
Abstract
Objective:
To evaluate chronic obstructive pulmonary disease (COPD)-related expenditure and hospitalisation in COPD patients treated with tiotropium versus alternative long-acting bronchodilators (LABDs).
Methods:
Data were from the Thomson Reuters MarketScan Research Databases. COPD patients ≥35 years with at least one LABD claim between July 1, 2004 and June 30, 2006 were classified into five cohorts based on index LABD: monotherapy with tiotropium, salmeterol/fluticasone propionate, formoterol fumarate, or salmeterol or combination therapy. Demographic and clinical characteristics were evaluated for a 6-month pre-period and COPD-related utilisation and total costs were evaluated for a 12-month follow-up period. LABD relationship to COPD-related costs and hospitalisations were estimated by multivariate generalised linear modelling (GLM) and multivariate logistic regression, respectively.
Results:
Of 52,274 patients, 53% (n = 27,457) were male, 71% (n = 37,271) were ≥65 years, and three LABD cohorts accounted for over 90% of the sample [53% (n = 27,654) salmeterol/fluticasone propionate, 23% (n = 11,762) tiotropium, and 15% (n = 7755) combination therapy]. Patients treated with salmeterol/fluticasone propionate (p < 0.001), formoterol fumarate (p = 0.032), salmeterol (p = 0.004), or with combination therapy (p < 0.001) had higher COPD-related costs and a greater risk of inpatient admission (p < 0.01 for all) versus tiotropium.
Limitations:
These data are based on administrative claims and as such do not include clinical information or information on risk factors, like smoking status, that are relevant to this population.
Conclusions:
Patients treated with tiotropim had lower COPD-related expenditures and risk of hospitalisation than patients treated with other LABDs
Introduction
Chronic obstructive pulmonary disease (COPD) is a leading cause of morbidity and mortality in the USCitation1. In 2008, there were an estimated 12.1 million adults in the US with COPDCitation2. COPD is a costly disease with annual expenditure in the US increasing steadily. In 2004, the National Heart, Lung, and Blood Institute estimated the total cost of COPD to be $37.2 billionCitation3. Based on national surveys, the average annual per-patient healthcare expenditure for patients with COPD has been estimated to be over $4000 per patientCitation3,Citation4. A claims-based analysis of managed-care patients in Utah calculated the average annual cost of treatment per COPD patient to be $13,654Citation5.
Inpatient expenditure for COPD has been reported to comprise the greatest proportion of medical costs, often accounting for about three-quarters of COPD-related costsCitation3,Citation4,Citation6,Citation7. Hospitalisation is generally a consequence of an acute exacerbation, which increases in frequency with age and disease severity. Pharmacological management is central to controlling COPD-related symptoms and preventing acute exacerbationCitation8.
Drug therapy for COPD includes both short-acting and long-acting bronchodilators (SABDs and LABDs). The SABDs, such as albuterol and ipratropium, are recommended for treatment of mild disease and are administered as needed for symptom relief. The Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines recommends regular treatment with LABDs as the disease progresses from mild-to-moderate (stage 1 to 2)Citation8,Citation9. Three LABDs are approved for use in the US: tiotropium, formoterol, and salmeterol. Salmeterol is also available in combination with the inhaled corticosteroid fluticasone, as is the fixed-dose combination of formoterol and budesonide. Randomised, controlled trials of LABD therapies have consistently found them to improve COPD-related symptoms, reduce exacerbations, and improve quality of lifeCitation10–15.
Consistent with studies demonstrating the clinical efficacy of therapy with LABDsCitation10–15, other studies suggest that pharmacologic management with LABDs significantly reduces healthcare utilisation and costsCitation12,Citation16. For example, a study of healthcare utilisation and costs incurred during two 1-year clinical trial periods found that treatment with tiotropium, compared to usual care, defined as any medication for COPD used prior to the trial except anticholinergics and long-acting β-adrenoceptor agonists, significantly reduced hospitalisations (44% reduction) and total hospital days (50% reduction)Citation16. As a result of reduced utilisation, patients receiving tiotropium had significantly lower average per-patient costs due to hospitalisation and lower total healthcare costs relative to patients receiving usual care.
