
Abstract
Objective: To describe the incidence of diagnosis of gastroesophageal reflux disease and acid-related conditions (GERD/ARC) throughout childhood and characterize patterns of diagnosis and treatment with proton pump inhibitors (PPIs) and histamine-2 receptor antagonists (H2RAs).
Methods: Cohorts of GERD/ARC children (age 0–18 years) were identified from a large US administrative claims database covering 1999–2005 using ICD-9 codes. Incidence, healthcare utilization (HCU), costs, therapy discontinuation and switching rates were compared between various age and patient groups.
Results: Between 2000 and 2005 annual incidence of GERD/ARC diagnosis among infants (age ≤1 year) more than tripled (from 3.4 to 12.3%) and increased by 30% to 50% in other age groups. Patients diagnosed by GI specialists (9.2%) were more likely to be treated with PPIs compared to patients diagnosed by primary care physician (PCP). PPI-initiated patients doubled (from 31.5% in 1999 to 62.6% in 2005) and, when compared with H2RA-initiated patients, were associated with 30% less discontinuation and 90% less therapy switching in the first month, and with higher comorbidity burden and pre-treatment total HCU and costs when diagnosed by GI specialists.
Limitations: The use of an exploratory definition for GERD/ARC, administrative claims data and potential coding errors in diagnosis codes used in selection process may limit the generalizability of the results.
Conclusions: GERD/ARC incidence increased for children of all ages between 2000 and 2005. PCPs made the majority of diagnoses. PPI initiations have now surpassed H2RA initiations.
Introduction
Symptoms of gastroesophageal reflux (GER) are common during infancy and childhoodCitation1,2 and include regurgitation, heartburn, epigastric pain, and respiratory difficultiesCitation3. Frequent regurgitation alone affects over half of newbornsCitation1, but generally resolves with age, affecting fewer than 5% of children after their first yearCitation1,2. However disruptive GER symptoms may constitute GER disease (GERD)Citation3.
Despite the high prevalence of pediatric GER symptoms, the frequency of pediatric GERD diagnosis has not been widely studied. The prevalence of GER varies substantially depending on age and symptomCitation1,2. For the prevalence of GERD, however, little is known. Chitkara et alCitation4 estimate the annual incidence of GERD among children aged less than 5 years to be 0.09%. Anecdotal evidence suggests that the incidence of diagnosis of GERD is increasing among children, and increasing rates of GERD have been documented in hospitalized infantsCitation5. These trends parallel a more thoroughly documented increase in GERD diagnoses among adultsCitation6.
The goal of treatment for pediatric GERD/acid- related conditions (ARC) is to eliminate symptoms, allow healing of esophageal mucosa and prevent or manage complicationsCitation3. Pharmacological therapies for the treatment of GERD/ARC include promotility agents (metoclopramide and bethanechol) and acid suppression with histamine-2 receptor antagonists (H2RAs) or proton pump inhibitors (PPIs). Promotility agents are not recommended for routine use. Both H2RAs and PPIs have been shown to be efficacious in children and are widely prescribed in pediatric practiceCitation3,7. However, no evidence-based guidance is available regarding the choice between H2RAs and PPIs, and patterns of H2RA and PPI use in infants and children have not been fully characterized. Pediatric PPI prescriptions for all indications have risen sharply in recent years, quadrupling for infants between 2000 and 2003Citation8 and tripling for children aged 12–17 years between 1997 and 2000Citation9. However, the extent to which this increase in pediatric PPI prescriptions represents an increasing preference for PPIs over H2RAs, as described in adultsCitation10, versus an increasing incidence of the diagnosis of pediatric GERD/ARC remains unclear.
Using an administrative claims database, the present study examines: (1) the incidence of diagnosis of pediatric GERD or acid-related conditions (ARC) across age groups and over time between 2000 and 2005, and (2) diagnosis and treatment patterns of pediatric GERD/ARC patients between 1999 and 2005. Pre-diagnosis demographics, comorbidity profiles and healthcare resource use are also compared between children diagnosed by primary care physicians (PCPs) and those diagnosed by gastrointestinal (GI) specialists. Acid-related conditions is an exploratory category created for this study to ensure that potential ICD-9-CM codes are captured that could potentially be used to diagnose GERD. For the purpose of this study, ‘diagnosis’ refers to the ICD-9-CM diagnosis codes available in the claims data to represent GERD/ARC.
