Abstract
Professionals learn and change throughout their careers. This continuing professional development is supported, in part, by educational activities developed by individuals, organisations or institutions.
In Europe and North America, processes have been established to set standards for the design and delivery of continuing healthcare professionals’ education (CE) that involve either approval of organisations as institutional providers of CE (i.e. accreditation) or approval of individual CE activities.
In systems based on provider accreditation, the accredited organisations develop into communities of practice that show evidence of learning and changing such as to allow the CE system to evolve. In addition the provider accreditation model provides an amplification effect not found in activity accreditation systems, whereby one accreditation decision can result in multiple activities being generated. Additional efficiencies can be identified and may be useful to those determining if a provider accreditation system is an appropriate fit for their system, for their context and for the culture of professional education in which they operate.
Keywords::
Professionals learn and change throughout their careers.Citation1 This continuing professional development is supported, in part, by educational activities developed by individuals, organisations or institutions.
In Europe and North America, processes have been established to set standards for the design and delivery of continuing healthcare professionals’ education (CE) and to certify that these standards have been met.Citation2–5 These processes involve either approval (i.e. accreditation) of organisations as institutional providers of CE,Citation2,Citation3 or approval of individual CE activities.Citation4,Citation5 The latter is referred to as activity accreditation.
In activity accreditation, there are standards set for the educational event or activity. Applicants for accreditation first plan the educational activity and then present documentation to the accreditor verifying compliance with the accreditor's standards. If the activity meets those standards, then the event is approved. The second approach is referred to as provider accreditation, where an organisation or institution as a whole, as well as a sample of individual activities, is evaluated to see if that organisation or institution meets the accreditor's standards. If it does, then the organisation is accredited as a provider of continuing professional education activities. In provider accreditation, the accredited provider is responsible for ensuring that every activity complies with the accreditation requirements, but all the activities are not individually reviewed by the accreditor.
In this essay, we seek to offer some perspectives on the attributes and outcomes of provider accreditation within our two continuing medical education systems. We hope that these perspectives will be of assistance to those considering whether a provider accreditation system is an appropriate fit for their system, for their context and for the culture of professional education in which they operate. This essay does not intend to compare and contrast provider accreditation and activity accreditation. The authors leave that comparison to the readers.
We believe there are four organisational or operational attributes of provider accreditation that are not often recognized and should be considered by those making decisions about the development of accreditation systems.
Organisational and operational advantages of provider accreditation
1. Provider accreditation contributes directly to the development and evolution of an institution or organisation beyond its ability just to create continuing education activities.
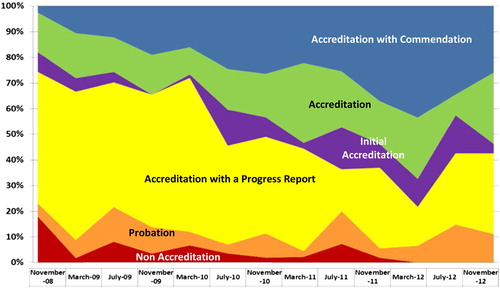
In provider accreditation there are requirementsCitation2,Citation3 that relate to the whole organisation (e.g. a statement of organisational mission; the need for the organisation to collaborate with other organisations; evidence that the organisation participates in healthcare quality improvement activities). These requirements result in accredited providers, as organisations, measurably changing and improving, over time, towards a common set of goals (). The system becomes populated with organisations that have demonstrated criterion-referenced development.
Figure 1. Accreditation outcomes for ACCME providers November 2008 to November 2012, as percentage of providers reviewed at each interval.
2. Provider accreditation predisposes to the development of a community of practice.
A community is “a group of people with a common characteristic or interest living together within a larger society”.Citation6 A community of practice develops around common goals or common interests. The development of a community of practice among accredited providers is based on their commitment to demonstrate the values and principles articulated within the system's accreditation standards. This community is self-organising with formalCitation7 and informal membership groups (e.g. LISTSERVEs, LinkedIn discussion groups, Twitter® feeds created by accredited providers), that offer the opportunity for interaction among leaders, educators and administrators in this community with common interests.
This community is a learning community and acts as an academy for learning about CE which, as a scholarly pursuitCitation8 can evolve and improve. This scholarship goes beyond discovery and includes the integration and application of new information on the effectiveness of CE into the practices of CE providers.Citation9 There are evidence-based accreditation requirementsCitation3 that reflect the integration of discovery into practice. As such, the community's learning can integrate the new knowledge developed in discovery within their CE programmes. This community is a conduit for the dissemination and distribution of important developments in education, administration and evaluation which are relevant to the effectiveness of CE (e.g. innovations in CE; compliance strategies; new laws; external forces impacting on accredited providers).
