsequent to the baseline phase (phase A1), phase B targeted each participant's first intervention priority on the PROMPT motor-speech hierarchy. Phase C then targeted one level higher. Weekly speech probes were administered, containing trained and untrained words at the two levels of intervention, plus an additional level that served as a control goal. The speech probes were analysed for motor-speech-movement-parameters and perceptual accuracy. Analysis of the speech probe data showed all participants recorded a statistically significant change. Between phases A1–B and B–C 6/6 and 4/6 participants, respectively, recorded a statistically significant increase in performance level on the motor speech movement patterns targeted during the training of that intervention. The preliminary data presented in this study make a contribution to providing evidence that supports the use of a treatment approach aligned with dynamic systems theory to improve the motor-speech movement patterns and speech production accuracy in children with cerebral palsy.
Introduction
Cerebral palsy (CP) is a neurodevelopmental condition that includes a group of non-progressive movement and posture disorders that are a result of lesions or dysfunction to the central nervous system. The worldwide prevalence is reported to be ˜2–2.5 per 1000 live births (CitationAshwal, Russman, Blasco, Miller, Sandler, Shevell, et al., 2004; CitationLin, 2003), making it one of the most prevalent childhood disorders. The literature identifies at least 40% of children with CP present with communication impairment (CitationKennes, Rosenbaum, Hanna, Walter, Russell, Raina, et al., 2002). Due to the complex interaction between multiple systems (e.g., physical, cognitive, sensory, and communicative), children with motor speech disorders associated with CP are at increased risk of social and educational limitations, and participation restrictions (CitationVoorman, Dallmeijer, Van Eck, & Schuengel, 2010).
Given this, one of the primary objectives of speech intervention is to improve communicative function and increase speech intelligibility by “maximizing the ability to speak within neurological limits”, thereby improving an individual's quality-of-life (CitationWorkinger, 2005). Speech production is a goal-oriented process requiring precise timing and accurate positioning of multiple sub-speech systems of the jaw, lips, tongue, velum, vocal folds, and respiratory system (CitationGreen, Moore, Higashikawa, & Steeve, 2000). It has been hypothesized that impairment to the speech sub-systems in children with CP may be attributed to a poor relationship between the motor command and perceptual consequences of the speech movement (CitationHoon, Stashinko, Nagae, Lin, Keller, Bastian, et al., 2009; CitationKent & Netsell, 1978).
Recent brain imaging studies show that children with CP indeed present with injury to the sensory system that includes a reduction in white matter fibres connecting to the sensory cortex (CitationHoon et al., 2009). These findings support the hypothesis that impaired motor speech control in children with CP could be associated with the selection of inefficient or ineffective movement strategies due to insufficient information regarding control, adjustment, and stabilization through peripheral (sensory) input. Research findings indicate the enhancement of somatosensory input during speech can not only affect change in the co-ordination of movement synergies, but also influence learning that can be maintained across time (CitationIto & Ostry, 2010). These findings suggest potential therapeutic value in enhancing tactile-kinaesthetic input to children with CP.
In this paper, the effectiveness of a motor-speech intervention approach, aimed at improving speech production accuracy in six children with cerebral palsy, is evaluated. The PROMPT (Prompts for Restructuring Oral Muscular Phonetic Targets) approach was selected due to the theoretical foundation of PROMPT; and the focus on enhancing motor learning through active task-specific augmentation of sensory information.
Theoretical foundation
The PROMPT approach is aligned with the core principles of dynamic systems theory (DST) (CitationHayden, 2006). Within these principles, it is considered that: growth and development are driven by continuous change within the inter-dependent domains/sub-systems that are both within and external to an individual. In order for a new behaviour to develop there must be a state of disequilibrium that functions to move the system to re-organize (CitationThelen & Smith, 2003); sub-system re-organization results in the emergence of new behaviours at a higher level of complexity and moves the system back to a new level of equilibrium. This process of self-organization evolves in a hierarchical manner, building on lower levels of organization (CitationHowe & Lewis, 2005); and individual, task, and environmental constraints/catalysts function as a means to (re)structure the system and guide emerging behaviours (CitationNewell, 1991).
Within the constructs of DST, impairments in body structure and function associated with CP have the potential to prevent integration between interdependent domains/sub-systems, thus constraining the emergence of higher level behaviours (CitationHadders-Algra, 2000). This may result in children with CP continuing to select the same inefficient motor solution as compared to typically-developing children. The continued and persistent use of inefficient behaviour can create rate-limiting systems that maintain deep stable attractor states resistant to change.
Within PROMPT, speech motor development is viewed as consisting of co-dependent sub-systems, with skill acquisition subject to the bidirectional interaction between existing and developing systems. Thus, motor learning is characterized by an alteration to the movement synergies unique to each individual (CitationKostrubiec, Tallet, & Zanone, 2006). The PROMPT clinician is trained to assess the speech sub-systems and work to promote co-ordination through the establishment of efficient functional higher order synergies.
Evaluation of the motor speech system (respiration, phonation, articulation, prosody) is assessed and interpreted using the PROMPT Motor Speech Hierarchy (MSH) (CitationHayden & Square, 1994). The MSH is based upon the hierarchical sequence of motor speech development (that is, the jaw provides the foundation for the integration of lip and tongue movements) and consists of seven levels. The first two levels focus on postural support for speech, and the ability to produce sound for at least 2–3 seconds. Levels 3–5 focus on training the appropriate movement patterns for speech of the jaw, the lips, and the tongue. The last two levels address the sequencing of movements seen in speech and prosody.
Intervention techniques are used to facilitate or act as a control parameter in bringing about change toward a higher level of functioning. This would occur as a result of the establishment of a new set of boundary conditions enhancing the search for stable and adaptive co-ordination solutions to task demands (CitationNewell & Valvano, 1998). Tactile-kinaesthetic input is used to re-structure the degrees of freedom available in a speech system to facilitate controlled flexible movements (as bound by conditions of time and space) for accurate speech production.
Enhancing motor learning through active task-specific augmentation of sensory information
Increasingly, the literature is highlighting the significant role somatosensory input plays in motor speech control and learning (CitationEstep, 2009; CitationIto & Ostry, 2010). In particular, recent research has shown that the speech production system is responsive to the provision of enhanced kinaesthetic information. Further the type, placement, and context in which tactile-kinaesthetic input is provided are essential in facilitating sensory-motor re-organization (CitationGick, Ikegami, & Derrick, 2010; CitationWilston, Reed, & Braida, 2010). These findings are supported by behavioural studies that indicate sensory augmentation can play a role in enhancing motor learning in general, particularly when stimuli are difficult to perceive (CitationAtchy-Dalama, Peper, Zanone, & Beek, 2005). For example, researchers have demonstrated that modifications to the speech system through external perturbation (i.e., stretching of the facial skin at the lateral angle of the mouth) changes speech production (CitationEstep & Barlow, 2007). Further, articulator coupling patterns will re-organize or compensate as a response to modifications/disruptions in articulator movements (CitationEstep, 2009).