Methods
Data
Study samples of children (aged 0–17 years) were drawn from a HIPAA-compliant, de-identified in-house administrative claims database, which includes over 5 million lives (of which approximately 1.2 million were under 18 years of age) from 31 large, privately-insured companies across the US. The businesses of these Fortune 500 companies span a wide spectrum of industries, including financial services, energy, telecommunications, and food and beverages. Beneficiaries include employees, retirees, spouses and dependents. The database contains information on all beneficiaries’ demographics, monthly enrollment history, medical service utilization, and prescription drug dispenses available from 1999 through 2005. All visits to medical professionals (i.e., doctors, nurse practitioners, physician assistants, etc.) are included. While this database does not contain Medicaid claims it is a large dataset that is well representative of the population. Different samples of children were selected for the study of (1) incidence rates to examine the occurrence of selected ICD-9 codes that represent pediatric GERD/ARC, (2) diagnosis patterns to identify what physician specialties were involved in the diagnosis of GERD/ARC in pediatric population, and (3) treatment patterns uses to treat pediatric GERD/ARC.
Incidence rates analysis: sample selection criteria
Annual incidence rates of GERD/ARC were calculated for each year between 2000 and 2005. To be included in the incidence rate calculation for a particular year children were required to be (a) younger than 18 years of age in the year in question, (b) continuously enrolled in their health plans for at least the entire year in question, and (c), for children older than 1, to be continuously enrolled in their health plan and free of GERD/ARC diagnosis during the 6 months prior to the year in question (washout period). To calculate the annual incidence rate, the individuals meeting all selection criteria above during calendar years and age groups of interest were first identified (denominator). Then, for each year–age-group combination of interest, the incidence rate was defined as the number of such individuals who had been diagnosed with GERD (numerator) divided by the denominator. The defining list of ICD-9 codes for GERD/ARC was developed based on discussions with experts in pediatric GERD. Because there were multiple potential codes for GERD/ARC only those that were highly specific for the intent to diagnose a child with GERD/ARC were included. The ICD-9 codes for GERD included 530.81 (Esophageal reflux) and for ARC 530.1x (Esophagitis), 535.xx (Gastritis and duodenitis), 787.1 (Heartburn) and 789.06 (Epigastric pain).
Diagnosis patterns analysis: sample selection criteria and diagnosis definition
Children included in the diagnosis pattern analysis were required to be (a) younger than age 18 years at the time of receiving their first diagnosis of GERD/ARC symptoms (index date), (b) diagnosed by a PCP (family practice, internal medicine, general preventive medicine and pediatrician) or a GI specialist (gastroenterologist and pediatric gastroenterologist), and (c) continuously enrolled in their health plan for the 6 months prior to the index date (pre-diagnosis baseline period).
Treatment patterns analysis: sample selection criteria and pattern definitions
Prescriptions for H2RAs (cimetidine, famotidine, nizatidine, ranitidine) and PPIs (esomeprazole, lansoprazole, omeprazole, pantoprazole, rabeprazole) were identified based on 9-digit National Drug Codes (NDC). Children with initial prescriptions for an H2RA or PPI were identified irrespective of the dosage form (e.g., tablets, melt tablets). The index date and the index therapy were defined to be the date and type (H2RA or PPI) of the initial therapy. To be included in the analyses, children must have (a) been continuously enrolled in their health plans during the 6 months prior to the index date (the pre-treatment baseline period), (b) been continuously enrolled during the 6 months following the index date (the study period), (c) received a GERD/ARC diagnosis during either the pre-treatment baseline period or the month following the index date, (d) been free of H2RA or PPI prescriptions during the pre-treatment baseline period and (e) been free of combination H2RA-PPI prescriptions within 1 week following the index date.
Discontinuation of index therapy was defined as a supply gap of 30 or more days of the index drug (H2RA or PPI). Among patients discontinuing their index therapy, therapy switching was defined as receiving a drug from the alternative class (i.e., changing from PPI to H2RA or vice versa) within 14 days following the last supply day of index drug prior to discontinuation.
