
Abstract
Objective:
This study was conducted to assess the cost effectiveness of zoledronic acid 5 mg as a first-line treatment for the secondary prevention of fragility fractures in women with postmenopausal osteoporosis in Finland, Norway and the Netherlands.
Methods:
A discrete-event, individual-patient computer-simulation model was used to compare the cost effectiveness of zoledronic acid with that of basic treatment (calcium and vitamin D) and commonly prescribed bisphosphonates in postmenopausal women aged 50–80 years who have experienced one previous fracture and have a bone mineral density T-score of −2.5.
Results:
The cost per quality-adjusted life-year (QALY) gained with zoledronic acid compared with basic treatment ranged from being cost saving in all age groups in Norway, to costing approximately €19,000 in Finland and €22,300 in the Netherlands. Compared with the other branded bisphosphonates, zoledronic acid was cost saving in many scenarios, including all age groups in Finland. In Norway, zoledronic acid dominated branded risedronate and ibandronate in all age groups and dominated or had incremental cost-effectiveness ratios (ICERs) of up to NOK83,954 per QALY gained compared with branded alendronate. In the Netherlands, zoledronic acid dominated branded intravenous ibandronate in all age groups; compared with branded risedronate and oral ibandronate, zoledronic acid dominated or had ICERs of up to €4832 per QALY gained; compared with branded alendronate, it had ICERs of up to €48,383 per QALY gained. In all three countries, zoledronic acid may be cost effective compared with generic alendronate when patient compliance with drug therapy is taken into account. Sensitivity analyses showed that the model was robust to changes in key values. The main model limitations were the lack of real-life compliance and persistence data, and lack of country-specific data for some parameters.
Conclusions:
Using local or commonly used thresholds, this analysis suggests that zoledronic acid would be a cost-effective first-line option compared with other branded bisphosphonates and, in some scenarios, compared with generic alendronate, for the secondary prevention of fractures in women with postmenopausal osteoporosis in Finland, Norway and the Netherlands.
Introduction
Postmenopausal osteoporosis is a major public health concern, incurring substantial healthcare costs. Osteoporosis is associated with significant morbidity and all-cause mortality following fragility fractures, particularly in the spine and hip. Such fractures lead to considerable disability, pain, hospitalisation, long-term care requirement, diminished quality of life, and an increase in all-cause mortality (particularly associated with hip fractures)Citation1–3. Patients who have experienced a fragility fracture are at increased risk for subsequent fracturesCitation4,Citation5 and require effective, well-tolerated treatment. In Europe it has been estimated that 2.7 million osteoporotic fractures occurred in women aged ≥50 years in 2000; of these, over 711,000 were hip fracturesCitation6. Within Europe, Norway has one of the highest risks of hip fracture, while the Netherlands and Finland are described as ‘high-risk’ countries for osteoporotic fracturesCitation7. The direct costs incurred by osteoporotic fractures in Europe were estimated to be €27.5 billion in 2000Citation6. The risk of osteoporotic fractures increases with ageCitation8 and the humanistic and economic burden will continue to escalate as the mean age of the population increases. Costs associated with osteoporotic fractures in European countries are estimated to rise to €36 billion by 2020 and to €54 billion by 2050Citation6.
While currently available oral bisphosphonates and other antiresorptive agents are effective in treating osteoporosis, their effectiveness is compromised by poor compliance and persistence; for example, about 50% of patients fail to adhere to osteoporosis treatments by the end of the first yearCitation9. This has far-reaching consequences for patients’ health and healthcare resource use. Several studies have demonstrated an association between poor compliance or persistence and an increased probability of fractureCitation10,Citation11, with one study demonstrating that 50% compliance with oral bisphosphonate therapy gives only negligible fracture protectionCitation11. Compliance and persistence with osteoporosis therapy thus also influence the costs associated with osteoporosis; poor compliance can result in wasted expense on drugs and increased costs due to fractures that could have been avoidedCitation10,Citation12,Citation13.
Zoledronic acid 5 mg is highly effective in preventing fractures in women with postmenopausal osteoporosisCitation14. Zoledronic acid 5 mg is unique among currently available osteoporosis treatments because it is administered as a once-yearly 15-minute intravenous infusion. This offers guaranteed 1-year treatment compliance and could potentially improve convenience to the patient through avoidance of the administration hurdles associated with oral bisphosphonate treatment, such as remaining in an upright position and food and drink restrictions. In addition, because administration of zoledronic acid 5 mg circumvents the gastrointestinal tract, it avoids the upper gastrointestinal side-effects that are typical of oral bisphosphonates and which can lead to decreased treatment adherenceCitation15. Long-term patient persistence with zoledronic acid 5 mg treatment is therefore likely to be improved compared with the oral bisphosphonates.
The current study aimed to compare the cost effectiveness of once-yearly zoledronic acid 5 mg for first-line use in the secondary prevention of fragility fractures in women with postmenopausal osteoporosis against that of the most widely used osteoporosis drugs approved for this indication in Finland, Norway and the Netherlands at the time when zoledronic acid was introduced and/or reimbursement sought in these countries. Cost effectiveness was assessed to assist decision-makers in reimbursement and pricing decisions relative to other available treatments. The cost-effectiveness model used in the present study is based on the health technology assessments performed for the UK’s National Institute for Health and Clinical Excellence (NICE) regarding the prevention and treatment of postmenopausal osteoporosis in the UK and published by Stevenson and colleaguesCitation8,Citation16. The model has been locally adapted for each country included in this analysis.
Methods
Study type
This cost-effectiveness analysis was conducted from the healthcare perspective of the countries studied, where healthcare comprises both community and institutionalised care. As in the approach taken by NICE and local guidelines, the analysis included those costs directly attributable to postmenopausal osteoporosis, but not indirect or intangible costs. Benefits were measured as quality-adjusted life-years (QALYs).
The cost-effectiveness model
Model structure
The analysis required the development of a discrete-event individual-patient computer simulation based on the model inputs used in the health technology assessments performed for NICE in the UKCitation8,Citation16. However, while the time horizon of the model used for those assessments was limited to 10 years, the present model can accommodate the lifetime of each patient by using the SIMUL8® interface (SIMUL8® version 13.0; SIMUL8® Corporation, Boston, MA, USA). Each patient’s path was tracked through the various transition states of the model, recording associated costs, all-cause mortality rates and health state utility values incurred as a result of fracture events (). Each run of the model comprised 100,000–250,000 patients, depending on the age group. A mean estimate was taken for the costs and QALYs of each modelled cohort.