The provider community is also an evolving community. Changes in provider accreditation tend to be second-order changesCitation10 where the community itself is changed through accreditation requirements (e.g. the Accreditation Council for Continuing Medical Education (ACCME)'s 2006 engagement criteria and the ACCME's 2004 addition of requirements regarding the identification and resolution of conflict of interest). The self-organisation, tacit learning and the commitment to demonstrate quality within this community of practice are associated with interactions, interdependency and competition that contribute to the vibrancy and continuous improvement of accredited providers. As a community, accredited CE providers can participate in national and international systems for healthcare quality improvement. As a community of accredited providers, there are individuals and organisations for accreditation and CE advocacy that relate to and influence other parts of the health care system. For example, there are interactions between professional organisations, government and health care providers. Through this engagement, the community has the opportunity to integrate within and be relevant to the broader health care system and becomes a vehicle for advocacy and implementation of accreditation standards and practices.
3. There is an amplification effect in provider accreditation.
There is an amplification effect in provider accreditation not present in activity approval systems. In provider accreditation, one accreditation decision delivered to one accredited organisation can turn into hundreds of directly sponsored activities. However one accreditation decision delivered within the activity approval model results in only one activity. This is illustrated for the period 2008 to 2012 during which the European Accreditation Council for Continuing Medical Education (EACCME) of the Union of European Medical Specialists (UEMS) approved 6500 activities based on approximately 6500 applications.Citation5 During a similar time frame (2008 to 2011), the ACCME of the U.S.A. made more than 700 accreditation decisions and its accredited providers reported 365,718 continuing medical education activities.Citation11 This is more than a 500:1 ratio of activities to accreditation decisions by the ACCME system while the EACCME of the UEMS maintains a 1:1 ratio. This amplification effect has been manifest in the Royal College of Physicians and Surgeons of Canada (since 2004) and in the ACCME system since it began Annual Reports in 1998.
A subset of this amplification effect is the inclusion of jointly sponsored activities in the ACCME's provider accreditation system. For example, in 2011, the ACCME's accredited providers reported the development of 25,564 activities in partnership with non-accredited organisations. The ACCME providers reported that there were 2,775,911 individual registrants for these activities.Citation11 Through joint sponsorship, accreditation becomes empowering rather than constraining. Organisations can mentor other organisations through review of their performance to design and develop educational resources for learners. The amplification effect continues.
4. There is an inherent efficiency in provider accreditation.
In activity accreditation, one provider submits one activity to one standard-setting organisation for review and approval. The provider and the standard-setting organisation repeat the process for each activity for which approval is sought. One review results in the approval of one activity.
In provider accreditation, the provider submits material describing how the organisation meets the accreditation requirements. In the authors’ systems, these materials include 1) a narrative description of the organisation's compliance with the requirements and 2) documentation from a sample of activities that have already been presented. From these materials, the accreditor determines the organisation's compliance with the accreditation requirements. The accreditor renders an accreditation decision and sets a term for that accreditation. Accredited providers go on to develop and deliver any number of educational activities during their term of accreditation.
Provider accreditation takes advantage of such economies of scale and scope especially for the benefit of organisations that are developing multiple activities and for systems where large numbers of activities are being developed.
lists parameters the authors have identified that describe where providers and accreditors expend effort, or energy to ensure accreditation standards are met. The parameters represent the provider side (items 1, 2, 3 and 4) and the accreditor side (items 5 and 6) of the energy equation. In this model, regardless of the type of accreditation system, providers spend energy maintaining their organisation, developing educational activities and then submitting them for review by the accreditor. Accreditors spend a certain amount of energy reviewing each organisation's programme of CME and/or their activities. We believe, that while there is some variation, the amount of energy expended on each of these could be considered constant, in an energy equation or calculation.
Table 1. Where energy is expended for accredited continuing education.
Therefore, the number of activities created and the number of activities reviewed become the variables that determine the energy expended in the system.
Each activity would have to be reviewed by an accreditor in an activity approval/accreditation system. However, the number of activities reviewed by a provider accreditor is set by the accreditor. In the authors’ provider systems the accreditors have set this as 15 activities reviewed in each accreditation cycle.
Hypothetical values can be assigned to all these parameters from which the energy costs across a range of activity numbers within the two accreditation formats can be extrapolated. The authors have represented the results of these calculations in .
Figure 2. Energy cost of accreditation, by accreditation type.