GOLD guidelines do not recommend a specific LABD as the drug of choice, citing insufficient evidence to support such a choiceCitation9. Although several existing studies have evaluated the direct medical costs of patients with COPD, there are fewer analyses comparing the real-world healthcare utilisation and costs of patients receiving different types of bronchodilators, with many of the available studies selecting patients based on both SABD and LABD useCitation3–5,Citation17,Citation18. Thus, the association between LABD treatment type and the risk of inpatient events, which account for the greatest proportion of healthcare costs among patients with COPD, remains unclear. The present study addresses these gaps in the literature by evaluating and comparing the association between different LABD treatment regimens and COPD-related healthcare expenditure and COPD-related inpatient admission among commercially-insured COPD patients receiving LABD treatment.
Methods
Data sources
Data for this retrospective database study are from the MarketScan Commercial Claims and Encounters (Commercial) and Medicare Supplemental and Coordination of Benefits (Medicare) Databases of Thomson ReutersCitation19. Together, these databases provide access to de-identified medical and prescription drug claims for over 20 million individuals annually in the US with employer-sponsored health insurance, including individuals with Medicare supplemental coverage. A total of 89% of Medicare beneficiaries have supplemental insurance; 35% have supplemental coverage through an employer-sponsored planCitation20. The databases are constructed from paid medical and prescription drug claims derived from a variety of health plans with non-capitated (e.g., fee-for-service, preferred provider organisations), fully capitated, or partially capitated payment arrangements and have been widely used for a variety of cost of illness research studiesCitation21–24. To enable analysis by setting of care, inpatient episode records are built from UB-92 claims with room and board revenue codes. UB-92 and CMS 1550 forms containing Current Procedural Terminology (CPT), Healthcare Common Procedure Coding System (HCPCS), and International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) procedure codes are used to identify outpatient claims. MarketScan data contributors provide National Drug Code (NDC) information from prescription drug claims in a National Council for Prescription Drug Programs (NCPDP)-compliant format. The present study period extended from January 1, 2004 to June 30, 2007. To accommodate a 6-month pre-period (for measurement of baseline demographic and clinical characteristics) and a 12-month post-period (for measurement of outcome measures of interest), the index date period extended from July 1, 2004 to June 30, 2006. The index date was included as the first day of the follow-up period. Because the present study did not involve the collection, use, or transmittal of individually identifiable data, institutional review board (IRB) approval was not required.
Patient selection criteria
Patients were included in the study if they met the following criteria: age 35 years and older with at least two outpatient claims or one inpatient or emergency department (ED) medical claim with a diagnosis of COPD (ICD-9-CM codes 491.x, 492.x, and 496) and at least one pharmacy claim for a LABD between July 1, 2004 and June 30, 2006 (index event) (See Appendix A for all diagnosis, procedure, and drug codes used in the study.) The index date is the first date for one of the LABDs of interest (but not necessarily the first LABD in the patient’s history). Requiring one pharmacy claim for a treatment of interest where diagnostic requirements are also implemented is a common methodological approach in retrospective data analyses and outcomes studies and has been previously used in administrative claims analyses focused on COPDCitation17,Citation18. Patients were also required to have 6 months of continuous enrolment during the period prior to the first observed LABD claim during the index period as well as 12 months following the index prescription claim. Absence of LABD use prior to the index period was not a basis for patient selection as we did not want to limit study patients to those newly treated with LABDs. Patients were excluded if they met the following criteria: presence of any medical claim with a diagnosis of asthma (ICD-9-CM diagnosis codes 493.xx), cystic fibrosis (ICD-9-CM diagnosis codes 277.0x), or tuberculosis (ICD-9-CM diagnosis codes 010.xx – 018.xx) at any time during the pre- or follow-up periods.
Patients meeting the inclusion and exclusion criteria were classified into one of five treatment cohorts based on their index LABD treatment regimen: monotherapy with (1) tiotropium, (2) salmeterol, (3) salmeterol/fluticasone propionate, (4) formoterol fumarate, or combination therapy with (5) two or more LABDs. Combination therapy was identified by a pharmacy claim for a LABD therapy other than the index medication in the 60-day period following the index date (inclusive of index) during which there was at least 1 day of overlapping days supply with the index medication.