Baseline cost calculations
Drug costs were defined as the costs for all prescription drugs identified using NDC codes (GERD/ARC related or not). Medical costs were defined as all non-drug costs, including inpatient and outpatient hospital visits, physician office visits, emergency room (ER) visits and all lab tests. Total healthcare costs were defined as the sum of drug and medical costs. All of the costs were calculated using the reported payments made by the insurance companies. Other costs such as co-payment, coinsurance or deductibles (e.g., third party costs) were not included in the calculation of costs.
Statistical methods
Incidence Rate Analysis: The annual incidence of the diagnosis of GERD/ARC was computed separately for different age groups in each year. GERD/ARC patients were further classified as to whether they received prescriptions for H2RAs or PPIs during the year of diagnosis.
Diagnosis Patterns Analysis: GERD/ARC patients diagnosed by PCPs were compared to those diagnosed by GI specialists in terms of pre-diagnosis baseline characteristics, including comorbidities, prescriptions for H2RAs or PPIs, healthcare resource use and total healthcare costs. Chi-squared tests were used to compare categorical variables and Wilcoxon rank sum tests were used to compare continuous variables. Among patients free of H2RA or PPI prescriptions during the pre-diagnosis baseline, the proportions prescribed H2RAs or PPIs in the first month following diagnosis were computed for PCPs and GI specialists.
Treatment Patterns Analysis: Rates of discontinuation and switching and median days on index therapy were estimated using the Kaplan–Meier method for patients initiated with H2RAs or PPIs. Using the same methods as in the analysis of diagnosis patterns, patient characteristics measured during the pre-treatment baseline period, including comorbidities, all-cause and GERD-related healthcare utilization and healthcare costs, were compared between H2RA patients and PPI patients. Trends in prescription H2RA vs. PPI use over time were estimated using ordinary least squares (OLS) regression. Logistic regression was used to identify pre-treatment baseline characteristics associated with the use of PPIs vs. H2RAs as the first line therapy in pediatric GERD/ARC patients. All analyses were conducted in SAS Version 9.1 (SAS Institute, Cary, NC, USA).
Results
Incidence rates
The annual incidence of the diagnosis of GERD/ARC increased between 2000 and 2005 for children of all ages (). Infants (ages 0 and 1) experienced the largest increase (262%) from an annual incidence of diagnosis of 3.4% in 2000 to 12.3% in 2005. During the same period, the annual incidence of the diagnosis of GERD/ARC among the other children of different age groups (i.e., 2, 3–5, 6–11 and 12–17), increased by 34% to 50%. Among the children older than age 1, those in the 12–17 group experienced the highest incidence rate (1.26%) in 2005, an increase from 0.94% in 2000. Similar conclusions can be drawn from the analysis of incidence rates of pediatric patients with subsequent prescription treatment with either H2RAs or PPIs ().
Table 1. Annual incidence rate of the diagnosis of GERD/ARC in pediatric patients by age group.
Diagnosis patterns
The majority of the 21,471 children identified with GERD/ARC between 1999 and 2005 were diagnosed by PCPs (90.8%) with the remaining 9.2% diagnosed by GI specialists. Compared to PCP-diagnosed patients, GI specialist-diagnosed patients had a higher prevalence of comorbid symptoms and conditions, used more healthcare resources and incurred higher total healthcare costs at baseline (). The most common co-morbid conditions were abdominal pain (excluding epigastric pain) and pharyngitis. Pre-diagnosis H2RA treatment was more prevalent than PPI treatment in PCP-diagnosed patients (4.3 vs. 2.6%), whereas GI specialist-diagnosed patients were more likely to have baseline use of PPIs than H2RAs (19.1 vs. 15.5%). For patients free of H2RA or PPI prescriptions during the pre-diagnosis baseline period, those diagnosed by a GI specialist were more likely to be prescribed PPIs vs. H2RAs (30 vs. 9%) within the first month following diagnosis whereas those diagnosed by PCPs were less likely to be prescribed PPIs vs. H2RAs (10 vs. 14%).
Table 2. Baseline characteristics of pediatric GERD/ARC patients diagnosed by GI specialists and primary care physicians (PCPs).