Figure 1. Structural diagram of the cost-effectiveness model.
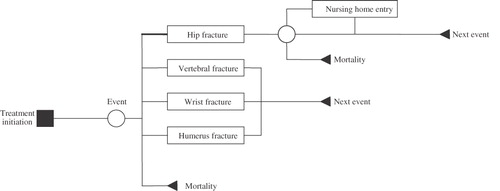
As in the NICE model and other previous cost-effectiveness analyses of bisphosphonate therapyCitation8,Citation17,Citation18, it was assumed that patients were treated for 5 years, that the effect of treatment was instantaneous, and that the relative risk of fracture returned to 1 in a linear manner over a 5-year period following cessation of treatment. Thus, the treatment effect for each intervention was modelled for a total of 10 years. The model ran for the lifetime of each patient to fully capture the costs and consequences of fractures experienced during the treatment period.
Seven different events could occur in the model: hip, vertebral, humerus or wrist fractures, nursing home placement due to hip fracture, death due to hip fracture and death from any cause. On entry into the model, the patient’s time of death was sampled from survival curves. With the exception of hip fracture, it was assumed that osteoporotic fractures do not affect all-cause mortality and so time of death was not re-sampled after a fracture event. The time to occurrence of the patient’s first fracture event was sampled next. If the sampled fracture event occurred before the time of death, costs incurred and QALYs gained in the period up to the event and the cost and utility losses caused by the event were calculated. If the patient was still alive after the event, then the time to his or her next event was sampled, with the risk of the event modified by factors from the previous event, where appropriate. The process was continued until all patients in the model had their treatment history generated until their death.
The probability of incurring a fracture is dependent on the patient’s absolute risk of a fracture given their age and their bone mineral density (BMD) T-score, their experience of previous fractures, and the effect of intervention. The time to fracture for each site was sampled by calculating the annual probability of fracture. The annual risk of a fracture was calculated for each site as a hazard where:
The probability of fracture was then calculated as 1 − exp(– fracture hazard)
The efficacy outcome measure used was QALYs. The effect of baseline comorbidities was not included in the model. It was assumed that when a patient experienced a fracture at the same site for a second or subsequent time, only the initial year’s reduction in quality of life would be taken into consideration; any long-term effects from previous fractures would be superseded.
Patient demographics
The analyses were run for a secondary prevention cohort, i.e. patients entering the model were assumed to have had one previous fracture. Patients were also assumed to have a BMD T-score of −2.5 and to be naïve to active osteoporosis treatment. Using sufficiently large numbers of patients to ensure stable results, the analyses were conducted for cohorts of postmenopausal women aged 50, 60, 70 and 80 years at the start of treatment.
Base-case analyses
The base-case scenario was run for branded zoledronic acid 5 mg once-yearly infusion [Aclasta®] and each comparator treatment (branded alendronate 70 mg oral once weekly [Fosamax®]; generic alendronate 70 mg oral once weekly; branded risedronate 35 mg oral once weekly [Actonel®/Optinate®]; branded ibandronate 150 mg oral once monthly and 3 mg injection once quarterly [Bonviva®]) against ‘basic’ treatment (placebo, calcium plus vitamin D). The base-case scenario was also applied for zoledronic acid 5 mg against each comparator treatment. For all analyses, costs incurred and the QALYs gained for each treatment were used to calculate the incremental costs per QALY gained. The incremental cost-effectiveness ratio (ICER) was defined as:
where C1 and C2 are the costs incurred when patients are treated with the specified bisphosphonate and basic treatment, respectively, and Q1 and Q2 are the QALYs gained through these treatments, respectively; or where C1 and C2 are the costs incurred when patients are treated with zoledronic acid 5 mg and one of the other specified bisphosphonates, respectively, and Q1 and Q2 are the QALYs gained through these treatments, respectively.
Sensitivity analyses
Sensitivity analyses were performed comparing zoledronic acid against branded alendronate. These included varying the drug costs; reducing the period during which nursing home costs are assumed to relate to the fracture causing nursing home entry; assessing patients with a lower T-score; and applying a 50% reduction in the cost of alendronate. A probabilistic sensitivity analysis was carried out using the Monte Carlo method to perform 1,000 runs of the model sampling from the distributions for all variables around which there was uncertainty. Sensitivity analyses were presented for the cohort of patients aged 70 years. A scenario analysis was performed to assess the impact on cost effectiveness of different levels of compliance with generic alendronate (the key comparator across all three countries), based on real-life data. Reduced compliance was applied in the model as diminished treatment effectiveness, which was extrapolated from the relationship described by Siris and colleagues for bisphosphonate efficacy in preventing fragility fracturesCitation11. Hence 90% compliance resulted in an estimated 70% efficacy and 80% compliance resulted in an estimated 50% efficacy.
Parameter estimates and sources
Baseline risk of fracture
The current model incorporated estimates of patients’ absolute risk of fracture, based on their age and T-score, and estimates of the distribution of previous fractures by age. For Finland and the Netherlands, epidemiological data on hip, wrist and proximal humerus fractures in women were derived from a large-scale Scottish studyCitation19 and data on vertebral fracture were taken from a study in SwedenCitation20, as used by Stevenson and colleaguesCitation8. For Norway, local data were obtained for hip and wrist fracturesCitation21,Citation22, while data for humerus and vertebral fractures were taken from the Swedish studyCitation20. General population fracture risks were adjusted to age and T-score specific risk as described in the analysis conducted for NICECitation8.
Events
Having an initial osteoporotic fracture greatly increases the risk for any subsequent osteoporotic fracturesCitation4,Citation5 and this was taken into account in the model by applying previous-fracture multipliers to the risk values for the different fracture types. Previous-fracture multipliers obtained from Klotzbuecher and co-workersCitation5 were adjusted downwards by 10% to adjust for BMD, as previously discussedCitation4,Citation8. For individuals who had fractures at two or more different sites, only the greatest risk adjustment was applied when calculating the risk of subsequent fractures.