Outcome measures
The outcome measures for this analysis were COPD-related inpatient admission and COPD-related medical expenditure in the 12-month follow-up period. COPD-related inpatient admission was identified via an inpatient medical claim with either a primary diagnosis for a respiratory condition or a secondary diagnosis for a respiratory condition where the primary diagnosis was a cardiac condition.
COPD-related medical expenditure was defined as those costs occurring on claims for services provided for the management and treatment of COPD. Specifically, COPD-related services included (a) outpatient claims with an associated primary or secondary diagnosis of COPD; (b) inpatient or ED visit claims with a primary diagnosis code for a respiratory condition; (c) inpatient and ED visit claims with a secondary diagnosis code for respiratory conditions where the primary diagnosis code on the same claim was a cardiac condition; and (d) specific medications including bronchodilators, steroids, antibiotics, oxygen, influenza/pneumonia vaccines, nebulisers, methylxanthines, mast cell stabilisers, and leukotriene modifiers.
Categories of medical services in the expenditure calculations included inpatient, ED, outpatient, and outpatient pharmacy. COPD-related expenditure for medical services paid for under fee-for-service arrangements was the allowed charges (i.e., the actual amounts paid by primary and secondary insurers plus patient cost share amounts [i.e., copayments and deductibles]). The costs of capitated medical claims were estimated using the average cost of non-capitated claims for the procedure, by geographic region and by year. Outpatient pharmaceutical costs were calculated as the sum of the insurer and patient cost shares for prescriptions. All costs were adjusted to 2006 US dollars, the most recent complete calendar year included in the study, by multiplying each year’s cost by the Medical Care Consumer Price Index (CPI)Citation25.
Covariates
Patient demographic characteristics included age at index date, patient sex, region of US residence (Northeast, North Central, South, and West), urban versus rural residence, and insurance plan type (capitated payment arrangement or not). A pre-index Charlson Comorbidity Index (CCI) score was calculated, which estimates the burden of comorbid illness from diagnoses associated with chronic diseases listed on healthcare claimsCitation26,Citation27. Higher scores of the CCI indicate a greater probability of death or major disability due to comorbid illness. Additionally, several binary indicator variables were created to denote the presence of pre-index claims with diagnoses of congestive heart failure (CHF) and pneumonia, conditions that are commonly associated with COPD and can further impact the degree of airflow limitations. Influenza and pneumonia vaccines were flagged based on the presence of HCPCS and CPT procedure codes consistent with their use, and in the case of influenza vaccines, ICD-9-CM procedure codes. Prescription claims appearing during the follow-up period with NDC codes for SABDs, systemic corticosteroids, oxygen therapy, and other respiratory medications were also flagged. Oxygen therapy was also determined on the basis of revenue, ICD-9-CM procedure, and HCPCS codes. Finally, pre-index respiratory-related inpatient and ED utilisation was summarised into a categorical variable, scored thusly: ≥2 respiratory-related events (≥2 inpatient hospitalisations or 1 inpatient hospitalisation and ≥1 ED visit or ≥2 ED visits); 1 respiratory-related event; and 0 respiratory-related events. ED visits resulting in inpatient admissions were counted towards inpatient admissions. Respiratory-related conditions were defined via: primary diagnoses associated with respiratory conditions and respiratory failure; and diagnoses associated with respiratory conditions or respiratory failure secondary to primary cardiac diagnoses.
Statistical analysis
Univariate analysis
Frequency distributions and descriptive statistics (e.g., mean and standard deviation) were used to describe the demographic and the baseline clinical characteristics of the study population. COPD-related healthcare utilisation and expenditure were summarised for the 12-month follow-up period. Differences between the treatment cohorts in the demographic and clinical characteristics were evaluated using Pearson chi-square tests for categorical variables and analysis of variance (ANOVA) for continuous variables. Values of two-sided p < 0.05 were considered statistically significant.