Intervention approaches designed to utilize tactile-kinaesthetic input to improve speech production have been documented in the literature (CitationChumpelik, 1984; CitationGordon-Brannan & Weiss, 2007; CitationStrand, Stoekel, & Baas, 2006). Of these approaches, PROMPT has developed specific types of prompts to facilitate improved articulatory control (CitationHayden, 2003). Tactile-kinaesthetic input during active speech is directed to specific orofacial regions richly innervated with slowly adapting, cutaneous mechanoreceptors that are responsive to external low level inputs during motor activity (CitationFeng, Gracco, & Max, 2011; CitationTrulsson & Johansson, 2002). This approach has been identified as having direct relevance to children with motor speech disorders (CitationMurdoch & Horton, 1998).
The data reported in this paper form part of a longitudinal single subject research design (SSRD) study aimed at evaluating the effectiveness of PROMPT in making change to speech production accuracy, in children with CP (CitationWard, 2012; CitationWard, Strauss, & Leitão, 2013). CitationWard et al. (2013) report the kinematic and speech intelligibility data for six children with CP subsequent to receiving PROMPT intervention. This paper reports on the data addressing perceptual changes in speech production accuracy for these same six participants.
A single subject research design (SSRD) was implemented based on the heterogeneity and small number of available participants for the study as well as the lack of existing efficacy studies. This study is consistent with a phase I intervention study (CitationRobey, 2004).
It was postulated that intervention focused on strengthening the weakest sub-system, with consideration given to individual, environmental, and task constraints, will result in the emergence of new higher level functional behaviours. It was hypothesized that:
(1) The training of new motor-speech movement patterns will result in improved speech production accuracy;
(2) A non-linear treatment effect will be observed, with the initial treatment phase recording the greatest magnitude of change;
(3) No significant change in the control targets will be observed; and
(4) Continued skill acquisition during the follow-up non-intervention period is expected with stabilization of the newly acquired motor-speech-movement patterns.
Method
Participants
illustrates the participant characteristics of the six participants (three males, three females, age range 3–11 years), as described in CitationWard et al. (2013).
Table I. Participant characteristics.
Inclusion criteria were: diagnosis of CP, aged between 3–14 years, a standard score ≥ 1.5 SD below the mean on the Arizona Proficiency Scale–3rd Revision (Arizona-3) (CitationFudala, 2001), and a developmental quotient ≥ 70 as measured on the Leiter-Brief International Performance Scale R Brief (Leiter-R) (CitationRoid & Miller, 1997). Exclusion criteria were: receptive language impairment > 2 SD below the mean on the CELF-P (CitationWiig, Secord, & Semel, 1992) or CELF 4 (CitationSemel, Wiig, & Secord, 1995), a hearing impairment > 25 dB hearing loss, the absence of motor speech impairment (i.e., within age appropriate limits on The Verbal Motor Production Assessment for Children (VMPAC) (CitationHayden & Square, 1999), non-correctable visual impairment, and past exposure to PROMPT intervention.
Procedure
A single-subject A1BCA2 multiple-baseline-across-participants-and-behaviours research design was utilized as reported in CitationWard et al. (2013). The phases are summarized below:
Phase A1: Baseline data collection phase. This phase ranged from 5–8 weeks.
Upon completion of a 5-week baseline-data-collection period and evidence of stable baselines (as assessed through statistical process control), participants were randomly allocated to commence intervention, while other participants remained in baseline. This process continued on a staggered basis until all participants commenced intervention (CitationPortney & Watkins, 2009).
Phase B: PROMPT intervention aimed at one level of the PROMPT motor speech hierarchy (MSH).
Phase C. PROMPT intervention aimed at one level higher on the MSH.
Phases B and C each consisted of weekly individual intervention blocks, 45 minutes in length for 10 weeks. Therapy sessions occurred at the same time of day on the same day of the week.
Phase A2: Follow-up data collection at 12 weeks post-phase C. This consisted of two data collection sessions, with the speech probe data collected in the second session. Following this study phase, all participants returned to their regular therapy services, consistent with the baseline phase.
The use of a SSRD, with two inter-hierarchical phases (B and C) of intervention, provides the opportunity to evaluate the time course of motor learning in terms of skill acquisition, consolidation, savings, and interference to achieve accurate speech production. Experimental control was maintained through the establishment of a stable baseline for all participants prior to the commencement of intervention; and the repeated measurements of both targeted and control behaviours, throughout the study phases.
Measures
Weekly speech probes were administered within each study phase. The speech probes consisted of three groups of 20 words. Group one contained trained and untrained words based on intervention priority one (IP1), group two contained trained and untrained words based on intervention priority two (IP2), and group three contained control words based on the untrained intervention priority three (control goal).
At each testing session, six cards from each of the five trained and untrained 20-word pools were randomly selected, to give a total of 30 words to be used on that day. These cards were then shuffled and administered to the children in random order. At the end of the session, the cards were returned to the word pools. At the next session, six words were selected randomly again, without any consideration of which words had been chosen in any previous sessions. The word pools were individualized to each participant and designed to facilitate the establishment of new motor-speech movement patterns. See for an example of the speech probe word-set for one participant.
An independent PROMPT trained speech-language pathologist (referred to as the transcriber), blinded to the phases of the study and the participants, completed the scoring of the speech data. Each word was scored for accuracy of the targeted motor speech movement pattern (MSMP) and perceptual accuracy (PA). A binary coding system was used to code each parameter, where 0 = inaccurate and 1 = accurate. A score of 1 was assigned as follows:
MSMP: the targeted motor speech movement pattern of that intervention priority for the individual participant was appropriately executed. Words containing more than one movement goal (e.g., push = lip-to-lip contact for /p/ and rounding /sh/) were assigned a fraction (e.g., /p/ = 1/2, /sh/ = 1/2 point) to enable a maximum score of one point for each parameter.
PA: production of the target word was perceptually correct based on the extIPA diacritics (CitationBall & Müller, 2005) that code sliding articulation, tongue position (e.g., retracted, bladed), dental production of bilabials, labial spreading, and nasalization.
Scoring process
Pre-training
The transcriber and chief investigator jointly transcribed a speech sample of a child (non-participant) with moderate-to-severe speech disorder, with speech characteristics similar to the speech of the children anticipated to participate in the study. The key error patterns sampled were discussed and key diacritics of the extIPA used to represent these errors were identified.
Consensus
The transcriber and chief investigator independently transcribed a speech sample of a child (non-participant) with a moderate-to-severe speech disorder using narrow phonetic transcription. All points of difference or disagreement were discussed and transcription consensus reached. Upon obtaining 90% inter-rater agreement, the transcriber commenced independent transcription of the speech samples of the participants.