Estimates of the probability of nursing home entry due to hip fracture for the Norwegian population were: 6.0%, 8.5%, 25.6% and 33.1% for ages 50–69, 70–79, 80–90 and >90 years, respectivelyCitation23. For the Dutch population, the corresponding probabilities were 0%, 4%, 12% and 17%, respectivelyCitation16. A probability of 12.5% was used for all age groups in the Finnish populationCitation24.
All-cause mortality data for the different age groups were taken from local statisticsCitation25–27. Weibull curves were fitted to the all-cause mortality data, which were then used to sample patients’ time to death. As recently reviewed by Abrahamsen and colleaguesCitation3, excess all-cause mortality after hip fracture is well documented, hence after a patient experienced a hip fracture in the model they were probabilistically tested for mortality. Data for 1-year excess mortality subsequent to a hip fracture in patients in the community and in nursing homes were as used in the NICE analysisCitation8.
Effectiveness
The reductions in the risk of fracture at each fracture site achieved with once-yearly zoledronic acid 5 mg treatment versus basic treatment were obtained from the results of the Health Outcomes and Reduced Incidence with Zoledronic Acid Once Yearly Pivotal Fracture Trial (HORIZON-PFT) ()Citation14,Citation28. This 3-year double-blind, randomised study assessed the efficacy and safety of zoledronic acid 5 mg compared with that of placebo in preventing fractures in 7736 women aged 65–89 years who had osteoporosis. All women also received calcium and vitamin D and the study was stratified to allow participants to take, in addition to study treatment, certain other approved treatments for osteoporosis, managed by their own physician.
Table 1. Efficacy values for the prevention of fragility fractures in postmenopausal women.
No data were available from direct comparisons of bisphosphonates in women with postmenopausal osteoporosis. Data on the relative risk reductions (versus placebo) achieved with risedronate and alendronate () were taken from the report by Stevenson and colleaguesCitation8 and the NICE Final Appraisal Determination on the secondary prevention of postmenopausal osteoporosisCitation29. Data for ibandronate were obtained from the package insert and published data (). It was assumed that oral and intravenous ibandronate have equivalent efficacyCitation30–32. Ibandronate does not have proven antifracture efficacy at non-vertebral sites, so the relative fracture-risk reduction for these sites was 1.0.
It was assumed that the treatment effect observed in clinical trials was independent of patients’ baseline risk factors, i.e. age and T-score.
Costs
Only costs directly attributable to a fracture event and its direct treatment and follow-up were included in the analyses (), with local costs being used where available. Where local costs were not available, source costs were adjusted for inflation and exchange rates applied. Costs for BMD scans were not included in the analyses as it was assumed that scans would be performed before the point in the patients’ management at which the model starts. It was assumed that all patients received adequate calcium and vitamin D; costs for supplements were not included in the model. All costs are presented in the local currency and were annually discounted (to convert future costs to present values) at the locally acceptable rates: 5.0% for FinlandCitation44; 4.0% for Norway (Norwegian Medicines Agency, personal communication); and 4.0% for the NetherlandsCitation46.
Table 2. Annual direct costs for patients with osteoporosis.
It was assumed that patients entering a nursing home because of hip fracture would remain there for the rest of their lives. Costs comprised the initial impact cost and then an annual cost associated with the nursing home stay.
Annual costs of osteoporosis interventions included the costs of infusion for zoledronic acid 5 mg in all countries and for intravenous ibandronate in Finland and Norway (). Costs for visits were also included. It was assumed that after the treatment period, no further costs were incurred for interventions.
For the sensitivity analysis of the impact of reduced compliance on cost effectiveness, annual drug acquisition costs were decreased in proportion to the amount of drug not obtained by the patient.
Quality of life
On entering the model the patient with osteoporosis was considered to be healthy, i.e. not experiencing any adverse effects due to hip, vertebral or wrist fracture. This baseline health state was assigned an age-specific utility value based on those for the UK general population: 0.850, 0.829, 0.747 and 0.699 at ages 50, 60, 70 and 80 years, respectivelyCitation8. On experiencing a fracture, the patient was assigned a utility value for the first year of the event, as described by Stevenson and colleaguesCitation16. This was calculated by applying a fracture-specific utility multiplier, which proportionally reduces the patient’s utility for the yearCitation47,Citation48. The multipliers for hip, proximal humerus, vertebral and wrist fracture, and for hip fracture leading to nursing home entry were 0.792, 0.794, 0.626, 0.977 and 0.400, respectivelyCitation47,Citation48. It was also assumed that for some fractures the patient could not recover in subsequent years to the level of health experienced before the event. Each fracture type was thus assigned a utility ‘ceiling’ multiplier to represent the maximum level of health to which patients could recover (0.813, 0.973, 0.909, 0.999 and 0.400, respectively)Citation16,Citation47,Citation48. The multipliers were applied to the baseline utility value to give the ongoing proportional disutility caused by the fracture. QALYs were annually discounted according to local guidance at the following rates: 5.0% for FinlandCitation44*; 4.0% for Norway (Norwegian Medicines Agency, personal communication); 1.5% for the NetherlandsCitation46.
Results
The internal validity of the model was demonstrated as the number of fractures predicted by the model was consistent with that observed in the epidemiology data. The results are presented from the healthcare perspective of each of the three countries, where healthcare includes residential care following a fracture.
Base-case analyses
The results of the base-case analyses are shown in and . For all three countries, compared with basic treatment (calcium and vitamin D), the cost per QALY gained (ICER) in any age group was highest for ibandronate and lowest for generic alendronate (). In Finland, zoledronic acid 5 mg had a lower ICER than all other branded bisphosphonates, with the cost per QALY gained decreasing from approximately €19,000 for a woman aged 50 years to €8300 for a woman aged 80 years (). In Norway, zoledronic acid 5 mg, risedronate and alendronate (branded and generic) dominated over basic treatment, with the ICER dropping substantially between the ages of 70 and 80 years (). Compared with basic treatment, zoledronic acid 5 mg had lower ICERs than branded risedronate and ibandronate. In the Netherlands, compared with basic treatment, zoledronic acid 5 mg had lower ICERs than branded risedronate and ibandronate and ranged from being cost-saving in women aged 80 years to having a cost per QALY gained of €22,330 (). Generic alendronate dominated over basic treatment at all ages.
