
Abstract
Objectives:
The Nippon Ultra-Rapid Insulin and Diabetic Complication Evaluation Study (NICE Study) (NCT00575172) was a 5-year, open-label, randomised controlled trial which compared cardiovascular outcomes in Japanese type 2 diabetes patients intensively treated with regular human insulin or insulin aspart (NovoRapid; Novo Nordisk A/S, Bagsværd, Denmark), a rapid-acting insulin analogue. The aim of the present analysis was to evaluate the cost effectiveness of insulin aspart versus regular human insulin from the perspective of a Japanese third-party healthcare payer.
Research design and methods:
A discrete event-simulation model was developed in Microsoft Excel to assess the within-trial cost effectiveness and make longer-term clinical projections in patients treated with regular human insulin or insulin aspart. In addition to severe hypoglycaemia, the model captured myocardial and cerebral infarction events and percutaneous coronary intervention and coronary artery bypass graft procedures. Within-trial mortality, incidence of severe hypoglycaemia and cardiovascular event probabilities were derived from the annual rates observed during the trial period, while post-trial outcomes were calculated using the event rates from the trial, adjusted for increasing patient age. Event costs were accounted from the healthcare payer perspective and expressed in 2008 Japanese yen (JPY), while health-related quality of life (HRQoL) was captured using event and state utilities. Future costs and clinical benefits were discounted at 3% annually. Life expectancy, quality-adjusted life expectancy, cardiovascular event rates and costs were evaluated over 5- and 10-year time horizons and sensitivity analyses were performed to assess variability in model outcomes.
Results:
Over 5 years of treatment, insulin aspart dominated human insulin both in incremental life expectancy and in incremental quality-adjusted life-years (QALYS). Insulin aspart was associated with a small improvement in discounted life expectancy of 0.005 years (4.688 vs. 4.684 years) and an increase of 0.023 quality-adjusted life-years (QALYs) (3.800 vs. 3.776 QALYs) when compared with regular human insulin. Insulin aspart also incurred lower costs (JPY 481,586 vs. 594,717, difference −113,131) which resulted from the decreased incidence of cardiovascular events with insulin aspart (0.013 events per patient year vs. 0.030 on regular human insulin). Breakdown of costs indicated that pharmacy costs were higher with insulin aspart (JPY 346,608 vs. 278,468), but these costs were more than offset by the reduced costs associated with cardiovascular complications and hypoglycaemia over 5 years of treatment (JPY 134,978 vs. 316,249). Sensitivity analysis showed that insulin aspart was still cost-effective in the case where only 18% of the within-trial cardiovascular and mortality benefit over regular human insulin was captured in the model (assuming a willingness-to-pay threshold of JPY 5,000,000).
Limitations:
The NICE study cohort was relatively small (n = 325), meaning that caution should be exercised when calculating and interpreting the incremental cost-effectiveness ratio. Also, despite the differences in cardiovascular risk profile between the Japanese and UK populations, UKPDS-derived risk equations were used to project MI outcomes and PCI and CABG procedures and UKPDS HRQoL scores were applied to all health states. While these risk formulas and HRQoL utilities may not be directly applicable to the Japanese population, no equivalent Japanese-specific data are currently available.
Conclusions:
In a Japanese type 2 diabetes population, prescribing rapid-acting insulin aspart significantly reduced cardiovascular complications over 5- and 10-year time horizons, resulting in increased quality of life and decreased costs when compared with human insulin.
Introduction
Type 2 diabetes is a metabolic disorder that is associated with considerable clinical and economic burden. The condition is linked with a wide range of comorbidities, including stroke, myocardial infarction, sensory neuropathy, macrovascular mortality and all-cause mortalityCitation1–10. The majority of these complications are, in turn, associated with a considerable economic burden, both in terms of direct medical costs and indirect costs arising from premature mortality and lost productivity. In Japan, estimates placed the prevalence of type 2 diabetes at 6.9% in 2003, a figure that is expected to rise to 7.9% by 2025Citation11, while a recent study found the prevalence of undiagnosed diabetes to be 6.4% in males and 3.2% in femalesCitation12. Given the relatively low prevalence of type 1 diabetes in Japan, the vast majority of these undiagnosed patients are also likely to have type 2 diabetesCitation13. There is a relative paucity of data regarding the economic burden of diabetes in the Japanese setting, but a number of studies placed the total diabetes-related expenditure between 4% and 6% of the country’s healthcare budgetCitation14–16. This compares with an estimated 12% of healthcare expenditure globallyCitation17.The primary goal of diabetes management is to slow or prevent the onset or progression of these complications. Many recent studies, such as Steno-2, the Collaborative Atorvastatin Diabetes Study (CARDS), the Hypertension Optimal Treatment (HOT) study and the Heart Outcomes Prevention Evaluation (MICRO-HOPE), have indicated that a multifactorial approach to treatment including, for example, oral antidiabetics, antihypertensives and statins, is beneficial in terms of reducing complications and controlling the disease. However, diabetes is a chronic, progressive disease and even with this multi-faceted approach, patients ultimately require insulin to improve glycaemic control.