Multivariate analysis
Generalised linear models (GLM) were used to estimate the effects of the index LABD treatment regimen on COPD-related expenditureCitation28. Additional covariates modelled included age (in years), gender, geographic region, having had some healthcare services paid under a capitated arrangement or not, urban vs. rural residence status, overall comorbid burden (as indicated by the CCI), presence of CHF or pneumonia, status of having influenza and pneumonia vaccine, pre-period respiratory-related inpatient and ED utilisation, and total pre-period medical costs. Patients treated with tiotropium at index served as the reference group and the effects of the other four treatment regimens on COPD-related medical costs were assessed relative to treatment with tiotropium. Log link and gamma variance functions were specified in the model since the outcome of COPD-related expenditure is non-negative and skewed. Two-sided p-values for the coefficients were considered statistically significant when p < 0.05. Sensitivity analysis was conducted using either the Poisson or normal variance function.
Additionally, a multivariate logistic regression model was constructed to evaluate the impact of index LABD treatment regimen on the risk of a COPD-related inpatient admission. As with the cost model, the logistic regression model adjusted for differences between the treatment cohorts in the following demographic and pre-index clinical and utilisation characteristics: age, sex, region, health plan capitation status, urban/rural residence, CCI, comorbid CHF or pneumonia, status of having influenza and pneumonia vaccine, and pre-period respiratory-related inpatient and ED utilisation. Tiotropium monotherapy was the reference group. Odds ratios (OR) of other treatment regimens were computed as the exponential of the logistic regression coefficients. p-values for the ORs were considered statistically significant when two-sided p < 0.05.
Results
Demographic characteristics
displays the impact of each inclusion and exclusion criterion on the final sample. The demographic characteristics of the study cohort are presented in . A total of 52,274 patients were identified for analysis. Approximately 53% (n = 27,457) were male and 28.7% (n = 15,003) were aged 35–64 years. The average age [SD] of the study cohort was 71.2 years [10.6]. Nearly three-quarters (n = 38,762 or 74.2%) of the study cohort resided in the South and the North Central census regions of the US and 78.6% (n = 41,103) resided in an urban area. In all, 85% (n = 44,432) were insured by an insurance plan without capitation.
Figure 1. Schematic diagram of study cohort selection and attrition. *Data Source: MarketScan Commercial Claims and Encounters Database and MarketScan Medicare Supplemental and Coordination of Benefits Database. †ICD-9-CM diagnosis codes and NDC codes are included in the Appendix. ‡At anytime during the 6-month pre-index or 12-month post-index periods.
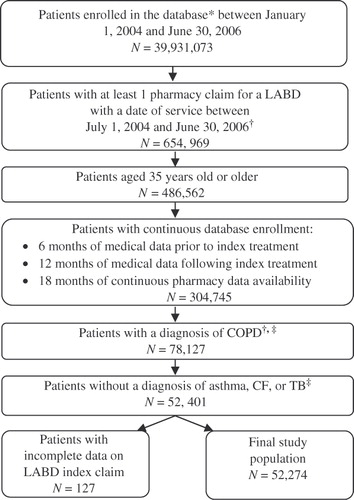
Table 1. Demographic characteristics of study cohort.
presents the demographic characteristics of the study cohort by index treatment. Significant differences in the demographic characteristics of the treatment cohorts were observed for sex, age, geographic region, urban versus rural residence, and health plan type (all p < 0.001).
Table 2. Demographic characteristics of study cohort by index treatment, evaluated at index date.
Clinical characteristics
Pre-index period clinical characteristics of the study cohort are presented in . Salmeterol/fluticasone propionate was the most commonly-used LABD medication at index among the five examined (n = 27,654 or 52.9%), followed by tiotropium (n = 11,762 or 22.5%) and combination LABD treatment (n = 7755 or 14.8%). Fewer patients were treated with salmeterol (n = 3720 or 7.1%) and formoterol fumarate (n = 1383 or 2.6%) monotherapy. A total of 81% (n = 42,422) of patients had no pre-period respiratory-related inpatient or ED utilisation event, 14.0% (n = 7300) had one such event, and 4.9% (n = 2552) had ≥2 respiratory-related events in the pre-period. Relative to the other treatment cohorts, a higher proportion of patients in the combination treatment cohort (n = 553 or 7.1%) had ≥2 respiratory-related events in the pre-period. In contrast, a lower proportion of patients receiving salmeterol at index had ≥2 respiratory-related events (n = 120 or 3.2%) as compared to the other groups. In addition to LABDs, most patients had prescription claims for other medications commonly used to manage COPD, including SABDs (70.5%), systemic corticosteroids (45.7%), oxygen therapy (30.9%), and other respiratory medications (21.3%).