Figure 2. Cost effectiveness by age group for selected bisphosphonates compared with basic treatment in (a) Finland, (b) Norway and (c) the Netherlands. Negative values indicate dominance, i.e. better efficacy and lower cost. ICER, incremental cost-effectiveness ratio; IV, intravenous; QALY, quality-adjusted life-year.
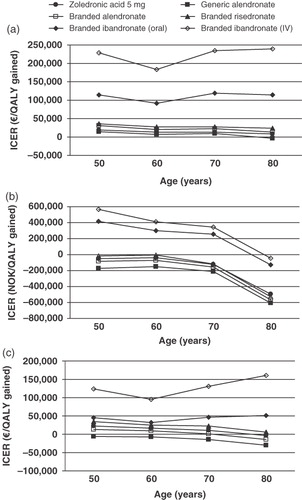
Figure 3. Cost effectiveness by age group for zoledronic acid 5 mg compared with selected bisphosphonates in (a) Finland, (b) Norway and (c) the Netherlands. Negative values indicate dominance, i.e. better efficacy and lower cost. ICER, incremental cost-effectiveness ratio; IV, intravenous; QALY, quality-adjusted life-year.
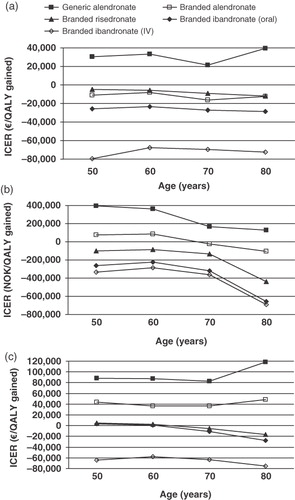
Zoledronic acid 5 mg was also a favourable option when ICERs were calculated directly in comparison with other bisphosphonates. In Finland, zoledronic acid 5 mg dominated over all the branded options for all age groups (). Compared with generic alendronate, the ICERs ranged from €21,419 to €39,614 per QALY gained (patients aged 70 and 80 years, respectively). Similarly, in Norway, zoledronic acid 5 mg dominated over branded ibandronate (oral and intravenous) and branded risedronate (). Zoledronic acid 5 mg dominated branded alendronate in patients aged 70 and 80 years; in patients aged 50 and 60 years, the ICER for zoledronic acid 5 mg compared with branded alendronate was NOK76,188 and NOK83,954 per QALY gained, respectively. Compared with generic alendronate, the ICERs for zoledronic acid 5 mg ranged from NOK130,794 to NOK396,574 per QALY gained (patients aged 80 and 50 years, respectively). In the Netherlands, zoledronic acid 5 mg dominated branded intravenous ibandronate at all ages and dominated branded oral ibandronate and risedronate in patients aged 70 and 80 years (). In patients aged 50 and 60 years, the ICERs for zoledronic acid 5 mg compared with branded oral ibandronate were €3124 and €923 per QALY gained, respectively; compared with branded risedronate the ICERs were €4832 and €2394, respectively. Compared with branded alendronate, the ICERs for zoledronic acid 5 mg ranged from €36,927 per QALY gained in patients aged 60 years to €48,383 per QALY gained in those aged 80 years. The ICER profiles were notably different between the countries, with ICERs remaining fairly similar across the age groups for Finland and the Netherlands, but decreasing after age 60 years and again after age 70 years in Norway.
Sensitivity analyses
Results of sensitivity analyses show that the model was robust to changes in key values and assumptions (). Application of lower values for compliance with generic alendronate – and hence decreased drug effectiveness – caused a substantial lowering in the ICERs for zoledronic acid 5 mg versus generic alendronate across all age groups in all countries ().
Table 3. Sensitivity analyses: Incremental cost-effectiveness ratios for zoledronic acid 5 mg versus branded alendronate.
Table 4. Sensitivity analyses: Incremental cost-effectiveness ratios for zoledronic acid 5 mg versus generic alendronate at different compliance rates for generic alendronate.
Discussion
The present study assessed the cost effectiveness of zoledronic acid 5 mg and key comparator drugs as first-line therapy for secondary prevention of fractures in postmenopausal women with one previous fracture and a T-score of –2.5 in Finland, Norway and the Netherlands at the time when zoledronic acid was introduced and/or reimbursement sought in these countries. A particular strength of this study was the model used; the discrete-event individual-patient model using SIMUL8® software has a distinct advantage over the cohort models used in some previous analyses in that it avoids the need for a large number of health states in order to correctly apply combinations of factors such as prior fractures and residential status. Such factors are more accurately employed in the individual-patient model where a full patient history is created. In addition, the current model has advantages over the model used in the assessments conducted for NICECitation8,Citation16. Although the NICE model also considered individual patient data, it was not based on discrete-event simulation; furthermore it was developed using Microsoft Excel software, which has restrictive processing and therefore required a Gaussian approximation to improve processing speed. It was thus limited in its time horizon and adaptability, compromising the accuracy of the results and the ability to vary assumptions. In contrast, by employing SIMUL8®, the model used in the present study allows simulation of events throughout the individual patient’s lifetime.
The comparator drugs chosen for analysis are those most commonly prescribed for osteoporosis in the countries studied. Generic alendronate has generally become the most frequently prescribed bisphosphonate. The analyses were conducted from what is termed a ‘healthcare perspective’, however, the authors recognise that in reality the cost of care for institutionalised patients might be funded from a different source to the other costs.
At present, no formally recognised thresholds for cost effectiveness (cost per QALY gained) are available in the countries studied. For the Netherlands, an often quoted willingness-to-pay threshold stems from the guideline on cholesterol-lowering drugs issued in 1998, which mentions a value of €18,000 per QALY gainedCitation49. However, in 2006, the Dutch Council for Public Health and Health Care stated that it might be acceptable to pay €80,000 per QALY gained for indications with a very high disease burden and unmet needCitation50. For Finland and Norway, it was assumed that the threshold applied by NICE in the UK would be applicable for the purposes of the current study, i.e. approximately £20,000–£30,000 per QALY gained. Using these thresholds (€80,000 for the Netherlands, €30,000 for Finland and Norway), zoledronic acid 5 mg was either dominant or cost effective compared with basic treatment in women with postmenopausal osteoporosis (T-score −2.5, one previous fracture) aged 50–80 years in all three countries. Zoledronic acid 5 mg was also dominant or cost effective compared with the other branded bisphosphonates most commonly prescribed for postmenopausal osteoporosis in the three countries examined, at all ages tested. Compared with generic alendronate, at the lower levels of compliance assessed, zoledronic acid 5 mg would probably be cost effective or even dominant in all age groups tested for all three countries. Even assuming full patient compliance with the oral bisphosphonate, zoledronic acid 5 mg was a cost-effective alternative for patients aged 70 years in Finland and for patients aged 70–80 years in Norway.