In 1985, a meeting held jointly by the World Health Organization (WHO) and the Juvenile Diabetes Foundation International concluded that there was a need to research new insulin formulations that would exhibit an improved pharmacokinetic profile to better match the insulin secretion profile that is observed post-prandially in non-diabetic individualsCitation18. This recommendation led to the development and approval of insulin lispro and subsequently insulin glulisine and aspart, all of which belong to a class known as the rapid/short-acting insulin analogues (SAIAs). Insulin aspart is an analogue with a proline to aspartic acid substitution at position 28 of the B chain that causes the rapid dissociation of insulin hexamers into monomers and dimers upon administrationCitation19. As a result, insulin aspart is absorbed more quickly and reaches higher peak plasma concentrations within approximately half the time when compared with regular human insulinCitation20,Citation21.
Since the pharmacokinetic properties of the SAIAs appear to be highly desirable, the clinical benefits over regular human insulin have been the focus of numerous studies. In 2006, a comprehensive meta-analysis of 49 studies (including 8,274 patients) was conducted by Siebenhofer et al. on behalf of the Cochrane CollaborationCitation22. The study showed SAIAs to be equivalent with human insulins in terms of HbA1c and overall hypoglycaemic events, and superior in terms of severe hypoglycaemic events (in type 2 diabetes patients). Although the study concluded that the SAIAs demonstrated only a minor overall clinical benefit, the authors noted that the vast majority of the included studies were of poor methodological quality and that further research, based on long-term efficacy and safety studies, was required. Furthermore, in the context of the present analysis, it should be noted that, of the studies included in the meta-analysis, only one was conducted in the Japanese setting.
The Nippon Ultra-Rapid Insulin and Diabetic Complication Evaluation-Study (NICE study; ClinicalTrials.gov number, NCT00575172) was a 5-year, open-label, randomised controlled trial which compared cardiovascular outcomes in Japanese type 2 diabetes patients intensively treated with short-acting regular human insulin (n = 162) or insulin aspart (n = 163)Citation23. Where necessary, intermediate- or long-acting insulin was also used as part of a basal bolus regimen (at baseline, this was the case in 42% of patients randomised to the regular human insulin arm and 40% of patients in the insulin aspart arm). The primary endpoint of the trial was a composite cardiovascular endpoint comprising myocardial infarction (MI), angina pectoris, cerebral infarct/transient ischaemic attack (TIA), coronary artery bypass graft (CABG) or percutaneous coronary intervention (PCI). Secondary endpoints included HbA1c, post-prandial glucose and fasting plasma glucose concentrations. The study showed a 43% reduction in incidence of the composite endpoint in patients on insulin aspart when compared with those on regular human insulin (6.4% or 12.8/1000/year vs. 11.3% or 22.2/1000/year, respectively, p < 0.02). With regard to secondary endpoints, no statistically significant difference was observed in HbA1c (7.5 ± 0.7 vs. 7.5 ± 0.7%, respectively) or fasting plasma glucose (128 ± 42 vs. 133 ± 54 mg/dl, respectively). However, a significant decrease in 90-minute postprandial glucose was observed in patients on insulin aspart relative to those on regular human insulin (142 ± 58 vs. 226 ± 48 mg/dl, p < 0.02).
The aim of the present study was to assess the cost effectiveness of insulin aspart versus regular human insulin from the perspective of a third-party healthcare payer in the Japanese setting based on the outcomes observed in the NICE study.
Methods
Model
A discrete-time cohort-level cost-effectiveness model with an annual cycle length was created in Microsoft Excel. The model comprised two temporally distinct sections, the first of which calculated within-trial outcomes based on complication incidence, mortality and cost data from the NICE trial. The second model section made post-trial projections using the trial outcomes as a baseline for progression formulas from the United Kingdom Prospective Diabetes Study (UKPDS) and a 2007 white paper on hypertension and strokeCitation24,Citation25.
Within-trial outcomes were calculated by associating costs and utilities with the events observed in the NICE study ( and , respectively). The mean number of at-risk patients in each year of the NICE study was then combined with the event incidence, utility and cost data to calculate per-patient cost and effectiveness outcomes for each arm. Similarly, within-trial mortality was modelled based on mortality data from the NICE study. Half-cycle corrections were applied to eliminate any systematic over- or under-estimation of model outcomes.