Intervention
Intervention protocols were designed and administered in accordance with the tenets of the PROMPT philosophy, as detailed in the Introduction to Technique manual (CitationHayden, 2003). The PROMPT approach incorporates dynamic tactile-kinaesthetic-proprioceptive input to facilitate speech production. The tactile input administered was dependent on the needs of the individual participant.
Video footage of each participant completing the Arizona-3, and the chief investigator's observations of each participant's motor speech movement patterns, was sent to Ms Deborah Hayden (Director and Founder of the PROMPT Institute) for confirmation of the intervention priorities for each participant, and the speech probe word-sets.
Upon confirmation of the intervention goals, the chief investigator consulted with the treating speech pathologist to set the intervention protocol tailored to reflect the individual interests and age of each participant, as described in CitationWard et al. (2013).
Three intervention priorities were selected: Treatment objectives written for the first two objectives and the third intervention priority served as an untreated control goal. Participants 2, 3, 5, and 6 targeted mandibular control in phase B and labial-facial control in phase C. Participant 1 targeted labial-facial control in phase B and lingual control in phase C. Participant 4 targeted mandibular and labial-facial control simultaneously in phase B and lingual control in phase C. Each participant's intervention priorities across the intervention phases are illustrated in .
Table II. Participant intervention priorities.
Participants attended therapy once a week for a duration of 45 minutes. Each treatment session followed the same format. The session commenced with a 5-minute warm-up period, followed by a 15-minute activity. Upon completion of the activity, a second 5-minute warm-up was followed by a second 15-minute activity. The warm-up period consisted of massed practice of individual phonemes and words. All participants were encouraged to start in a neutral posture (i.e., lips softly closed together without excessive retraction). Knowledge of performance feedback was provided after each trial. During the 15-minute activity words from the trained word-set pool were practiced in a distributed manner. Knowledge of performance and results were randomly given. No prescribed schedule was adhered to and varied across the therapy sessions. However, therapists were required to provide information regarding the motor movement pattern and perceptual accuracy. For example, “you opened your mouth too wide, let's do that again with a smaller mouth”. The PROMPT technique was applied as described in the Introduction to Technique Manual (CitationHayden, 2003).
Four PROMPT trained therapists administered the intervention protocols. Inclusion criteria for therapist participation in the study included (a) completion of the Introduction to Technique workshop, (b) completion of the case study detailed in the Introduction to Technique manual within 3 months of the workshop, (c) regular use of the technique for at least 9 months, (d) attendance at a PROMPT mentoring day held by Deborah Hayden in October 2006, (e) a fidelity rating to the PROMPT approach of no less than 80%, as assessed by an independent senior PROMPT Instructor, and (f) an expression of interest to participate in the study. The therapists only administered the PROMPT intervention and were not involved in any scoring or administration of testing protocols.
Reliability and fidelity
Speech data
Twenty per cent of the data were randomly selected by the research assistant and given to the transcriber for rescoring. Intra-rater agreements of 94% and 93% for accuracy of speech production and motor-speech-movement-parameters respectively, were achieved.
Fifty per cent of the data were randomly selected for determination of inter-rater reliability. An inter-rater agreement of 87% and 91% for accuracy of speech production and motor-speech-movement-parameters respectively, was achieved. These agreement values are within the range deemed “acceptable” for research needs (CitationShriberg, Fourakis, Hall, Karlsson, Lohmeier, McSweeney, et al., 2010).
Intervention
The PROMPT Institute provided an independent senior PROMPT Instructor, who was blinded to the phases of the study and the intervention session, to evaluate each therapist's fidelity to the treatment approach, using the PROMPT fidelity protocol (CitationRogers, Hayden, Hepburn, Charlifue-Smith, Hall, & Hayes, 2006).
Prior to commencing the study, each therapist's fidelity to the PROMPT approach was evaluated, with all therapists obtaining a minimum of 80% fidelity. Two further fidelity measures, per participant, per intervention phase, were taken to generate a total of four fidelity ratings per participant. Fidelity measures throughout intervention block one (phase B) ranged between 77.7–93.7%. All therapists achieved the desired 80% fidelity during intervention block two (phase C), with scores ranging between 80.2–97%.
Data analyses
The determination of intervention effects in SSRD requires a judgement about changes in: stability (consistency of response over time), magnitude (level), and trend (direction) of performance both within and between the study phases (CitationPortney & Watkins, 2009).
In addition to visual inspection, statistical methods were used to evaluate changes in the data as follows:
(1) Change in performance level using the two standard deviation (2 SD) band analysis. Typically a significant change is considered to have occurred when two consecutive points fall outside the upper and lower confidence levels. However, given there were insufficient data points to calculate the degree of serial dependency, a more stringent criterion of three consecutive data points was used (CitationOrme & Cox, 2001).
(2) Change in trend using the conservative dual-criterion method of trend estimation with binomial test (CitationFisher, Kelley, & Lomas, 2003; CitationWambaugh & Mauszycki, 2010).
(3) The magnitude of the treatment effect calculated using a modified Cohen's d, based on the pooled standard deviation (CitationDunst, Hamby, & Trivette, 2004; CitationSolanas, Manolov, & Onghena, 2010).
Results
Visual inspection
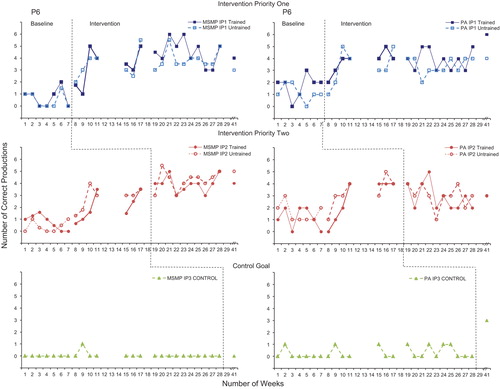
Graphs of the speech probe data across the study phases are shown in for each participant. These graphs show the effect of treatment on the motor-speech movement patterns and speech production accuracy following the training of the intervention priorities. Data for the MSMPs and PA for each intervention priority are presented in separate graphs, ordered from top to bottom, with the IP1 presented at the top, IP2 in the middle, and the control goal at the bottom. The data indicate low and stable baselines with a positive treatment effect evident for all participants on the trained and untrained word-sets. No significant changes were recorded in the control goal.
Figure 1. Accuracy of performance on the speech probes as scored for motor speech movement patterns (MSMP) and perceptual accuracy (PA) across the intervention priorities and study phases for P1.
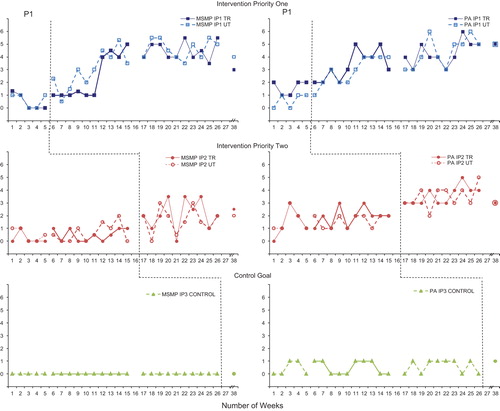
Figure 2. Accuracy of performance on the speech probes as scored for motor speech movement patterns (MSMP) and perceptual accuracy (PA) across the intervention priorities and study phases for P2.