Table 3. Patient Clinical Characteristics, by Index Treatment, evaluated during pre-period and follow-up period.
Multivariate results
Results of the generalised linear model estimating the association between index LABD treatment and COPD-related medical expenditure during the 12-month follow-up are presented in . The regression analysis, along with the estimated coefficients (coef), indicates that after adjusting for differences in demographic and clinical characteristics, patients treated with salmeterol/fluticasone propionate (coef = 0.145, p < 0.001), formoterol fumarate (coef = 0.215, p = 0.032), salmeterol (coef = 0.192, p = 0.004), or with combination therapy (coef = 0.350, p < 0.001) incurred significantly higher COPD-related costs over the follow-up period compared to patients treated with tiotropium monotherapy at index. Adjusting for all covariates, the expected COPD-related expenditure of patients treated with salmeterol/fluticasone propionate, formoterol fumarate, salmeterol, or combination therapy were 16–42% higher than those of patients treated with tiotropium monotherapy (16% (exp(0.145)−1) higher among patients treated with salmeterol/fluticasone propionate, 24% (exp(0.215)−1) higher among those treated with formoterol fumarate, 21% (exp(0.192)−1) higher among those treated with salmeterol, and 42% (exp(0.350)−1) higher among those treated with combination therapy). Sensitivity analysis indicated that the gamma distribution was the most appropriate variance function.
Table 4. Generalised linear model of COPD-related costs for COPD patients treated with LABDs.
Results of the logistic regression model used to estimate the risk of a COPD-related inpatient admission during follow-up are presented in . These results indicate that the risk of COPD-related inpatient admission varies significantly by treatment type. Relative to patients treated with tiotropium at index, the risk of inpatient admission was significantly higher for patients treated with each of the four alternative LABD therapies, adjusting for differences in demographic and clinical characteristics (OR = 1.162, 95% CI = 1.089–1.239 for patients treated with salmeterol/fluticasone propionate; OR = 1.178, 95% CI = 1.055–1.315 for patients treated with salmeterol; OR = 1.237, 95% CI = 1.058–1.447 for patients treated with formoterol fumarate; OR = 1.337, 95% CI = 1.233–1.45 for patients treated with combination LABD therapy; p < 0.01 for all).
Table 5. Logistic regression analysis of COPD-Related inpatient admission during a 12-month follow-up period for COPD patients treated with LABDs.
Results of the logistic regression model also indicate that older age, the presence of CHF and pneumonia in the pre-period, as well as pre-period respiratory-related inpatient and ED utilisation, and pre-period medical costs also are associated with increased risk of COPD-related inpatient admission in the follow-up period (p < 0.001).
Discussion
The GOLD guidelines recommend treatment with LABDs as first-line therapy to treat symptoms related to moderate-to-severe COPD. Several LABD treatment options are available for patients with COPD but little is known about how patient outcomes, such as healthcare utilisation and associated costs, vary by the different treatment options. This study assessed COPD-related medical expenditure and risk of inpatient admission within a cohort of commercially-insured COPD patients treated with one of five LABD regimens: monotherapy with tiotropium, salmeterol/fluticasone propionate, salmeterol, formoterol fumarate, and combination therapy with two or more LABDs.
Following adjustment for differences in patient demographic and clinical characteristics, our multivariate results indicate that COPD-related healthcare expenditure and risk of inpatient admission vary by LABD treatment type. Patients treated with salmeterol/fluticasone propionate, formoterol fumarate, salmeterol, or with combination LABD therapy incurred significantly higher COPD-related expenditure over the follow-up period compared to patients treated with tiotropium monotherapy at index. Furthermore, patients treated with salmeterol/fluticasone propionate, formoterol fumarate, salmeterol, or with combination LABD therapy at index had a significantly higher risk of COPD-related inpatient admission during the 12-month follow-up period than patients treated with tiotropium monotherapy at index.