In the absence of cardiovascular risk data in a Japanese diabetes population, post-trial MI incidence was modelled using the UKPDS MI cumulative incidence formulaCitation11,Citation26, populated with the baseline physiological parameters of the NICE study cohort (). Baseline MI risk was calculated using the mean rate of MI over the duration of the entire NICE study. The UKPDS formula was used to calculate the cumulative incidence of MI in each year of the simulation. The quotient of the present year’s cumulative incidence and the previous year’s cumulative incidence was then applied as an annual multiplier to the baseline risk. The progression of incidence of MI was then used as a surrogate to model the annual increase in incidence of PCI and CABG procedures, using the incidence of within-trial procedures as the baseline in each case. Post-trial incidence of cerebral infarction was calculated using a straightforward model in which the probability of an event was assumed to double every 10 years (in patients aged 55 and over)Citation25. The risk of cerebral infarction (relative to that observed in each arm of the NICE study) in year t after conclusion of the study was therefore represented by (20.1)t. Rates of severe hypoglycaemia were assumed to remain constant (at the end-of-study rate) for the duration of the extrapolation period. Post-trial mortality was modelled by calculating annual risk multipliers from age-indexed and gender-weighted Japanese life tables from the World Health Organization (using the same technique as that employed with the UKPDS risk formula)Citation27. Mortality risk multipliers were then applied to the mean annual mortality observed during the NICE study. The data sources used to calculate event incidence rates in the within-trial and post-trial sections of the model are summarised in .
Figure 1. Data sources for event incidence over the model time horizon.
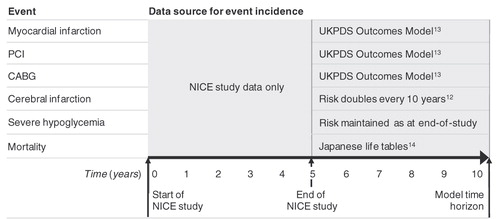
Table 1. Baseline cohort characteristics from the NICE study.
Baseline cohort characteristics from the NICE study population were used in the post-trial simulation (). Mean values from all patients were used (although there were no statistically significant differences between patients in the regular human insulin and insulin aspart arms in terms of baseline demographics, physiology or concomitant therapies). It should be noted that, from a modelling perspective, the cohort characteristics only affect post-trial projections, as the within-trial portion of the model was based exclusively on the cardiovascular events and mortality reported from the NICE study.
Perspective, time horizon and discounting
The base-case analyses were performed over 5 and 10-year time horizons from the perspective of a third-party healthcare payer in Japan. The payer perspective was selected on the grounds that there is currently no apparent consensus in the Japanese health economic literature on whether a payer or societal perspective is most acceptedCitation28–31. A pragmatic literature search revealed that the majority of previous cost-effectiveness analyses in the Japanese setting had been performed from the payer perspective, indicating that the societal perspective is perhaps less well established. The 5-year outcomes are based exclusively on the outcomes observed in the NICE study, while the 10-year outcomes add 5 years of post-trial projection as described above. Given the relatively low event rates observed in the NICE study, modelling beyond a 10-year time horizon was considered unjustifiable. In line with previous health economic analyses in the Japanese setting, all future costs and clinical outcomes (those incurred or accrued in year 2 and onwards) were discounted at a rate of 3% annuallyCitation28–31. To simplify the calculation of patient co-payment in the Japanese setting, it was assumed that all patients contributed 30% of costsCitation32.
Costs
With the exception of severe hypoglycaemia, adverse events costs were derived from hospital receipt data supplied by the Japanese Medical Data Centre in 2008 Japanese yen (JPY) and are presented in . In the absence of cost or resource-use estimates for severe hypoglycaemia in the Japanese setting, a value of €239 was used from a 2008 study into the cost of severe hypoglycaemia in Spain by Reviriego and colleaguesCitation33. This value was converted to JPY using the mid-2008 exchange rate of 167.6 yen to the euro (mid-market rate from Citibank, N.A.)Citation34.
Table 2. Event and pharmacy costs used in the modelling analysis.
Insulin usage was taken from the trial and per-unit insulin costs were supplied by Novo Nordisk Japan (). Total daily bolus doses of regular human insulin and insulin aspart were conservatively calculated based on insulin usage at the end of the NICE study, at which point insulin aspart dosage was significantly higher than regular human insulin (34.8 and 28.4 units per day, respectively). In the absence of basal insulin use data in every year of the NICE Study, daily doses (and the proportion of patients taking basal insulin) were assumed to increase linearly over the duration of the NICE study (from the baseline dose to the dose at the end of the study). In the insulin aspart arm, the mean daily dose increased from 12.2 units per day (in 40% of patients) at the start of the study to 14.6 units per day (in 56% of patients) at end of study. In the regular human insulin arm, the proportion of patients taking basal insulin remained constant, but the mean daily dose increased from 12.6 units to 14.2 units over the course of the study. Costs of concomitant medications such as oral antidiabetics, antihypertensives, antithrombotics and antihyperlipidaemics were not accounted as inter-arm differences in medication use were not statistically significant in the NICE study (and hence would have no direct impact on incremental outcomes).