Treatment patterns
Of the 9,329 GERD/ARC patients initiated on an H2RA or PPI between 1999 and 2005, 4,729 (50.7%) were initiated on an H2RA. Compared to patients initiated on H2RAs, patients initiated on PPIs () had a significantly higher prevalence of comorbid symptoms and conditions, upper respiratory infections, otitis media and abdominal pain being the most common, during the pre-treatment baseline period and significantly higher healthcare resource use and total healthcare costs ($4,431 vs. $3,887). Between 1999 and 2005, the proportion of PPI patients followed an increasing trend in all age groups (p-value for trend <0.001), with the overall proportion of PPI-initiated patients nearly doubling from 31.5% to 62.6% (). In addition, older patient groups had a higher percentage of PPI use than the younger groups (data not shown).
Figure 1. Distribution of pediatric GERD/ARC patients initiated on H2RAs and PPIs (1999–2005). GERD, gastroesophageal reflux disease; ARC, acid-related conditions; H2RA, histamine-2 receptor antagonists; PPI, proton pump inhibitors.
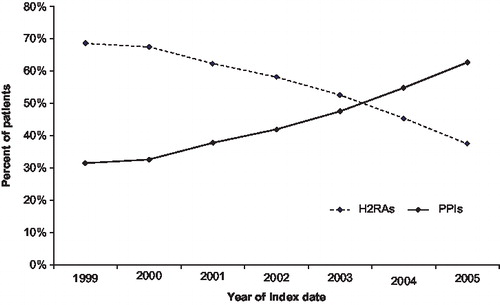
Table 3. Baseline characteristics of pediatric GERD/ARC patients initiated on H2RAs and PPIs.
The median time on index therapy during the first year was also twice as long for patients initiated on PPIs compared to those initiated on H2RAs (). PPI patients were 30% less likely to discontinue the index therapy and 90% less likely to switch during the first month following index therapy initiation.
Table 4. Treatment pattern of pediatric GERD/ARC patients initiated on H2RAs and PPIs.
In a multivariate logistic regression model, initiation with PPIs rather than H2RAs was associated with older age, more recent treatment initiation, asthma, abdominal pain, depression, dysphagia, noncardiac chest pain, underweight, failure to thrive (FTT), absence of GERD-related ER visits, GERD-related outpatient visits, visits to an otolaryngologist or pulmonologist, diagnosis by upper endoscopy and use of promotility agents during the pre-treatment baseline period ().
Table 5. Selected predictors of PPIs vs. H2RAs as first line therapy for pediatric GERD/ARC Patients*,†.
Discussion
Using a large US claims database, this study described an increasing incidence of diagnosis of pediatric GERD/ARC between 2000 and 2005 across all age groups, with the greatest increase occurring among infants. Patients in this study encompass different areas of the country and different types of health insurance and thus the results are representative of the actual pediatric GERD/ARC population in the US. The incidence rates of diagnosis observed in this study are higher than the estimate of Chitkara et alCitation4 for children aged younger than 5 years born between 1976 and 1982. The difference in incidence rates of diagnosis may be explained by several factors.
The broader definition of GERD/ARC used in the present study and the use of only a 6-month washout period to define incident cases of diagnosis of GERD/ARC would be expected to yield higher incidence rates than counting first-ever diagnoses of GERD alone. Given the increasing incidence of diagnosis of GERD/ARC over time, the more current cohort investigated in the present study would be expected to have a higher incidence of diagnosis of GERD/ARC than the historical cohort studied by Chitkara et alCitation4. Finally, the nationwide patient population investigated in the present study is more diverse than the largely Caucasian sample from Rochester, Minnesota, studied by Chitkara et alCitation4.
A limitation of the present study is that diagnosis codes for GERD/ARC could not be validated against clinical records, as in Chitkara et alCitation4. The definition of ARC used in this study is an exploratory category that was defined by the authors for the purpose of this study only. Also, ICD-9 coding can be subjective to the individual doing the actual coding. For example, in clinical practice a child with pain in the upper abdomen might be coded as epigastric pain, GERD, or gastritis depending on the practitioner. Since no tests are usually done it is impossible to know what is, in fact, the true source of the child's pain. The differences in our methodology and patient populations make comparisons with the Chitkara et alCitation4 difficult. Interestingly, both studies found no difference in the incidence of the diagnosis of GERD/ARC between males and females.