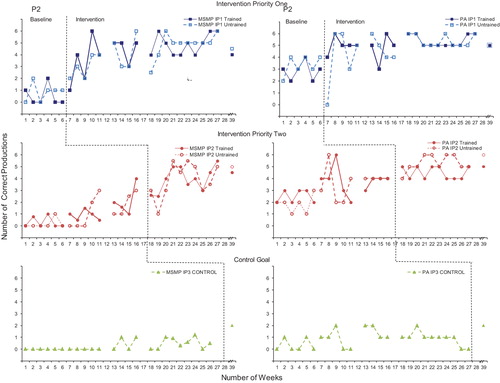
Figure 3. Accuracy of performance on the speech probes as scored for motor speech movement patterns (MSMP) and perceptual accuracy (PA) across the intervention priorities and study phases for P3.
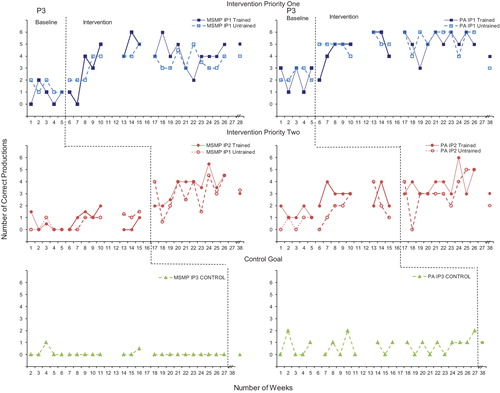
Figure 4. Accuracy of performance on the speech probes as scored for motor speech movement patterns (MSMP) and perceptual accuracy (PA) across the intervention priorities and study phases for P4.
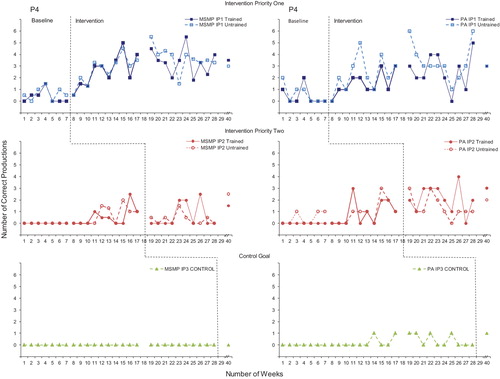
Figure 5. Accuracy of performance on the speech probes as scored for motor speech movement patterns (MSMP) and perceptual accuracy (PA) across the intervention priorities and study phases for P5.
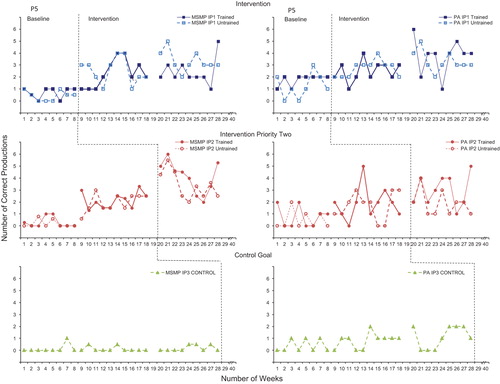
Figure 6. Accuracy of performance on the speech probes as scored for motor speech movement patterns (MSMP) and perceptual accuracy (PA) across the intervention priorities and study phases for P6.
Statistical analysis
Change in level
details a summary of the 2SD-band analysis on the speech probes for each intervention priority for each of the participants, across the study phases.
Table III. Summary of the two-standard deviation band analysis on the speech probes across the study phases for each of the participants.
The data show a significant change in performance level subsequent to the PROMPT intervention for:
(1) All participants on the MSMPs of intervention priority1 between phases A1–B; and 4/6 between phases B–C during the training of intervention priority 2. Five participants (one participant had no follow-up data) achieved a statistically significant increase at 12-weeks post-intervention (A2) as compared to phase A1.
(2) Four participants in PA of intervention priority 1 and intervention priority 2 between phases A1–B. In addition, one participant recorded a statistically significant increase in PA between phases B–C; and five participants achieved a statistically significant increase in intervention priority 2 between phases A1–C.
(3) All participants in PA on both intervention priorities at 12-weeks post-intervention.
No significant change to the control goal was recorded.
Change in slope
summarizes the split-middle and binomial tests on the speech probes for each of the participants across the study phases.
Table IV. Summary of the split-middle and binomial test on the speech probes across the study phases for each of the participants
The data show a significant change in trend direction subsequent to the PROMPT intervention for:
(1) All participants on the MSMPs of IP1 between phases A1–B.
(2) Five participants on the MSMPs of IP2 between phases A1–C, and 3/6 between phases B–C.
(3) Five participants in PA on IP1 between phases A1–B.
(4) All participants in PA on IP2 between phases A1–C and one participant between phases B–C.
No significant change to the control goal was recorded.
Effect size
The magnitude of the treatment effect was evaluated using the Cohen's d effect size, calculated across each of the study phases (see ). The data indicate a cumulative treatment effect for all perceptual outcome measures across the study phases, with phases A1–B and A1–A2 recording the largest effect size.
Table V. Effect size data on the speech probes across the phases of the study for each participant.
Discussion
The findings of this study show all participants recorded substantial change in speech production accuracy subsequent to the PROMPT intervention. Speech production accuracy was assessed for both attainment of the targeted motor-speech movement pattern (MSMP) and perceptual accuracy (PA) using weekly speech probes. All participants recorded changes on the trained and untrained speech probes for the intervention priorities targeted during both intervention phases of the study, with the initial treatment phase recording the greatest magnitude of change. There was no significant change to the control word-sets, thus providing evidence that the changes in perceptual accuracy and motor speech movement patterns were due to the effectiveness of the therapy. These findings are consistent with the study hypotheses.
The use of a single-subject research design with two inter-hierarchical phases of intervention provided the opportunity to evaluate the time course of motor learning in terms of skill acquisition and consolidation (CitationKostrubiec et al., 2006; CitationLuft & Buitrago, 2005). Specifically, the initial relatively short-term skill acquisition of the first intervention priority in intervention block one (phase B) can be compared to the ongoing skill acquisition/consolidation of that same skill, during a second intervention phase that targeted a second intervention priority (phase C). The subsequent introduction of a second priority during the second intervention phase presented the opportunity to make observations regarding effect of therapy on the first intervention priority during the training of the second intervention priority (anterograde interference).
The results of this study are discussed in turn, for each intervention priority across the study phases.