Estimation of quality-adjusted life expectancy
To account for the effect of cardiovascular events on health-related quality of life (HRQoL) (and in the absence of local HRQoL scores for diabetes patients), health utilities from the UKPDS were applied to all patients in the model. The baseline utility for patients with complication-free diabetes was taken to be 0.814, a value based on tobit regression analysis of 3,192 responses to the EuroQol EQ-5D quality of life instrumentCitation35. For patients experiencing MI or cerebral infarction, distinct utilities were applied in the year of the event and years subsequent to the event (). Patients who underwent CABG or PCI were assumed to have the same quality of life as diabetes patients with no complications (previous studies suggest that HRQoL may initially increase after CABG or PCICitation36–38 although none of these studies have focused specifically on outcomes in diabetes patients). Severe hypoglycaemia was associated with a disutility of −0.0118 in the year of the eventCitation39. No subsequent state disutility was applied.
Table 3. Quality of life utilities.
Sensitivity analyses
To assess the sensitivity of model outcomes to changes in input parameters, a series of one-, two- and multi-way sensitivity analyses were performed around the 5-year base case, including analyses around discounting, pharmacy and complication costs, HRQoL utilities and the efficacy of insulin aspart relative to regular human insulin. To address uncertainty in the NICE study outcomes, a series of the efficacy-based sensitivity analyses were used to form a break-even analysis, in which the cardiovascular and mortality event rates in the insulin aspart arm were increased in increments of 20% of the difference between the rates observed in the insulin aspart and regular human insulin arms of the NICE study. In turn, these outcomes were used to plot a net health benefit chart, assuming a willingness-to-pay (WTP) threshold of JPY 5,000,000/QALYCitation40. Net health benefit is a means by which the outcomes of a cost-effectiveness analysis (i.e., incremental cost and effectiveness) are combined and expressed as a single measure (in this case incremental quality-adjusted life expectancy). In the present analysis, the incremental cost with insulin aspart (relative to human insulin) was converted to an equivalent quality-adjusted life expectancy value using the WTP threshold. This (negative) value was then subtracted from the projected incremental quality-adjusted life expectancy to give the total net health benefit in QALYs (ΔQALE – ΔCost/WTP).
Additional sensitivity analyses were performed around the cost of complications and procedures. Where 95% confidence intervals were available for costs (which was the case for MI, CI, CABG and PCI), analyses were performed with the costs set to the highest and lowest bounds of the confidence intervals. As confidence intervals were not available for the cost of severe hypoglycaemia, three additional analyses were performed in which the cost of all complications was set to JPY 0, 50% of the base case and 200% of the base case. The effect of discounting was explored in two analyses, which used values of 0% and 6% for cost and clinical discounting. Two sensitivity analyses were performed around HRQoL utilities, the first of which investigated the effect of setting all utilities to 0.814 (the base-case utility for complication-free type 2 diabetes) and the second of which explored the effect of increasing the utilities associated with CABG and PCI to 105% of that in the base case (0.855).
Finally, sensitivity analyses were performed around MI and CI incidence rates, setting the rates in the regular human insulin arm to the same as those in the insulin aspart arm.
Results
Clinical outcomes
Over the 5-year duration of the NICE study, the incidence of all adverse cardiovascular events was lower in patients on insulin aspart than those on regular human insulin (0.013 vs. 0.030 events per patient year). Insulin aspart was also associated with a small improvement in discounted life expectancy of 0.005 years compared to human insulin (4.688 vs. 4.683 years) and an additional 0.023 quality-adjusted life-years (QALYs) (3.800 vs. 3.776 QALYs).
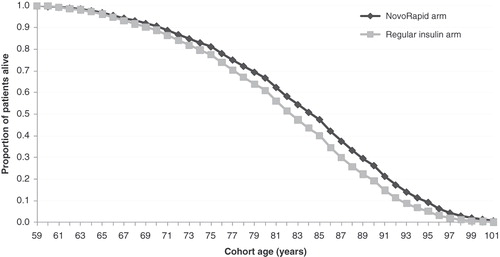
Over a 10-year period, insulin aspart was found to be associated with an improvement in discounted life expectancy of 0.043 years (8.546 vs. 8.503 years) and an improvement in quality-adjusted life expectancy of 0.062 QALYs (6.942 vs. 6.879 QALYs). A survival curve showing the proportion of patients alive over a 40-year time horizon is presented in . The curve shows separation between the insulin aspart and regular human insulin arms after a mean age of 65 years.
Figure 2. Survival curve showing proportion of patients alive in the insulin aspart and regular human insulin arms.