The differences in results observed between the countries included in the analysis are primarily driven by the differences in baseline risk of fracture and its incidence, annual cost of treating fractures and drug acquisition costs. In particular there is a much higher risk of hip fracture in the Norwegian epidemiology data compared with Finland and the Netherlands; due to the high cost of treatment, this is a key driver of the cost effectiveness. Other country-specific variations in the modelled data are likely to have contributed to these differences; for example, in the Finnish analysis, increased costs were applied to patients aged >80 years in association with some types of fractures. It is also noticeable that the ICERs change more dramatically with age in some scenarios than in others. For example, in Norway the ICERs for all bisphosphonates versus basic treatment decrease substantially at age 80 years compared with other age groups, and in Finland the ICERs for zoledronic acid 5 mg versus generic alendronate are much lower in patients aged 70 years than for other age groups. In addition to differences in local costs, such changes may in part be due to an increased proportion of fractures in these age groups being hip fractures – the most costly type of fragility fracture to manage. For example, in Norway the risk of hip fracture and the probability of subsequent nursing-home entry was higher in older age groups (>75 years) compared with the other countries.
The costs included in the study are those applicable in 2008 when zoledronic acid 5 mg entered the market. Since these analyses were conducted, drug prices have changed and a greater number of generic alendronate formulations as well as generic risedronates have become available in some countries. In the specified scenarios – and when compliance is taken into account – the principal outcomes of the present analyses are likely to prevail: that zoledronic acid 5 mg is likely to be a cost-effective option compared with other branded bisphosphonates and may be cost effective compared with generic formulations. However, given the recent rapid changes in drug costs and availability in this therapeutic area, any future assessments of the relative cost effectiveness of these drugs should incorporate current local costs and formularies.
The model was used as originally populated for reimbursement applications. The data incorporated in the model were obtained from local sources and from data previously used in the analyses conducted for NICE in the UKCitation8. For Finland and the Netherlands some of the epidemiological data (hip, wrist and proximal humerus fracture rates) were taken from a Scottish study used in the NICE analysis, rather than from local sources. Fracture incidence in Finland and the Netherlands is very similar to that in the UKCitation51, however, the authors acknowledge that local differences in fracture incidence rates, particularly for hip fracture, may affect the cost-effectiveness outcomes. The authors are also aware that studies that could provide data have been conducted since the present model was constructedCitation52. Assumptions were also made regarding some of the efficacy data for comparator agents. To date, ibandronate has not been shown in randomised clinical trials to have antifracture efficacy at non-vertebral sitesCitation32, so for the purposes of the model, a relative risk reduction of 1.0 was assigned at these sites. Recent analyses of pooled data have suggested that higher doses of ibandronate may reduce non-vertebral fracture risk in postmenopausal womenCitation53,Citation54, but this remains to be proven in a clinical trial.
The current analysis modelled a particular set of scenarios in which a number of factors were included, however, it was not possible to encompass all possible influences on cost and efficacy. Some of the factors that may alter cost effectiveness in clinical practice are discussed below and demonstrate that the data presented – and hence the cost-effectiveness results – are likely to be conservative estimates, in particular for zoledronic acid 5 mg.
The present study considered patients with a T-score of –2.5, the minimum threshold for osteoporosis. Although a low T-score is not the only indicator of risk, and several other factors should be taken into account in clinical practice, patients with lower T-scores are at greater risk of fracture. Treatment with a bisphosphonate would thus be expected to avoid more fractures and be even more cost-effective than basic treatment in such patients compared with those at the minimum threshold of osteoporosis.
When applying fracture-associated reductions in quality of life, it was assumed that the impact of the fracture with the most severe utility detriment superseded any effect of previous or current fracture(s), thus in the model it is possible to have a fracture that has no utility impact (for example a wrist fracture following a hip fracture). Such conservative assumptions contribute to an underestimation of the cost effectiveness of treatments with better fracture prevention.
One of the most important aspects of osteoporosis treatment is adherence to therapy. As for many drugs used to treat predominantly asymptomatic conditions, compliance and persistence with osteoporosis medications are poor. Studies of real-world patient activity have revealed that up to 50% of patients have discontinued oral bisphosphonates by the end of the first year of treatmentCitation9,Citation55. Persistence and compliance diminish even further over longer periods; for example, van den Boogaard and colleagues showed that 2-year persistence with weekly bisphosphonates was as low as 26%Citation56. Several studies have demonstrated that poor compliance and/or persistence with bisphosphonates have a significant negative impact on treatment outcomesCitation10,Citation11. Meijer and colleagues have also shown that continued compliant use of bisphosphonates is required to maintain efficacy in preventing fractureCitation57. Given that a minimum of 50% compliance is required in order to attain anything above negligible clinical efficacyCitation11, it is likely that many patients prescribed oral antiresorptives are not achieving optimal fracture protection. Not surprisingly, modelled analyses of bisphosphonate treatment for postmenopausal osteopenia or osteoporosis have shown that compliance and persistence have an effect on cost effectivenessCitation58,Citation59. Although the genericisation of alendronate may reduce drug acquisition costs, recent data suggest that persistence with generic alendronate is even poorer than with branded alendronateCitation60.