Intervention priority one
Phase B: Skill acquisition
Two patterns of motor learning were evident. An initial rapid and immediate change followed by incremental improvement was observed in P2–P6. The second pattern was defined by small and gradual change that continued throughout the intervention phase (P1). This second pattern had limited change from baseline data until week 8, where a rapid gain followed by gradual skill acquisition was observed. These results are consistent with data reported from intervention studies aimed at developing complex motor control skills in children with cerebral palsy (CitationBarnes & Whinnery, 2002; CitationShumway-Cook, Hutchinson, Kartin, Price, & Woollacott, 2003).
Possible explanations for the different patterns of learning in children with CP could be linked to severity, diagnosis, age, or any non-linear combination of these. CitationShumway-Cook et al. (2003) suggested patterns of motor learning observed in their study were associated with the level of disability. They report two participants rated level I on the GMFCS (least severe) with spastic hemiplegia showed rapid change, whilst three participants rated at level II with diplegia showed gradual improvement. Similar to Shumway-Cook et-al. (2003), the participant to record the most gradual change in this study (P1) differed from the other participants in terms of diagnosis and intervention priorities targeted. P1 was rated level III on the GMFCS with a diagnosis of athetosis, had the severest global motor score on the VMPAC, and was also the oldest. Thus, it is also possible that the pattern of learning is influenced by age. For example, the youngest participants (P5, P6) in this study recorded a rapid profile of change.
These data indicate a complicated and non-linear relationship of skill acquisition in individuals with neurologic impairment. This is illustrated in the data of P3. This participant had a diagnosis of spastic quadriparesis, was rated level II on the GMFCS, and recorded the second lowest global motor score on the VMPAC. The severity of motor impairment suggests this participant should have recorded a gradual pattern of change. However, P3 recorded a pattern more consistent with rapid change.
Phase C: Consolidation
The hypothesis that training the second intervention priority in phase C would not interfere with consolidation of the earlier trained behaviour (intervention priority one) in phase B was supported. During phase C, when intervention priority two was targeted, the overall pattern observed in the data for intervention priority one was consistent with a phase of consolidation. This was indicated by a decrease in the steepness of the slope, small incremental gains in performance level, and increased stability in the data.
The results obtained in phase C are discussed within the context of resource allocation as well as the role of tactile-kinaesthetic input. In this study, resource allocation is considered in terms of both cognitive attention required for the task and strength of coupling between the existing and “to-be-learned” behaviour (CitationTemprado, Zanone, Monno, & Laurent, 2001).
Learning a sequenced task (as is required in speech) involves consolidation of both explicit and implicit components of the task, with these two components operating on different time scales (CitationGhilardi, Moisello, Silvestri, Ghez, & Krakauer, 2009). The literature suggests children with CP are less successful than TD peers in learning sequences due to increased cognitive demands that contributed to impaired implicit and explicit memory skills (CitationGagliardi, Tavano, Turconi, Pozzoli, & Borgatti, 2011).
Empirical evidence to support the hypothesis that training one intervention priority at a time has the benefit of decreasing the cognitive load can be found in co-ordination studies. For example, CitationSerrien (2009) explored the competition between new (2:1 finger-tapping task) and existing (1:1 in/anti-phase finger task) dynamics in a bimanual finger-tapping task, using two experimental conditions with an ABA design.Whilst both groups recorded significantly improved performance in the training task, the participants that had their training schedules interrupted with another task (that consisted of an already acquired behaviour) were less accurate. The interpretation of this finding was that competition occurred as a result of attending to two tasks, and provides evidence that attending to two tasks during the rapid acquisition phase can create competition between the existing skill and the new to be-developed skill.
Despite the lesser complexity of these experimental tasks compared to speech, the findings could support the interpretation that training the second intervention priority separately, as opposed to interweaving the two intervention priorities in the same phase, promoted stabilization due to minimization of competing resource allocation. Further, empirical data indicates the greater the coupling (intrinsic biomechanical properties, cognitive demands and task constraints) between the existing (intervention priority one) and new behaviour (intervention priority two), the greater the resistance to interference (CitationTemprado et al., 2001). The speech science literature supports the notion of a lower order jaw/lip and higher order lip aperture synergy (CitationSmith & Zelaznik, 2004). It is possible that the inter-articulator coupling associated with the jaw/lower lip synergy, and use of tactile-kinaesthetic input to control the degrees of freedom of movement, promoted consolidation.
It is proposed that the tactile-kinaesthetic input provided in this study served to stabilize the first intervention priority (as shown by the small incremental gain and decrease in variability) whilst destabilizing the second intervention priority, to facilitate a phase shift toward a transition of change. CitationKelso, Fink, DeLaplain, and Carson (2001) state “coupling specific aspects of an individual movement to specific sensory information from the environment serves to stabilize co-ordination globally” (p. 1210). They report haptic information serves to stabilize movement patterns in one training condition, whilst destabilizing in another condition. The data from this study are consistent with this statement.
Intervention priority two
Phase B: Skill acquisition
Visual inspection of the speech probe data indicates the training of IP1 affected the performance of IP2 during phase B. Two participants (P4 and P5) recorded a significant change in performance level to the MSMPs of IP2, whilst four participants recorded a significant change in PA. Further, the data shows increased variability in comparison with the baseline phase.
CitationMattar and Ostry (2007) provide evidence that suggests increased generalization should be expected when training movements that are close together and involve similar patterns of muscle activation. The results observed in this study support these findings for the four participants who were directly targeted for mandibular control (intervention priority one). Empirical data indicate the jaw is the primary articulator, with early lip movements tied to mandibular control in early motor development (CitationGreen et al., 2000; CitationGreen, Moore, & Reilly, 2002; CitationWalsh, Smith, & Weber-Fox, 2006). Studies have also demonstrated that perturbation of the jaw will cause compensatory changes to the lips (CitationGomi, Honda, Ito, & Murano, 2002). It was, therefore, hypothesized that improving and refining control of the mandible would result in changes at the labial-facial level of control.
Additional support for the interpretation that movements that involve similar patterns show better generalization is also found in the data recorded for P1. This participant commenced training at the labial-facial level of control (IP1). The second intervention priority targeted lingual control. Whilst there was an increase in the variability of IP2 during the training of IP1, there was no change in performance level or trend direction. As explained by CitationMattar and Ostry (2007), it may be that the patterns of muscle activation were too dissimilar and, thus, generalization was less.
Research aimed at evaluating single vs concurrent acquisition would further our knowledge pertaining to competing attention in skill acquisition in children with CP. It is well recognized that the type of training schedule affects motor learning (CitationMaas, Robin, Austermann Hula, Wulf, Ballard, & Schmidt, 2008). Whilst the literature also provides evidence to support concurrent skills training, there are limited data available that examine schedules of motor skill learning in children with CP. Recently, CitationWambaugh and Mauszycki (2010) reported evidence of over-generalization in a participant with acquired apraxia of speech, subsequent to dual skills training. They postulated impaired sensory motor integration may have attributed to over-generalization observed in the participant in their study. Given children with CP present with impaired sensory motor integration this needs to be further examined when considering intervention protocols.