Cost and cost effectiveness
Over the duration of the NICE study, insulin aspart was found to be cost saving (JPY 481,586 vs. 594,717, difference −113,131) when compared with human insulin (). Pharmacy costs in the insulin aspart arm were greater (JPY 346,608 vs. 278,468, an increase of JPY 68,140), but these were more than offset by a reduction in costs associated with cardiovascular complications over 5 years of treatment (JPY 134,978 vs. JPY 316,249, a reduction of JPY 181,271). Insulin aspart was therefore found to be the dominant option, reducing costs, CVD events and severe hypoglycaemia and thereby increasing quality-adjusted life expectancy.
Table 4. Within-trial and post-trial cost and effectiveness outcomes.
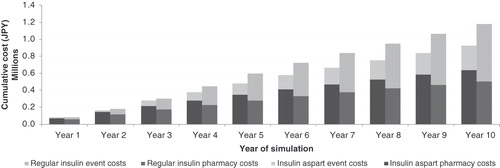
Over a 10-year time horizon (including the trial period), insulin aspart was projected to save an average of JPY 252,923 (incurring costs of JPY 926,472 per patient vs. JPY 1,179,395 in the regular human insulin arm). As in the exclusively in-trial analysis, pharmacy costs were found to be higher (JPY 638,269 vs. JPY 506,817, difference JPY 131,453), but were again more than offset by cost savings resulting from a reduced incidence of cardiovascular complications (JPY 288,203 vs. JPY 672,578, difference JPY −384,376). Insulin aspart was therefore dominant compared with regular human insulin. A bar chart showing the cumulative costs in each year of the model is presented in .
Figure 3. Pharmacy and event costs in the insulin aspart and regular human insulin arms over a 10-year time horizon.
Sensitivity and break-even analyses
Outcomes of sensitivity analyses and the break-even analysis are presented in and . The break-even analysis showed that insulin aspart was dominant even in the case where only 29% of the cardiovascular and mortality benefit from the NICE study were accounted in the model. Furthermore, the net health benefit chart () showed insulin aspart to remain cost-effective down to only 18% of the benefit observed in the NICE study (given a willingness-to-pay threshold of JPY 5,000,000). Other sensitivity analyses showed that model outcomes were not sensitive to any one input parameter, with insulin aspart remaining dominant in all cases except for that in which all complication costs were set to JPY 0, where the ICER was found to be JPY 2,947,310/QALY gained.
Figure 4. Break-even analysis showing (A) incremental costs, (B) net health benefit and (C) incremental QALE over a range of the observed cardiovascular and mortality benefits of insulin aspart when compared with regular human insulin (over a 5-year time horizon).
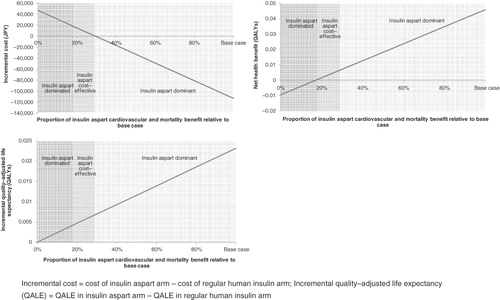
Table 5. Sensitivity analyses (5-year base case).
Discussion
Based on the results of the NICE study, insulin aspart significantly reduced the incidence of cardiovascular complications and severe hypoglycaemia over 5- and 10-year time horizons, resulting in increased life expectancy and quality of life and decreased costs when compared with human insulin. The reduction in cardiovascular event rates in the insulin aspart arm of the NICE study was of particular interest, as statistically significant reductions in cardiovascular complications have not been widely observed in previous studies comparing SAIAs with regular human insulin. Also of note is that inter-arm differences in HbA1c and fasting plasma glucose (FPG) were not statistically significant at end-of-study, corroborating prior evidence that HbA1c and FPG may not be optimal indicators or predictors of cardiovascular risk in diabetes patients, as noted in previous SAIA versus regular human insulin studiesCitation41.
The reduction in incidence of the composite cardiovascular endpoint (12.8/1000/year vs. 22.2/1000/year in the insulin aspart and regular human insulin arms, respectively; p < 0.02) should be interpreted in the context of the Japanese population, which has a markedly different cardiovascular risk profile from Western populationsCitation42. The fact that such reductions have not been widely observed previously may be due to the emphasis on Western populations in the vast majority of studies and meta-analyses investigating outcomes in SAIA-treated patients to-date. For example, of the 49 studies included in the Siebenhofer et al. meta-analysis, only one was based in the Japanese settingCitation43.