The annual incidence rates of diagnosis of pediatric GERD/ARC observed in this study in 2000 (0.6–1.0%) are comparable in magnitude to the 0.45% annual incidence rate for GERD in patients of any age in the UK in 1996Citation11 and the 0.54% annual incidence that can be estimated for Georgia Medicaid patients in 1998 using the data reported by Kotzan et alCitation12. The slightly higher incidence rates of diagnosis observed in this study, compared to patients of any age in 1996 and 1998, are consistent with a higher prevalence of GER symptoms among children compared to adults and with the trend towards increasing rates of GERD diagnosis observed in this study.
Several factors could explain an increasing incidence of pediatric GERD/ARC diagnosis. Awareness of pediatric GERD/ARC may have been increased by marketing campaigns following new labels for pediatric GERD. Given the dramatic increase in the incidence of diagnosis, particularly among infants, it is of concern that some of the increase in GERD/ARC diagnosis may represents over-diagnosis. However, a true modest increase in the incidence of GERD is supported by the world-wide increase in the incidence of Barrett's esophagus and esophageal cancersCitation13,14, both which are thought to be related to GERDCitation15,16. Changes in children's lifestyles, especially an increased intake of fats, sugars, and caffeine from fast food and sodaCitation17, as well as an increasing incidence of childhood obesityCitation18, could contribute to an increased risk of GERD/ARC. It is also possible that some of the increase in GERD/ARC diagnoses could be explained by mis-diagnoses of eosinophilic esophagitis, which is also increasing in incidenceCitation19.
This study found that most infants and children diagnosed with GERD/ARC are diagnosed by PCPs rather than GI specialists. Though a limitation of this study is that prescription treatments for GERD/ARC could not be linked to the prescribing physician's specialty, the preponderance of diagnoses by PCPs suggests that most treatment for GERD/ARC also takes place in a primary care setting. This finding has implications for the design and interpretation of clinical studies of GERD/ARC therapies in pediatrics, as most published studies were conducted in the tertiary care setting.
This study also indicates that less than half of the children identified with GERD/ARC were subsequently prescribed acid-suppression therapy. There is a possibility that these children may be prescribed lifestyle modification or may be using over-the-counter (OTC) H2RAs or PPIs. Such use of OTC H2RAs or PPIs by children may be limited especially since these OTC medications are not labeled for pediatric use. Also, the OTC medications would probably be used by older children since they are generally available only in solid dosage forms which may be difficult for infants and younger children to swallow. Since the present study used claims data the authors could not examine lifestyle modifications and to what extent written prescriptions were not filled or if prescriptions that were actually filled were not consumed.
The increase in PPI prescriptions observed in this study is consistent with the increase described by Barron et alCitation8. The current study further shows that the increase in pediatric PPI prescriptions is due to two trends: an increasing incidence of diagnosis of pediatric GERD/ARC treated with acid-suppression therapy and an increasing preference for prescription PPIs vs. H2RAs. The increase use in PPIs in infancy is surprising since PPIs are not FDA approved in this age group and recent infant placebo-controlled trials have not be able to demonstrate efficacy.
The majority of pediatric prescriptions for acid suppression therapy observed in this study were continued for less than 2 months, with patients initiated on H2RAs tending to discontinue earlier than patients initiated on PPIs. Longer treatment durations with PPIs could arise from PPI patients being generally sicker, in terms of having a higher comorbidity burden and higher healthcare resource utilization at baseline. The durations of use for both PPI and H2RA treatment observed among pediatric patients in this study are much shorter than durations of use reported in adultsCitation20.
Conclusion
The annual incidence of diagnosis of GERD/ARC diagnosis increased for children of all ages between 1999 and 2005, more than tripling among infants, with the majority of diagnoses made by PCPs. Initiation of prescription therapy with PPIs has become increasingly common for pediatric GERD/ARC, and is now more common than initiation with prescription H2RAs.
Acknowledgment
Declaration of interest: This study was sponsored by Takeda Pharmaceuticals North America, Inc., Deerfield, IL, USA.