The sensitivity analyses conducted in the present study investigated the potential impact on cost effectiveness of suboptimal compliance. Annual compliance rates of 90% and 80% for generic alendronate would result in zoledronic acid 5 mg being a cost effective or dominant option in many age groups. The compliance rates assumed in the sensitivity analyses are still very conservative compared with what might be expected in clinical practice, and it was also assumed that the level of compliance would be the same for each of the 5 years of treatment. In reality, compliance and persistence with the comparators included in the present study are likely to be lower than assumed in the model and hence their cost-effectiveness values are likely to be lower than calculated. Persistence and compliance with zoledronic acid 5 mg was assumed to be 100% in both the base-case and sensitivity analyses. This can be confidently assumed for the first year of treatment, as a single infusion guarantees 1 year of exposure. Surveys of patient preference in clinical trials of zoledronic acid 5 mg versus weekly alternatives (while still blinded to treatment) show that patients predominantly prefer yearly administration and thus suggest that patients will be more likely to persist with such therapyCitation61,Citation62. In the HORIZON-PFT approximately 80% of patients received all three scheduled infusions of zoledronic acid 5 mgCitation14. However, persistence levels for zoledronic acid 5 mg in clinical practice are as yet unexplored, due to a lack of real-life usage data at the time this cost-effectiveness study was conducted; thus the sensitivity analyses could not incorporate the levels of compliance and persistence that might occur in real clinical practice. Despite this, the study has demonstrated the effect of the differences in compliance that might be reasonably expected between zoledronic acid 5 mg and generic alendronate. Further real-life analyses of compliance and persistence beyond the first infusion are planned once sufficient data have been collected for zoledronic acid 5 mg in women with postmenopausal osteoporosis.
Treatment-associated adverse events were not included in the model. In clinical practice, the oral bisphosphonates are likely to be associated with upper gastrointestinal adverse events that may require additional visits to a primary care physician and additional treatment. Such events may also lead to reduced quality of life and to discontinuation. With regard to zoledronic acid 5 mg, a low number of patients may experience post-dose flu-like symptoms. Clinical trials have shown these events to be generally mild to moderate and transient, usually resolving within 3 days and diminishing with each subsequent annual infusionCitation14. The symptoms can be reduced by administering paracetamol (acetaminophen) or ibuprofen before the intravenous infusionCitation63 with a minimal impact on costs. Thus, given that the most common adverse events occurring with zoledronic acid 5 mg would have little impact on cost-effectiveness, while the costs and effects of gastrointestinal adverse events associated with oral bisphosphonates would diminish their cost effectiveness, the estimates reported in this study of zoledronic acid’s cost effectiveness relative to the oral bisphosphonates are likely to be conservative.
The model assumed that all the drugs involved would affect all-cause mortality only to the degree that they prevent hip fracture. The HORIZON-Recurrent Fracture Trial (HORIZON-RFT) demonstrated that zoledronic acid 5 mg was associated with a significant 28% reduction in the risk of all-cause mortality in patients who had experienced a hip fractureCitation64. To what extent this was due to the reduction in hip fracture in the study population is unknown, but there may be other factors involved that were not taken into account in the current model. As the HORIZON-RFT population was different to that modelled in the present study – the former comprised male and female patients, all with hip fracture and many with a T-score below –2.5 – the all-cause mortality benefit observed in this study was not applied in the model. There is also evidence that vertebral fractures are associated with an increased risk of all-cause mortalityCitation65–67, although the risk has not been well characterised. However, given that the drugs included here – in particular zoledronic acid 5 mg – are effective in preventing vertebral fracture, they are likely to be more cost effective compared with basic treatment in clinical practice than estimated by the present analysis if all-cause mortality following vertebral fracture is considered. In addition, the current model used estimates of excess mortality occurring within 12 months after a hip fractureCitation8. In reality, the impact of hip fracture on mortality is likely to be longer lasting, possibly up to several yearsCitation3. Thus, the benefit derived from prevention of hip fracture may be more extensive than considered in the model, again suggesting that the present estimates of zoledronic acid’s cost effectiveness may be conservative.
Conclusions
Zoledronic acid 5 mg represents an effective new treatment for osteoporosis in postmenopausal women. Compared with oral antiresorptive therapies, it has the potential advantage of extended effectiveness because the once-yearly infusion is sufficient to provide year-long exposure without the problems of poor compliance that are associated with oral agents.
Based on clinical trial efficacy data, the current study has shown that in postmenopausal women with osteoporosis requiring secondary prevention of fragility fractures (i.e. women with a previous fracture and a T-score of −2.5) in Finland, Norway and the Netherlands, the use of zoledronic acid 5 mg is likely to translate into a cost-effective first-line approach compared with basic treatment and with the most commonly prescribed branded bisphosphonates. In addition, in some scenarios, zoledronic acid 5 mg may be a cost-effective alternative to generic alendronate.
Transparency
Declaration of funding
This work was supported by an unrestricted educational grant from Novartis Pharmaceutical Corporation.
Declaration of financial/other relationships
R. Akehurst received payment from Novartis for the original model development to support reimbursement submissions relating to zoledronic acid but did not receive fees or funding in relation to the development of the current manuscript; he is also a paid adviser to Novartis on other products.
R. Ariely is an employee of Novartis Pharmaceuticals Corporation.
S.B. has received consultancy fees and research funding from Novartis but did not receive fees or funding in relation to the development of the current manuscript.
N.B. has received consultancy fees from Novartis but did not receive fees or funding in relation to the development of the current manuscript.
P.F. is an employee of Novartis Norge AS.
M.G. is an employee of Novartis Pharma BV.
T.L. is an employee of Novartis Finland Oy.
Acknowledgements
Editorial support was provided by J. Ponting at Anthemis Consulting Ltd, funded by Novartis Pharmaceutical Corporation.
Notes
* This was the rate applicable at the time of the analysis. The most recent guidance (2009) recommends a rate of 3.0%45.