The only physiological endpoint recorded in the NICE study that showed a significant inter-arm difference at end-of-study was mean 90-minute post-prandial glucose (PPG) concentration, which was significantly lower with insulin aspart than regular human insulin (142 ± 58 vs. 226 ± 48 mg/dl, respectively, p < 0.02). A link between decreased PPG and lower cardiovascular risk has been reported in previous studiesCitation44,Citation45. Indeed, a number of such studies have noted that progression of cardiovascular risk is more closely correlated with PPG excursions than either FPG or HbA1c Citation46,Citation47. The increase in cardiovascular risk associated with acute hyperglycaemic episodes may result from vascular inflammation caused by hyperglycaemia-induced production of proinflammatory cytokines such as tumour necrosis factor-alpha, interleukin (IL)-6, IL-1 beta, and IL-8Citation48. The increase in cytokine production has been found to be mitigated by infusion of insulin and subsequent return to normoglycaemia, providing a potential physiological explanation for the risk reduction observed in the NICE study, in which insulin aspart patients experience fewer and less severe glycaemic spikesCitation28. From an economic perspective, the costs and HRQoL utilities associated with cardiovascular complications are such that even a relatively small reduction in risk has a dramatic effect on incremental cost and effectiveness outcomes.
The present study has a number of limitations that should be acknowledged. Firstly, the size of the cohort in the NICE study was relatively small (n = 325). As previous studies have noted, caution should be exercised when calculating and interpreting incremental cost-effectiveness ratios in such small populations, especially when statistical uncertainty data are unavailableCitation49. However, the break-even analysis and net health benefit chart presented in attempt to address these concerns by modelling a range of reduced cardiovascular and mortality benefits for insulin aspart versus regular human insulin. The analysis showed that, even with a 71% reduction in the adverse event and mortality rate benefits observed in the trial, insulin aspart would remain dominant over regular human insulin and would still be cost effective after an 82% reduction. Secondly, in the absence of local data, UKPDS HRQoL scores were applied to all health states. To evaluate the influence of utility scores associated with complications, a sensitivity analysis was performed where no changes in utility were applied when complications occurred (i.e., all patients had a utility score of 0.814 regardless of complication status). As a result of the increased mortality in the regular human insulin arm, insulin aspart remained dominant in this analysis, although the inter-arm difference in quality-adjusted life expectancy fell to 0.0037 (from 0.0231 in the base case). Finally, despite the differences in cardiovascular risk profile between the Japanese and UK populations, UKPDS-derived risk formulas were used to project MI outcomes and PCI and CABG procedures. While these risk formulas may not be directly applicable to the Japanese population, no equivalent Japanese-specific data are currently available. It should also be noted that these formulas only affect the post-trial projection section of the model, not the within-trial section (in which all cardiovascular event, hypoglycaemia and mortality data were taken directly from the NICE study).
Conclusion
The NICE study was the first study to focus specifically on cardiovascular risk in Japanese patients taking SAIAs. The findings showed a 43% reduction in incidence of the composite endpoint (MI, angina pectoris, CI/TIA, CABG or PCI) in patients on insulin aspart when compared with those on regular human insulin. However, given the unique cardiovascular profile of the Japanese population, future large-scale, long-term randomised controlled trials investigating cardiovascular outcomes in Japanese diabetes patients would be a welcome addition to the current evidence base. While the health economic outcomes of this analysis should be interpreted in the appropriate context, the evidence suggests that insulin aspart was both cost- and life-saving even when only 29% of the observed cardiovascular benefit was captured in the modelling analysis. Therefore, marginally higher daily pharmacy costs with insulin aspart should not be a barrier to reimbursement and widespread uptake amongst type 2 diabetes patients requiring insulin in the Japanese setting.
Transparency
Declaration of funding
This analysis was supported by an unrestricted grant from Novo Nordisk A/S, Copenhagen, Denmark.
Declaration of financial/other relationships
R.P. and W.V. are currently employed by Ossian Health Economics and Communications GmbH, Basel, Switzerland, which has received consulting fees from Novo Nordisk A/S. T.P. is currently employed by Novo Nordisk A/S. H.N. is currently employed by Osaka Saiseikai Nakatsu Hospital, Osaka, Japan.
Acknowledgements
The authors would like to acknowledge and thank Yuki Narita for her assistance in the cost data collection for the analysis.
This study was supported by an unrestricted grant from Novo Nordisk.
