The latest publication in the Journal is from North America and is an essay on the putative advantages of provider accreditation in CME. The authors describe their accreditation system in which educational providers apply to a regulatory authority for accreditation of their organisations on the basis of their performance over previous years. If successful, the providers are then free to plan and deliver their CME during the period of their awarded accreditation, which may vary from 2 years for providers considered sub-optimal to 6 years for commended providers.
In most European countries, activity accreditation is preferred to provider accreditation. Every proposed educational activity (live event or e-learning) is submitted for accreditation by its provider before the activity takes place. Activities designed for learners in their own countries are accredited by national accreditation authorities, whereas activities delivered on a European level are accredited by the European Accreditation Council for CME whose decision is based on reports from the relevant European specialty accreditation agency and from the national accreditation authority of the country where the activity will take place.
In their paper, the authors suggest that provider accreditation is characterised by four operational advantages that are not widely recognised. Firstly they believe that providers are stimulated to evolve and improve their performance; secondly that they develop into a community of practice which acts as an academy for continuing education; thirdly that there is an amplification effect whereby one accreditation decision may allow the delivery of many educational activities and fourthly that there is an inherent efficiency in provider accreditation in which the amount of accreditation energy expended in relation to the educational activities becomes progressively less as the number of provided activities increases.
The authors do not claim to have conducted a scientific comparison between the two types of accreditation, although they support their contentions with data derived from their activities. They leave further comparison to the readers in an implicit challenge to advocates of activity accreditation. The Journal appreciates that this contribution is not a scientific treatise, in which each assertion is based on rigorous analysis of data, but rather represents the informed opinions of two men who have thoughtfully devoted their professional lives to the business of accreditation. Just as experience makes the best CME, so should experience of its accreditation be deserving of our respect and consideration.
Since publication of this paper, we have attempted to assess its impact on the CME community at large. To this end we devised an internet survey and invited providers and accreditors obtained from the European CME Forum database to respond to a series of questions relating specifically to the paper and also to some more general aspects of the provision and accreditation of CME in Europe. We received 66 responses: 47 from Europe, 17 from North America and 2 from Asia/Australasia. Twenty-three were from European specialist societies, 24 from independent/commercial providers and 7 from accreditation agencies.
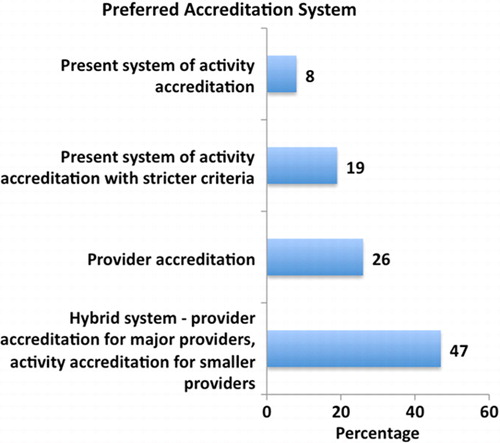
We asked whether respondents agreed with Kopelow and Campbell that provider accreditation encourages providers to improve their performance in a “community of practice” and that provider accreditation has an “inherent efficiency” because of its “amplification effect”; 71% agreed and 29% disagreed. We also asked about preferred accreditation systems; only 8% were happy with the existing activity accreditation, 19% wanted stricter criteria in activity accreditation, 26% advised changing to provider accreditation and a surprising 47% opted for a hybrid system with provider accreditation for major providers and activity accreditation for smaller providers. There was no difference between European and North American responses in relation to preferences about activity accreditation. However 53% of North Americans in contrast to 16% Europeans favoured full provider accreditation, whereas this position was reversed in relation to the hybrid model which was favoured by 58% of Europeans and 18% of North Americans.
In summary, more than two-thirds of respondents agreed with the claims about provider accreditation made in the paper. Almost half favoured the introduction of a hybrid system with provider accreditation for major providers in Europe and only slightly more than a quarter wanted to persist with activity accreditation.
How should Europe react to this paper from North America and to the responses in our survey? There does appear to be support for a change in the practice of European CME accreditation, but the number of respondents in our survey was small and may not be truly representative. The Journal therefore invites the European accreditation agencies to comment on their current policy and to justify continuing with a system which seems to lack popular support in the CME community.