References
- Cooper C. The crippling consequences of fractures and their impact on quality of life. Am J Med 1997;103(2 Suppl 1):12-17
- Lips P, Cooper C, Agnusdei D, et al. Quality of life in patients with vertebral fractures: validation of the Quality of Life Questionnaire of the European Foundation for Osteoporosis (QUALEFFO). Working Party for Quality of Life of the European Foundation for Osteoporosis. Osteoporos Int 1999;10:150-160
- Abrahamsen B, van Staa T, Ariely R, et al. Excess mortality following hip fracture: a systematic, epidemiological review. Osteoporos Int 2009;20:1633-1650
- Kanis JA, Johnell O, De Laet C, et al. A meta-analysis of previous fracture and subsequent fracture risk. Bone 2004;35:375-382
- Klotzbuecher CM, Ross PD, Landsman PB, et al. Patients with prior fractures have an increased risk of future fractures: a summary of the literature and statistical synthesis. J Bone Miner Res 2000;15:721-739
- Kanis JA, Johnell O. Requirements for DXA for the management of osteoporosis in Europe. Osteoporos Int 2005;16:229-238
- Kanis JA, Johnell O, De Laet C, et al. International variations in hip fracture probabilities: implications for risk assessment. J Bone Miner Res 2002;17:1237-1244
- Stevenson M, Lloyd Jones M, De Nigris E, et al. A systematic review and economic evaluation of alendronate, etidronate, risedronate, raloxifene and teriparatide for the prevention and treatment of postmenopausal osteoporosis. Health Technol Assess 2005;9:1-160
- Seeman E, Compston J, Adachi J, et al. Non-compliance: the Achilles' heel of anti-fracture efficacy. Osteoporos Int 2007;18:711-719
- Huybrechts KF, Ishak KJ, Caro JJ. Assessment of compliance with osteoporosis treatment and its consequences in a managed care population. Bone 2006;38:922-928
- Siris ES, Harris ST, Rosen CJ, et al. Adherence to bisphosphonate therapy and fracture rates in osteoporotic women: relationship to vertebral and nonvertebral fractures from 2 US claims databases. Mayo Clin Proc 2006;81:1013-1022
- Briesacher BA, Andrade SE, Yood RA, et al. Consequences of poor compliance with bisphosphonates. Bone 2007;41:882-887
- Sheehy O, Kindundu CM, Barbeau M, et al. Adherence to weekly oral bisphosphonate therapy: cost of wasted drugs and fractures. Osteoporos Int 2009;20:1583-1594
- Black DM, Delmas PD, Eastell R, et al. Once-yearly zoledronic acid for treatment of postmenopausal osteoporosis. N Engl J Med 2007;356:1809-1822
- Penning-van Beest FJA, Erkens JA, Olson M, et al. Determinants of noncompliance with bisphosphonates in women with postmenopausal osteoporosis. Curr Med Res Opin 2008;24:1337-1344
- Stevenson M, Davis S, Lloyd-Jones M, et al. The clinical effectiveness and cost-effectiveness of strontium ranelate for the prevention of osteoporotic fragility fractures in postmenopausal women. Health Technol Assess 2007;11:1-134
- Johnell O, Jönsson B, Jönsson L, et al. Cost-effectiveness of alendronate (fosamax) for the treatment of osteoporosis and the prevention of fractures. Pharmacoeconomics 2003;21:305-314
- Borgström F, Carlsson A, Sintonen H, et al. The cost-effectiveness of risedronate in the treatment of osteoporosis: an international perspective. Osteoporos Int 2006;17:996-1007
- Singer BR, McLauchlan GJ, Robinson CM, et al. Epidemiology of fractures in 15,000 adults: the influence of age and gender. J Bone Joint Surg Br 1998;80:243-248
- Kanis JA, Johnell O, Oden A, et al. Long-term risk of osteoporotic fracture in Malmö. Osteoporos Int 2000;11:669-674
- Lofthus CM, Osnes EK, Falch JA, et al. Epidemiology of hip fractures in Oslo, Norway. Bone 2001;29:413-418
- Lofthus CM, Frihagen F, Meyer HE, et al. Epidemiology of distal forearm fractures in Oslo, Norway. Osteoporos Int 2008;19:781-786
- Osnes EK, Lofthus CM, Meyer HE, et al. Consequences of hip fracture on activities of daily life and residential needs. Osteoporos Int 2004;15:567-574
- Nurmi I, Narinen A, Lüthje P, et al. Cost analysis of hip fracture treatment among the elderly for the public health services: a 1-year prospective study in 106 consecutive patients. Arch Orthop Trauma Surg 2003;123:551-554
- Statistisk sentralbyrå (Statistics Norway). 2006. Available at: www.ssb.no [Last accessed December 2007]
- Tilastokeskus (Statistics Finland). Kuolleisuus – ja eloonjäämislukuja. 2005. Available at: http://www.tilastokeskus.fi [Last accessed September 2007]
- Centraal Bureau voor de Statistiek (2006) Voorburg/Heerlen. Available at: http://www.cbs.nl [Last accessed May 2008]
- Olson M, Brereton N, Huels J, et al. Comparison of the cost-effectiveness of zoledronic acid 5 mg for the management of postmenopausal osteoporosis in the UK setting. Poster POS8 presented at the annual European congress of the International Society for Pharmacoeconomics and Outcomes Research, Dublin, Ireland, 20-23 October, 2007
- National Institute for Health and Clinical Excellence. Final Appraisal Determination: Alendronate, etidronate, risedronate, raloxifene, strontium ranelate and teriparatide for the secondary prevention of osteoporotic fragility fractures in postmenopausal women. 2007. Available at: http://guidance.nice.org.uk/page.aspx?o=437523 [Last accessed December 2009]
- Roche Products Ltd. Bonviva 3 mg/3 mL solution for injection in pre-filled syringe: Summary of product characteristics. 2006. Available at: http://emc.medicines.org.uk/emc/assets/c/html/displayDocPrinterFriendly.asp?documentid=17546 [Last accessed January 2008]
- Roche Products Ltd. Bonviva 150 mg film-coated tablets: Summary of product characteristics. 2006. Available at: http://emc.medicines.org.uk/emc/assets/c/html/displayDocPrinterFriendly.asp?documentid=16730 [Last accessed January 2008]
- Chesnut CH III, Skag A, Christiansen C. Effects of oral ibandronate administered daily or intermittently on fracture risk in postmenopausal osteoporosis. J Bone Miner Res 2004;19:1241-1249