Phase C: Interference
The changes observed in IP2 in phase C are interpreted with reference to behavioural studies that have explored the effect of anterograde interference on motor learning (CitationKelso & Zanone, 2002; CitationKrakauer, Mazzoni, Ghazisadeh, Ravindran, & Shadmehr, 2006; CitationSing & Smith, 2010). Anterograde interference refers to the process by which learning a novel task (task B) is influenced by the previously learned behaviours (task A). Of particular interest to this study are the data reported by CitationSing and Smith (2010) that suggest the learning of a subsequent task may proceed more slowly than the previously trained task. Visual inspection of the data during the training of the second intervention priority (phase C) show the maximum performance level achieved was 67% for MSMPS and 75% for PA on the trained word set. Whilst the change in performance level was statistically significant for five participants, the level of performance and rate of learning on IP2 was less than IP1 for all participants in this study. These results are, therefore, consistent with findings reported in the literature.
Two possible explanations for interference include the level of skill mastery and the effect of task similarity. CitationSing and Smith (2010) found that duration of training, and not necessarily the level of mastery, had a significant impact on the degree of interference. They state “the amount of anterograde interference depends systematically on the strength of a particular component of the initial adaptation rather than on the total amount of adaptation that is achieved” (p. 2). Specifically, the group of participants in their study that had more training trials (230-trial group) had more interference than the group that received less training (13-trial group), even though this group had recorded a lower level of mastery.
The data from this study challenge the application of high level skill mastery as a criterion for continuing or terminating intervention. Typically the success of an intervention program is based on performance mastery, with a mastery criterion typically of ˜ 80–90% applied before proceeding to the next intervention phase (CitationWilliams, 2000). This study differed in that an a priori decision was made to continue intervention, regardless of performance gain (CitationGierut, 1998). None of the participants recorded performance mastery of the MSMPs above 66% in IP1. However, all participants with the exception of P4 made progress on IP2. In addition, there was minimal interference on IP1. It is therefore interpreted that a mastery of 80% accuracy is not a requirement for moving to a second intervention priority. In fact, it could be argued that setting a criterion of mastery too high could interfere with the mastery of a second higher-order skill. These results support the statement of CitationRvachew, Rafaat, and Martin (1999) that “it is unnecessary and inefficient to treat an individual target sound continuously until mastery is achieved [emphasis added]” (p. 33).
A second explanation for the observation of minimal interference is based on evidence that suggests learning both requires and results in the modification of pre-existing behaviours (CitationKelso & Zanone, 2002). Thus, the learning of a new task may be expected to either co-operate or compete with existing behaviours. A “to-be-learned behaviour” that co-operates with a previously learned behaviour is expected to increase the rate of learning as a result of a reduction of competition between task requirements.
The data from this study indicate that the training of IP1 was a co-operative priority to IP2, for the participants who commenced training at the mandibular level of control. Continued improvement to IP1 was recorded in five participants, between baseline and the second intervention priority.
An example of how training of a second intervention priority competes with previously learned behaviour is evident in the data from P4. The clinician was required to support mandibular stability for P4 whilst targeting labial-facial control. This participant recorded data that showed rapid but variable skill acquisition in the first intervention priority. During the training of the second intervention priority, the first intervention priority maintained a variable pattern of performance, with a slight decrease in the trend direction. No real change was observed in the performance accuracy of the second intervention priority in this phase. Thus, the data from this participant support the notion that training of the first intervention priority was successful because the muscles of activation were similar; however, the second intervention priority (lingual control) introduced patterns of activation that were too dissimilar and contributed to resource competition.
Further, the results suggest that changes to the higher order synergy of lip aperture required greater refinement and, therefore, lagged the MSMP changes. Whilst significant changes in the MSMPs were recorded between phases B–C, changes in PA reached statistical significance between phases A–C for five participants, but only one participant recorded a statistically significant change between phases B–C.
Interpretation of the results of this study, as considered within the theoretical perspective framework of dynamic systems theory (and co-ordination dynamics) suggest the learning of IP2 (for five participants) was sympathetic to the skills acquired in IP1, and therefore promoted learning of the second intervention priority. For one participant, the second intervention priority introduced competition. This perspective supports the results that were obtained not only on the speech production measures discussed here, but also the kinematic measures discussed in CitationWard et al. (2013).
The results obtained in this study indicate the need for additional research to further develop our understanding of our ability to predict the influence of interference on motor learning. The role for further research aimed at not only examining the rate and level of performance change, but also potential to influence performance mastery by manipulating time frames within treatment designs requires further investigation.
Limitations
Single word measures were used in this study due to the severity of the speech impairment in the participants. This does not recognize that speech intelligibility is a multi-dimensional construct influenced by factors that include linguistic complexity. For example, CitationHustad (2012) reports data that indicates children with CP experience decreased speech intelligibility with increasing sentence length. This study could have been strengthened through the use of an outcome measure designed to enable the systematic evaluation of changes to speech production with increasing linguistic complexity (CitationHodge & Whitehall, 2010).
Further, it is acknowledged this is an early phase experimental research study, with a small participant sample. Further research is required to evaluate the effectiveness of this approach in a larger group of children with CP, as well as compare the effectiveness with an alternate approach.
Conclusion
The data from this study provide preliminary evidence to suggest that an intervention approach framed within the principles of DST; and aimed at developing efficient functional movement patterns, through the establishment of appropriate movement boundaries, resulted in improved motor-speech control. These findings support the need for further investigation of therapy protocols designed to accommodate different phases of motor-learning in targeting motor-speech strategies in children with CP.
The application of the principles of motor learning in speech-language intervention protocols is strongly recommended (CitationLudlow, Hoit, Kent, Ramig, Shrivastav, Strand, et al., 2008; CitationMaas et al., 2008). Whilst the principles of motor learning are considered essential components of intervention approaches focused on the development of motor skills, research into these principles has been largely limited to the typically-developing population. The results of our study suggest that participants not only exhibited the two phases of skill acquisition and consolidation consistent with the general motor control literature, but that they also continued to record improvements during the non-intervention follow-up phase. This phenomenon has been previously documented in the motor learning literature for children with CP subsequent to physiotherapy intervention (CitationTrahan & Malouin, 2002).
Acknowledgements
This research was completed as part of a Doctoral Program completed in March 2012. The authors wish to acknowledge the families and staff at the Centre for Cerebral Palsy for their participation in this study. In addition, the authors acknowledge Dr Marie Blackmore (The Centre for Cerebral Palsy), Associate Professor Anne Ozanne and Dr Beverly Joffe (LaTrobe University) for their contributions to the research design and earlier phases of the study, and Peter McKinnon (Statistician, School of Physiotherapy) for support with the statistics. This study was made possible in part due to funding from the Centre for Cerebral Palsy, The CP Trust of the Centre for Cerebral Palsy and Non-Government Centre Support funding.