Previous presentations: European Association for the Study of Diabetes 45th Annual Meeting, Vienna, Austria, 2009. (abstract and poster 891); International Diabetes Federation 20th World Diabetes Congress, Montreal, Canada, 2009. (abstract and poster MT-1608); International Society for Pharmacoeconomics and Outcomes Research 15th Annual International Meeting, Atlanta, USA, 2010. (abstract and poster PDB31)
References
- Adler AI, Boyko EJ, Ahroni JH, et al. Risk factors for diabetic peripheral sensory neuropathy. Results of the Seattle Prospective Diabetic Foot Study. Diabetes Care 1997;20:1162-1167
- Klein R. Hyperglycemia and microvascular and macrovascular disease in diabetes. Diabetes Care 1995;18:258-68
- Lehto S, Rönnemaa T, Pyörälä K, et al. Predictors of stroke in middle-aged patients with non-insulin-dependent diabetes. Stroke 1996;27:63-68
- Turner RC, Millns H, Neil HA, et al. Risk factors for coronary artery disease in non-insulin dependent diabetes mellitus: United Kingdom Prospective Diabetes Study (UKPDS: 23). BMJ 1998;316:8233-8238
- Standl E, Balletshofer B, Dahl B, et al. Predictors of 10-year macrovascular and overall mortality in patients with NIDDM: the Munich General Practitioner Project. Diabetologia 1996;39:1540-1545
- Groeneveld Y, Petri H, Hermans J, et al. Relationship between blood glucose level and mortality in type 2 diabetes mellitus: a systematic review. Diabet Med 1999;16:2-13
- Wei M, Gaskill SP, Haffner SM, et al. Effects of diabetes and level of glycemia on all-cause and cardiovascular mortality. The San Antonio Heart Study. Diabetes Care 1998;21:1167-1172
- Knuiman MW, Welborn TA, Whittall DE. An analysis of excess mortality rates for persons with non-insulin-dependent diabetes mellitus in Western Australia using the Cox proportional hazards regression model. Am J Epidemiol 1992;135:638-648
- Hanefeld M, Fischer S, Julius U, et al. Risk factors for myocardial infarction and death in newly detected NIDDM: the Diabetes Intervention Study, 11-year follow-up. Diabetologia 1996;39:1577-1583
- Stratton IM, Adler AI, Neil HA, et al. Association of glycaemia with macrovascular and microvascular complications of type 2 diabetes (UKPDS 35): prospective observational study. BMJ 2000;321:405-412
- International Diabetes Federation. Diabetes Atlas, 3rd edn. Brussels: International Diabetes Federation, 2006
- Bando Y, Kanehara H, Aoki K, et al. Characteristics of undiagnosed diabetes mellitus in a population undergoing health screening in Japan: target populations for efficient screening. Diabetes Res Clin Pract 2009;83:341-346
- Neville SE, Boye KS, Montgomery WS, et al. Diabetes in Japan: a review of disease burden and approaches to treatment. Diabetes Metab Res Rev 2009;25:705-716
- World Health Organization Western Pacific Region. Plan of action for the Western Pacific Declaration on Diabetes 2000-2005. Manila: International Diabetes Foundation – Western Pacific Regional Office, 2001
- Kamae I, Kasuga M. [Medical economics of diabetes—consideration of its background and significance.] Medical ASAHI 2003; December: 68-72
- Takeda A. [The policy for diabetes of local government]. Nippon Rinsho 2002;60(Suppl 10):608-612
- Zhang P, Zhang X, Brown J, et al. Global healthcare expenditure on diabetes for 2010 and 2030. Diabetes Res Clin Pract 2010;87:293-301
- JDFI: Current status, Future Directions. Report of the Juvenile Diabetes Foundation International World Conference on Diabetes Research 1985; Monaco, 1985
- Setter SM, Corbett CF, Campbell RK, et al. Insulin aspart: a new rapid-acting insulin analog. Ann Pharmacother 2000;34:1423-1431
- Howey DC, Bowsher RR, Brunelle RL, et al. [Lys(B28), Pro(B29)]-human insulin. A rapidly absorbed analogue of human insulin. Diabetes 1994;43:396-402
- Torlone E, Fanelli C, Rambotti AM, et al. Pharmacokinetics, pharmacodynamics and glucose counter-regulation following subcutaneous injection of the monomeric insulin analogue [Lys(B28), Pro(B29)] in IDDM. Diabetologia 1994;37:713-720
- Siebenhofer A, Plank J, Berghold A, et al. Short acting insulin analogues versus regular human insulin in patients with diabetes mellitus. Cochrane Database of Systematic Reviews 2006, Issue 2. Art. No.: CD003287
- Nishimura H, Shintani M, Maeda K, et al. Does multiple injection therapy (MIT) with an ultra-rapid-acting insulin analogue prevent cardiovascular disease in type 2 diabetes? Poster presentation at the 44th Annual Meeting of the European Association for the Study of Diabetes, 2008, Rome, Italy
- Stevens RJ, Kothari V, Adler AI, et al.; United Kingdom Prospective Diabetes Study (UKPDS) Group. The UKPDS risk engine: a model for the risk of coronary heart disease in type II diabetes (UKPDS 56). Clin Sci (Lond) 2001;101:671-679
- Appel L, Llinas R. Hypertension and Stroke. Johns Hopkins White Papers, 2007. ISBN 193308748X