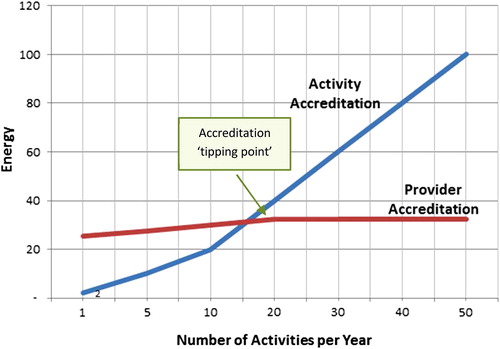
shows that in this hypothetical calculation, the energy cost within an activity accreditation system is lower than the energy cost of a provider accreditation system when providers are producing fewer than 15 activities per year. At this tipping point, the sum cost of approving each activity outweighs the providers’ costs of a programme review and the accreditors costs of performing a programme review. There are few opportunities for economies of scale or scope within activity accreditation. It is not clear how many CE submissions an activity accreditation system can accommodate. The ACCME system, which operates under provider accreditation, reports about 100,000 activities per year and utilises about 100 surveyors, 25 committee reviewers and 7 ACCME staff to accomplish this task.Citation12 The human and fiscal resources required to review 100,000 activities per year have never been determined but would surely be enormous.
Conclusion
Accreditation involves the setting of standards by an accreditor followed by a process to determine the degree to which adherence to these standards has been met. We have described the organisational and operational benefits of provider accreditation that include the development of a community of practice to foster learning, scholarship and system change. In addition, provider accreditation offers an amplification effect in the number of accredited CE activities that can be handled by the system as well as striking economies of scale and scope over activity accreditation.
Interestingly, regardless of the type of accreditation, in all cases, providers are notified that they have been given approval by the accreditor based on their ability to demonstrate their adherence to the established standards and requirements. So, one might say in the end, that all CE accreditation is in fact provider accreditation in which some systems offer provider accreditation one activity at a time. The cost effectiveness of this choice can be based in part on the economics resulting from our hypothetical model, as well as the potential impact that accreditation systems can have on both organisations and the broader health-care systems within which they exist.
Declaration of interest
The authors report no declarations of interest. The authors alone are responsible for the content and writing of the paper.
Author(s) Financial Disclosure
M.K. has disclosed that he has no relevant financial relationships.
C.C. has disclosed that he has no relevant financial relationships.
Peer Reviewers Financial Disclosure
Peer Reviewer 1 has disclosed that she has no relevant financial relationships.
Peer Reviewer 2 has disclosed that he has no relevant financial relationships.
References
- Regnier K, Kopelow M, Lane D, Alden E. Accreditation for learning and change: quality and improvement as the outcome. J Contin Educ Health Prof 2005;25:174–182.
- Royal College of Physicians and Surgeons of Canada found at http://www.royalcollege.ca, accessed December 28, 2012.
- Accreditation Council for Continuing Medical Education found at www.accme.org, accessed December 28, 2012.
- American Academy of Family Physicians found at www.aafp.org, accessed December 28, 2012.
- European Accreditation Council for Continuing Medical Education found at www.uems.net, accessed December 28, 2012.
- Merriam-Webster On-line Dictionary found at http://www.merriam-webster.com/dictionary/community, accessed December 24, 2012.
- Alliance for Continuing Education in the Health Professions found at http://www.acehp.org, accessed December 28, 2012.
- Boyer, Ernest, Scholarship Reconsidered: Priorities of the Professoriate. A Special Report Carnegie Foundation for the Advancement of Teaching, 1990.
- Marinopoulos SS, Dorman T, Ratanawongsa N, . Effectiveness of Continuing Medical Education. Evidence Report/Technology Assessment No. 149 (Prepared by the Johns Hopkins Evidence-based Practice Center, under Contract No. 290-02-0018.) AHRQ Publication No. 07-E006. Rockville, MD: Agency for Healthcare Research and Quality. January 2007.
- Porras JI, Robertson PJ. Organizational development: Theory, practice, and research. In: Dunnette MD, Hough LM (Eds.), Handbook of industrial and organizational psychology, (2nd ed., Vol. 3, pp. 719–822). Palo Alto, CA: Consulting Psychologists Press; 1992.
- Annual Report data, Accreditation Council fro Continuing Medical Education, accessed December 28, 2012.
- The ACCME at Work, available at http://www.accme.org/sites/default/files/Chapter%203_The%20National%20Accreditation%20System_20120927.pdf, accessed December 26, 2012.