Declaration of interest: The authors report no conflicts of interest. The authors alone are responsible for the content and writing of the paper.
References
- Ashwal, S., Russman, B. S., Blasco, P. A., Miller, G., Sandler, A., Shevell, M., et al. (2004). Practice parameter: Diagnostic assessment of cerebral palsy. Neurology, 62, 851–863.
- Atchy-Dalama, P., Peper, C. E., Zanone, P., & Beek, P. J. (2005). Movement-related sensory feedback mediates the learning of a new bimanual relative phase pattern. Journal of Motor Behavior, 37, 186–196.
- Ball, M. J., & Müller, N. (2005). Phonetics for communication disorders. Mahwah, NJ: Lawrence Erlbaum Associates.
- Barnes, S. B., & Whinnery, K. W. (2002). Effects of functional mobility skills training for young students with physical disabilities. Council for Exceptional Children, 68, 313–324.
- Chumpelik, D. (1984). The PROMPT system of therapy: Theoretical framework and applications for developmental apraxia of speech. Seminars in Speech and Language, 5, 139–155.
- Dunst, C. J., Hamby, D. W., & Trivette, C. (2004). Guidelines for calculating effect sizes for practice-based research syntheses. Centrescope: Evidence-based approaches to early childhood development, 3, 1–10.
- Estep, M. (2009). Modulation, adaptation, and control of orofacial pathways in healthy adults. Journal of Communication Disorders, 42, 280–285.
- Estep, M., & Barlow, S. M. (2007). Modulation of the trigeminofacial pathway during syllabic speech. Brain Research, 1171, 67–74.
- Feng, Y., Gracco, V. L., & Max, L. (2011). Integration of auditory and somatosensory error signals in the neural control of speech movements. Journal of Neurophysiology, 106, 667–679.
- Fisher, W. W., Kelley, M. E., & Lomas, J. E. (2003). Visual aids and structured criteria for improving visual inspection and interpretation of single-case designs. Journal of Applied Behaviour Analysis, 36, 387–406.
- Fudala, J. (2001). Arizona Articulation Proficiency Scale, Third Revision. Los Angeles, CA: Western Psychological Services.
- Gagliardi, C., Tavano, A., Turconi, A. C., Pozzoli, U., & Borgatti, R. (2011). Sequence learning in cerebral palsy. Pediatric Neurology, 44, 207–213.
- Ghilardi, M. F., Moisello, C., Silvestri, G., Ghez, C., & Krakauer, J. W. (2009). Learning of a sequential motor skill comprises explicit and implicit components that consolidate differently. Journal of Neurophysiology, 101, 2218–2229.
- Gick, B., Ikegami, Y., & Derrick, D. (2010). The temporal window of audio-tactile integration in speech perception. Journal of the Acoustical Society of America, 125, EL342–EL346.
- Gierut, J. (1998). Treatment efficacy: Functional phonological disorders in children. Journal of Speech, Language, and Hearing Research, 41, S85–S100.
- Gomi, H., Honda, M., Ito, T., & Murano, E. Z. (2002). Compensatory articulation during bilabial fricative production by regulating muscle stiffness. Journal of Phonetics, 30, 261–279.
- Gordon-Brannan, M. E., & Weiss, C. E. (2007). Clinical management of articulatory and phonologic disorders. Third edition. Baltimore, MD: Lippincott Williams and Wilkins.
- Green, J. R., Moore, C., & Reilly, K. (2002). The sequential development of jaw and lip control. Journal of Speech, Language, and Hearing Research, 45, 66–79.
- Green, J. R., Moore, C., Higashikawa, M., & Steeve, R. (2000). The physiologic development of speech motor control: Lip and jaw coordination. Journal of Speech, Language, and Hearing Research, 43, 239–255.
- Hadders-Algra, M. (2000). The neuronal group selection theory: Promising principles for understanding and treating developmental motor disorders. Developmental Medicine and Child Neurology, 42, 707–715.
- Hayden, D. (2003). PROMPT introduction to technique manual. Sante Fe, NM: The PROMPT Institute.
- Hayden, D. (2006). The PROMPT Model: Use and application for children with mixed phonological impairment. Advances in Speech-Language Pathology, 8, 265–281.
- Hayden, D., & Square, P. (1994). Motor speech treatment hierarchy: A systems approach. Clinics in Communication Disorders, 4, 162–174.
- Hayden, D., & Square, P. (1999). Verbal Motor Production Assessment for Children. Examiner’s Manual. San Antonio, TX: The Psychological Corporation.
- Hodge, M., & Whitehall, T. (2010). Intelligibility impairments. In J. S Damico, N. Müller, & M. J. Ball (Eds.), The handbook of language and speech disorders (pp. 99–114). Oxford, UK: Wiley-Blackwell.
- Hoon, A. H., Stashinko, E. E., Nagae, L. M., Lin, D. D., Keller, J., Bastian, A., et al. (2009). Sensory and motor deficits in children with cerebral palsy born preterm correlate with diffusion tensor imaging abnormalities in thalamocortical pathways. Developmental Medicine and Child Neurology, 51, 697–704.
- Howe, M. L., & Lewis, M. D. (2005). The importance of dynamic systems approaches for understanding development. Developmental Review, 25, 247–251.
- Hustad, K., Schueler, B., Schultz, L., & Duhadway, C. (2012). Intelligibility of 4 year old children with and without cerebral palsy. Journal of Speech, Language, and Hearing Research, 55, 1177–1189.
- Ito, T., & Ostry, D. J. (2010). Somatosensory contribution of motor learning due to facial skin deformation. Journal of Neurophysiology, 104, 1230–1238.
- Kelso, J. A. S., & Zanone, P. (2002). Coordination dynamics of learning and transfer across different effector systems. Journal of Experimental Psychology: Human Perception and Performance, 28, 776–797.
- Kelso, J. A. S., Fink, P. W., DeLaplain, C. R., & Carson, R. G. (2001). Haptic information stabilizes and destabilizes coordination dynamics. Proceedings of the Royal Society of London, 268, 1207–1213.
- Kennes, J., Rosenbaum, P., Hanna, S. E., Walter, S., Russell, D., Raina, P., et al. (2002). Health status of school-aged children with cerebral palsy: Information from a population-based sample. Developmental Medicine and Child Neurology, 44, 240–247.
- Kent, R. D., & Netsell, R. (1978). Articulatory abnormalities in athetoid cerebral palsy. Journal of Speech and Hearing Disorders, 43, 353–373.
- Kostrubiec, V., Tallet, J., & Zanone, P. (2006). How a new behavioral pattern is stabilized with learning determines its persistence and flexibility in memory. Experimental Brain Research, 170, 238–244.