S.P.N. has disclosed that she is on the Speakers’ Bureau and serves as a consultant for Takeda Pharmaceuticals North America; S.K. and O.H.D. have disclosed they are employed by Takeda Pharmaceuticals North America; E.Q.W., J.M.M. and N.B. have disclosed they are employed by Analysis Group, Inc. and received consulting fees from Takeda Pharmaceuticals North America.
References
- Nelson SP, Chen EH, Syniar GM, Prevalence of symptoms of gastroesophageal reflux during infancy – A pediatric practice-based survey. Arch Pediatr Adolesc Med 1997;151:569-72.
- Nelson SP, Chen EH, Syniar GM, Prevalence of symptoms of gastroesophageal reflux during childhood – A pediatric practice-based survey. Arch Pediatr Adolesc Med 2000;154:150-4.
- Rudolph CD, Mazur LJ, Liptak GS, Guidelines for evaluation and treatment of gastroesophageal reflux in infants and children: Recommendations of the North American Society for Pediatric Gastroenterology and Nutrition. Pediatr Gastroenterol Nutr 2001(Suppl 2):S1-31.
- Chitkara DK, Talley NJ, Weaver AL, Incidence of presentation of common functional gastrointestinal disorders in children from birth to 5 years: a cohort study. Clin Gastroenterol Hepatol 2007;5:186-91.
- Callahan CW. The diagnosis of gastroesophageal reflux in hospitalized infants: 1971-1995. J Am Osteopath Assoc 1998;98: 32-4.
- El-Serag HB, Richardson P, Pilgrim P, Determinants of gastroesophageal reflux disease in adults with a history of childhood gastroesophageal reflux disease. Clin Gastroenterol Hepatol 2007;5:696-701.
- Colletti RB, Di Lorenzo C. Overview of pediatric gastroesophageal reflux disease and proton pump inhibitor therapy. J Pediatr Gastroenterol Nutr 2003;37(Suppl 1):S7-11.
- Barron JJ, Tan H, Spalding J, Proton pump inhibitor utilization patterns in infants. J Pediatr Gastroenterol Nutr 2007;45:421-7.
- Scott Levin & Associates. IMS American prescription audit. Newton, PA: Scott Levin Audit, 2000.
- Martin RM, Lim AG, Kerry SM, Trends in prescribing H-2-receptor antagonists and proton pump inhibitors in primary care. Aliment Pharmacol Ther 1998;12:797-805.
- Ruigomez A, García Rodríguez LA, Wallander MA, Natural history of gastro-oesophageal reflux disease diagnosed in general practice. Aliment Pharmacol Ther 2004;20:751-60.
- Kotzan J, Wade W, Yu HH. Assessing NSAID prescription use as a predisposing factor for gastroesophageal reflux disease in a Medicaid population. Pharm Res 2001;18:1367-72.
- Blot WJ, Devesa SS, Kneller RW, Rising incidence of adenocarcinoma of the esophagus and gastric cardia. JAMA 1991;265:1287-9.
- Devesa SS, Blot WJ, Fraumeni JF. Changing patterns in the incidence of esophageal and gastric carcinoma in the United States. Cancer 1998;83:2049-205.
- Lagergren J, Bergstrom R, Lindgren A, Symptomatic gastroesophageal reflux as a risk factor for esophageal adenocarcinoma. N Engl Med 1999;340:825-31.
- Lieberman DA, Oehlke M, Helfand M. Risk factors for Barrett's esophagus in community-based practice. Am J Gastroenterol 1997;92:1293-7.
- Bowman SA, Gortmaker SL, Ebbeling CB, Effects of fast-food consumption on energy intake and diet quality among children in a national household survey. Pediatrics 2004;113:112-18.
- Ogden CL, Flegal KM, Carroll MD, Prevalence and trends in overweight among US children and adolescents, 1999-2000. JAMA 2002;288:1728-32.
- Noel RJ, Rothenberg ME. Eosinophilic esophagitis. Curr Opin Pediatr 2005;17:690-4.
- Van Soest EM, Siersema PD, Dieleman JP, Persistence and adherence to proton pump inhibitors in daily clinical practice. Aliment Pharmacol Ther 2006;24:377-85