- Clarke PM, Gray AM, Briggs A, et al.; UK Prospective Diabetes Study (UKDPS) Group. A model to estimate the lifetime health outcomes of patients with type 2 diabetes: the United Kingdom Prospective Diabetes Study (UKPDS) Outcomes Model (UKPDS no. 68). Diabetologia 2004;47:1747-1759
- World Health Organization. Japanese life tables. Available at http://www.who.int/whosis/database/life_tables/life_tables.cfm [last accessed 8/7/2009]
- Inomata T, Izumi T, Kobayashi M. Cost-effectiveness analysis of carvedilol for the treatment of chronic heart failure in Japan. Circ J 2004;68:35-40
- Saito I, Kobayashi M, Matsushita Y, et al. Cost-utility analysis of antihypertensive combination therapy in Japan by a Monte Carlo simulation model. Hypertens Res 2008;31:1373-1383
- Miyagawa T, Arakawa I, Shiragami M, et al. Cost-effectiveness of including salmeterol in asthma therapy in a primary care setting in Japan. Yakugaku Zasshi 2006;126:51-59
- Tsutani K, Igarashi A, Fujikawa K, et al. A health economic evaluation of aspirin in the primary prevention of cardiovascular disease in Japan. Intern Med 2007;46:157-162
- Babazono A, Miyazaki M, Imatoh T, et al. Effects of the increase in co-payments from 20 to 30 percent on the compliance rate of patients with hypertension or diabetes mellitus in the Employed Health Insurance System. Int J Technol Assess Health Care 2005;21:228-233
- Reviriego J, Gomis R, Marañés JP, et al. Cost of severe hypoglycaemia in patients with type 1 diabetes in Spain and the cost-effectiveness of insulin lispro compared with regular human insulin in preventing severe hypoglycaemia. Int J Clin Pract 2008;62:1026-1032
- Citibank N.A. via Google Finance. EUR to JPY 2008 mid-year exchange rate. http://www.google.com/finance?chdet=1215126000000&chddm=27620&q=CURRENCY:EURJPY&ntsp=0. Last accessed October 30, 2010
- Clarke P, Gray A, Holman R. Estimating utility values for health states of type 2 diabetic patients using the EQ-5D (UKPDS 62). Med Decis Making 2002;22:340-349
- Seto TB, Taira DA, Berezin R, et al. Percutaneous coronary revascularization in elderly patients: Impact on functional status and quality of life. Ann Intern Med 2000;132:955-958
- Rumsfeld JS, Magid DJ, Plomondon ME, et al. Department of Veterans Affairs Angina With Extremely Serious Operative Mortality (AWESOME) Investigators. Health-related quality of life after percutaneous coronary intervention versus coronary bypass surgery in high-risk patients with medically refractory ischemia. J Am Coll Cardiol 2003;41:1732-1738
- Loponen P, Luther M, Korpilahti K, et al. HRQoL after coronary artery bypass grafting and percutaneous coronary intervention for stable angina. Scand Cardiovasc J 2009;43:94-99
- Davis RE, Wittrup-Jensen KU, Peters JR, et al. The impact on health-related quality of life (EQ-5D index) in people with type 1 diabetes who experience severe hypoglycemia. Diabetologia 2005;48 Suppl: A3. (EASD abstract and poster)
- Shiroiwa T, Sung YK, Fukuda T, et al. International survey on willingness-to-pay (WTP) for one additional QALY gained: what is the threshold of cost effectiveness? Health Econ 2010;19:422-437
- Gallagher A, Home PD. The effect of improved post-prandial blood glucose control on post-prandial metabolism and markers of vascular risk in people with type 2 diabetes. Diabetes Res Clin Pract 2005;67:196-203
- Sekikawa A, Kuller LH, Ueshima H, et al. Coronary heart disease mortality trends in men in the post World War II birth cohorts aged 35-44 in Japan, South Korea and Taiwan compared with the United States. Int J Epidemiol 1999;28:1044-1049
- Iwamoto Y, Akanuma Y, Niimi H, et al. Comparison between insulin aspart and soluble human insulin in type 1 diabetes (IDDM) patients treated with basal-bolus insulin therapy -- Phase III clinical trial in Japan. J Japan Diabet Soc 2001;44:799-811
- Haffner SM. The importance of hyperglycemia in the nonfasting state to the development of cardiovascular disease. Endocr Rev 1998;19:583-592
- Bonora E. Postprandial peaks as a risk factor for cardiovascular disease: epidemiological perspectives. Int J Clin Pract Suppl 2002;129:5-11
- Temelkova-Kurktschiev TS, Koehler C, Henkel E, et al. Postchallenge plasma glucose and glycemic spikes are more strongly associated with atherosclerosis than fasting glucose or HbA1c level. Diabetes Care 2000;23:1830-1834
- DECODE Study Group, European Diabetes Epidemiology Group. Is the current definition for diabetes relevant to mortality risk from all causes and cardiovascular and noncardiovascular diseases? Diabetes Care 2003;26:688-696
- Stentz FB, Umpierrez GE, Cuervo R, et al. Proinflammatory cytokines, markers of cardiovascular risks, oxidative stress, and lipid peroxidation in patients with hyperglycemic crises. Diabetes 2004;53:2079-2086
- Willan AR, O'Brien BJ. Sample size and power issues in estimating incremental cost-effectiveness ratios from clinical trials data. Health Econ 1999;8:203-211