- Hujanen T. Terveydenhuollon yksikkökustannukset Suomessa vuonna 2001, Stakes Aiheita 1/2003. Available at: http://www.stakes.fi/verkkojulkaisut/muut/Aiheita1-2003.pdf [Last accessed September 2007]
- Borgstrøm F, Zethraeus N, Johnell O, et al. Costs and quality of life associated with osteoporotic-related fractures in Sweden. Osteoporos Int 2006;17:637-650
- Meerding WJ, Mulder S, van Beeck EF. Incidence and costs of injuries in The Netherlands. Eur J Public Health 2006;16:272-278
- KOSTRA. Korrigerte brutto driftsutg., pleie i institusjon, pr. kommunal plass. 2006. Available at: http://www.ssb.no/kostra [Last accessed December 2007]
- Forbruksundersøkelsen 2003-2005. Available at: www.ssb.no/emner/05/02/fbu/tab-2006-09-11-01.html [Last accessed December 2007]
- Oostenbrink JB, Bouwmans CAM, Koopmanschap MA. Handleiding voor kostenonderzoek, methoden en standaard kostprijzen voor economische evaluaties in de gezondheidzorg. Geactualiseerde versie 2004. Diemen, The Netherlands: College voor zorgverzekeringen, 2004
- SLD price database. Helsinki, Finland: Finnish Pharmaceutical Data Ltd, 2008
- Stevenson MD, Davis SE, Kanis JA. The hospitalisation costs and out-patient costs of fragility fractures. Women's Health Med 2006;3:149-151
- Norwegian Medicines Agency Database. 2008. Available at: http://www.legemiddelverket.no/custom/Preparatsok/prepSearch____80333.aspx [Last accessed July 2008]
- Z-Index bv. Z-Index Taxe, December 2008
- Den norske legeforening. Normaltariff of privat spesialistpraksis 2007-2008. Oslo, Norway: Den norske legeforening. 2007. Available at: http://www.legeforeningen.no/assets/Normaltariffen_2007.pdf [Last accessed December 2007]
- Ministry of Social Affairs and Health. Guidelines for preparing a health economic evaluation. Annex to decree 1111/2005. Helsinki, Finland: Ministry of Social Affairs and Health, 2005
- Ministry of Social Affairs and Health. Guidelines for preparing a health economic evaluation. Annex to decree 201/2009. Helsinki, Finland: Ministry of Social Affairs and Health, 2009
- College voor zorgverzekeringen. Guidelines for pharmacoeconomic research in The Netherlands (updated version). Diemen, The Netherlands: College voor zorgverzekeringen, April 2006
- Kanis JA, Johnell O, Oden A. The risk and burden of vertebral fractures in Sweden. Osteoporos Int 2004;15:20-26
- National Osteoporosis Foundation. Osteoporosis: review of the evidence for prevention, diagnosis, and treatment and cost-effectiveness analysis. Osteoporos Int 1998;8(Suppl 4):S7-S80
- Kwaliteitsinstituut voor de Gezondheidszorg CBO. Behandeling en preventie van coronaire hartziekten door verlaging van de plasmacholesterolconcentratie. Consensus cholesterol tweede herziening. Utrecht, The Netherlands: CBO, 1998
- Council for Public Health and Health Care. Sensible and sustainable care. Zoetermeer, The Netherlands: Council for Public Health and Health Care, 2006
- FRAX® WHO Fracture risk assessment tool: Charts of the FRAX® tool. Available at: http://www.sheffield.ac.uk/FRAX/charts.jsp [Last accessed 17 September 2010]
- Kanis JA, Stevenson M, McCloskey EV. Glucocorticoid-induced osteoporosis: a systematic review and cost-utility analysis. Health Technol Assess 2007;11:1-231
- Cranney A, Wells GA, Yetisir E, et al. Ibandronate for the prevention of nonvertebral fractures: a pooled analysis of individual patient data. Osteoporos Int 2009;20:291-297
- Harris ST, Blumentals WA, Miller PD. Ibandronate and the risk of non-vertebral and clinical fractures in women with postmenopausal osteoporosis: results of a meta-analysis of phase III studies. Curr Med Res Opin 2008;24:237-245
- Lo JC, Pressman AR, Omar MA, et al. Persistence with weekly alendronate therapy among postmenopausal women. Osteoporos Int 2006;17:922-928
- van den Boogaard CH, Breekveldt-Postma NS, Borggreve SE, et al. Persistent bisphosphonate use and the risk of osteoporotic fractures in clinical practice: a database analysis study. Curr Med Res Opin 2006;22:1757-1764
- Meijer WM, Penning-van Beest FJA, Olson M, et al. Relationship between duration of compliant bisphosphonate use and the risk of osteoporotic fractures. Curr Med Res Opin 2008;24:3217-3222
- Schousboe JT, Nyman JA, Kane RL, et al. Cost-effectiveness of alendronate therapy for osteopenic postmenopausal women. Ann Intern Med 2005;142:734-741
- Goeree R, Blackhouse G, Adachi J. Cost-effectiveness of alternative treatments for women with osteoporosis in Canada. Curr Med Res Opin 2006;22:1425-1436
- Sheehy O, Kindundu CM, Barbeau M, et al. Differences in persistence among different weekly oral bisphosphonate medications. Osteoporos Int 2009;20:1369-1376
- McClung M, Recker R, Miller P, et al. Intravenous zoledronic acid 5 mg in the treatment of postmenopausal women with low bone density previously treated with alendronate. Bone 2007;41:122-128
- Saag K, Lindsay R, Kriegman A, et al. A single zoledronic acid infusion reduces bone resorption markers more rapidly than weekly oral alendronate in postmenopausal women with low bone mineral density. Bone 2007;40:1238-1243
- Novartis Europharm Ltd. Aclasta: summary of product characteristics. 2008. Available at: http://emc.medicines.org.uk/emc/assets/c/html/displaydoc.asp?documentid=18171 [Last accessed December 2008]
- Lyles KW, Colón-Emeric CS, Magaziner JS. Zoledronic acid and clinical fractures and mortality after hip fracture. N Engl J Med 2007;357:1799-1809
- Cauley JA, Thompson DE, Ensrud KC, et al. Risk of mortality following clinical fractures. Osteoporos Int 2000;11:556-561
- Kado DM, Browner WS, Palermo L, et al. for the Study of Osteoporotic Fractures Research Group. Vertebral fractures and mortality in older women: a prospective study. Arch Intern Med 1999;159:1215-1220
- Kanis JA, Oden A, Johnell O, et al. Excess mortality after hospitalisation for vertebral fracture. Osteoporos Int 2004;15:108-112