- Krakauer, J. W., Mazzoni, P., Ghazisadeh, A., Ravindran, R., & Shadmehr, R. (2006). Generalization of motor learning depends on the history of prior action. PLoS Biology, 4, e316.
- Lin, J. (2003). The cerebral palsies: A physiological approach. Journal of Neurology, Neurosurgery and Psychiatry, 74 (Suppl. 1), i23–29.
- Ludlow, C. L., Hoit, J., Kent, R., Ramig, L. O., Shrivastav, R., Strand, E. A., et al. (2008). Translating principles of neural plasticity into research on speech motor control reocery and rehabilitation. Journal of Speech, Language, and Hearing Research, 51, S240–S258.
- Luft, A. R., & Buitrago, M. M. (2005). Stages of motor skill learning. Molecular Neurobiology, 32, 205–216.
- Maas, E., Robin, D. A., Austermann Hula, S. N., Wulf, G., Ballard, K. J., & Schmidt, R. A. (2008). Principles of motor learning in treatment of motor speech disorders. American Journal of Speech-Language Pathology, 17, 277–298.
- Mattar, A. G., & Ostry, D. J. (2007). Modificability of generalization in dynamics learning. Journal of Neurophysiology, 98, 3321–3329.
- Murdoch, B., & Horton, S. K., (Eds.). (1998). Acquired and developmental dysarthria in childhood. Cheltenham, UK: Stanley Thornes.
- Newell, K. M. (1991). Motor learning in practice: A constraints led approach. Annual Review of Psychology, 42, 213–237.
- Newell, K. M., & Valvano, J. (1998). Therapeutic intervention as a constraint in learning and relearning movement skills. Scandinavian Journal of Occupational Therapy, 5, 51–57.
- Orme, J. G., & Cox, M. E. (2001). Analyzing single-subject design data using statistical process control charts. Social Work Research, 25, 115–127.
- Portney, L., & Watkins, M. (2009). Foundations of clinical research. Applications to practice (3rd ed.). Upper Saddle River, NJ: Prentice Hall Health.
- Robey, R. R. (2004). A five-phase model for clinical-outcome research. Journal of Communication Disorders, 37, 401–411.
- Rogers, S., Hayden, D., Hepburn, S., Charlifue-Smith, R., Hall, T., & Hayes, A. (2006). Teaching young nonverbal children with autism useful speech: A pilot study of the Denver Model and PROMPT interventions. Journal of Autism and Developmental Disorders, 36, 1007–1024.
- Roid, G., & Miller, L. (1997). Leiter International Performance Scale-Revised. Wood Dale, IL: Stoelting Company.
- Rvachew, S., Rafaat, S., & Martin, M. (1999). Stimulability, speech perception skills, and the treatment of phonological disorders. American Journal of Speech-Language Pathology, 8, 33–43.
- Semel, E., Wiig, E., & Secord, W. (1995). Clinical Evaluation of Language Fundamentals (4th ed.). San Antonio, TX: The Psychological Corporation.
- Serrien, D. (2009). Interactions between new and pre-existing dynamics in bimanual movement control. Experimental Brain Research, 197, 269–278.
- Shriberg, L. D., Fourakis, M., Hall, S. D., Karlsson, H. B., Lohmeier, H. L., McSweeney, J. L., et al. (2010). Perceptual and acoustic reliability estimates for the speech disorders classification system (SDCS). Clinical Linguistics and Phonetics, 24, 825–846.
- Shumway-Cook, A., Hutchinson, S., Kartin, D., Price, R., & Woollacott, M. (2003). Effect of balance recovery of stability in children with cerebral palsy. Developmental Medicine and Child Neurology, 45, 591–602.
- Sing, G. C., & Smith, A. M. (2010). Reduction in learning rates associated with anterograde interference results from interactions between different timescales in motor adaptation. PLoS Computation Biology, 6, e1000893.
- Smith, A., & Zelaznik, H. N. (2004). Development of functional synergies for speech motor coordination in childhood and adolescence. Developmental Psychobiology, 45, 22–33.
- Solanas, A., Manolov, R., & Onghena, P. (2010). Estimating slope and level change in N = 1 designs. Behavior Modification, 34, 195–218.
- Strand, E. A., Stoekel, R., & Baas, B. (2006). Treatment of severe childhood apraxia of speech: A treatment efficacy study. Journal of Medical Speech-Language Pathology, 14, 297–307.
- Temprado, J., Zanone, P. G., Monno, A., & Laurent, M. (2001). A dynamical framework to understand performance trade-offs and interference in dual tasks. Journal of Experimental Psychology: Human Perception and Performance, 27, 1303–1313.
- Thelen, E., & Smith, A. (2003). Development as a dynamic system. Trends in Cognitive Sciences, 7, 343–348.
- Trahan, J., & Malouin, F. (2002). Intermittent intensive physiotherapy in children with cerebral palsy: A pilot study. Developmental Medicine and Child Neurology, 44, 233–239.
- Trulsson, M., & Johansson, R. (2002). Orofacial mechanoreceptors in humans: Encoding characteristics and responses during natural orofacial behaviors. Behavioural Brain Research, 135, 227–233.
- Voorman, J. M., Dallmeijer, A. J., Van Eck, M., & Schuengel, C. (2010). Social functioning and communication in children with cerebral palsy: Association with disease characteristics and personal and environmental factors. Developmental Medicine and Child Neurology, 52, 441–447.
- Walsh, B., Smith, A., & Weber-Fox C. (2006). Short-term plasticity in children’s speech motor systems. Developmental Psychobiology, 48, 660–674.
- Wambaugh, J. L., & Mauszycki, S. (2010). Sound treatment: Application with severe apraxia of speech. Aphasiology, 24, 814–825.
- Ward, R. (2012). The effectiveness of PROMPT therapy for children with cerebral palsy. Doctoral thesis. Perth, Australia: Curtin University. http://espace.library.curtin.edu.au/R/?func = dbin-jump-full&object_id = 187094&local_base = GEN01-ERA02.
- Ward, R., Strauss, G., & Leitão, S. (2013). Kinematic changes in jaw and lip control of children with cerebral palsy following participation in a motor-speech (PROMPT) intervention. International Journal of Speech-Language Pathology, 15, 136–155.
- Wiig, E., Secord, W., & Semel, E. (1992). Clinical evaluation of language fundamentals - Preschool (CELF-P). San Antonio, TX: The Psychological Corporation.
- Williams, A. L. (2000). Multiple oppositions: Case studies of variables in phonological intervention. American Journal of Speech-Language Pathology, 9, 289–299.
- Wilston, E. C., Reed, C. M., & Braida, L. D. (2010). Integration of auditory and vibrotactile stimuli: Effects of frequency. Journal of the Acoustical Society of America, 127, 3044–3059.
- Workinger, M. (2005). Cerebral palsy resource guide for speech-language pathologists. Clifton Park, NY: Thomson Delmar Learning.