Akazawa et al.Citation17 and Delea et al.Citation18 each conducted studies to evaluate risk of hospitalisation and ED visits and to estimate costs in COPD patients initiating treatment with various bronchodilators, using ipratropium as the comparator. While the studies found a lower risk of COPD-related hospitalisation or ED visit and lower costs in the LABD cohorts compared to ipratropium, these findings are not surprising given that regular treatment with LABDs is more effective than treatment with SABDsCitation9.
A study by Najafzadeh et al.Citation29 evaluated the cost-effectiveness of tiotropium/placebo (TP) vs. tiotropium/salmeterol (TS) and tiotropium/fluticasone/salmeterol (TFS) in 449 COPD patients with moderate-to-severe disease. Cost and outcome data were collected through a randomised, double-blind, placebo-controlled trial conducted in a patient population enrolled from 27 Canadian medical centersCitation30. In that trial, while the proportion of patients with exacerbations did not differ between the study groups, the TFS group compared to the TP group demonstrated improved lung function and disease-specific quality of life and a decreased number of COPD-related and overall hospitalisations. In the cost-effectiveness study, costs adjusted to 2006 Canadian dollars over the 52-week study period were lowest for TP (CAN$2678) vs. TS and TFS (CAN$2801 and CAN$4042, respectively). Two cost-effectiveness measures were calculated: the incremental cost per exacerbation avoided and the incremental cost per quality adjusted life-year (QALY). TS costs and exacerbation rates were higher and its effectiveness was lower vs. TP. However, the incremental cost for exacerbation avoided was CAN$6510 and the incremental cost per QALY was CAN$243,180 for TFS vs. TP. Based on these findings, the authors concluded that the combination therapy with tiotropium vs. tiotropium alone was not cost-effective. While there are obvious differences in the methodology and outcome measures in the study by Najafzadeh et al. and the current study, our study also found lower COPD-related expenditure with tiotropium monotherapy compared to other LABDs, although we also found a decreased risk of COPD-related hospitalisation. The Najafzadeh et al. study was limited to patients with moderate-to-severe COPD (FEV1/FVC ratio <0.70 and a postbronchodilator FEV1 <65% of the predicted value). It was not possible to determine disease severity from administrative claims, and although an attempt was made to adjust for differences using frequency of occurrence of respiratory-related events, to the extent that this measure was inadequate, results may be biased due to selection of patients into specific treatment groups based on COPD severity.
The findings in the Najafzadeh et al. study are particularly noteworthy given the differences in clinical outcomes of the prior randomised trial. They underscore the complex dynamic between clinical benefit and cost benefit in drug treatment of COPD and the need for additional studies in these areas. As COPD treatment regimens evolve it will be important to document both the clinical and economic benefits in relation to specific therapies. The present study assessed COPD-related medical expenditure and risk of inpatient admission within a large and diverse sample of employees with employer-sponsored health insurance. To the authors’ knowledge, the present study is the first to examine how real-world healthcare utilisation outcomes vary for COPD patients treated with different LABD therapies. Understanding the healthcare utilisation and economic outcomes incurred by patients receiving different treatment options can inform healthcare and payer decision-making and highlights the importance of effective disease management in reducing the economic burden of disease.
Limitations
This analysis has several limitations that merit discussion. First, because this study examined a cohort of patients with employer-sponsored health insurance, the results may not be generalisable to the entire US population, particularly individuals covered under state Medicaid programs. Also, while the strength of the present study was its large and diverse sample of employees, the sample was not randomly selected. It should also be noted that misclassification of condition-specific care (i.e., COPD-related care) due to inaccurate or absent diagnosis coding is possible when analyzing claims data. Additionally, like all administrative healthcare databases, the MarketScan Research Databases rely on administrative claims data for clinical detail. Potentially useful information such as race, socioeconomic status, biometric information and mortality are unavailable in medical claims. A key risk factor in COPD is smoking and data relating to smoking history and status are not available in administrative claims. Also, treatment was evaluated in this study based solely on presence of pharmacy claims for the respective drugs. Once prescribed and filled, patients may or may not take the medications as instructed. Adherence to COPD treatment regimens was not evaluated as part of this study. An additional caveat to the current study results is that the overall medical costs of patients with Medicare supplemental coverage in this study may be underestimated where Medicare paid for 100% of the healthcare service. In such instances, no commercial claim would have been generated and the cost would not have been captured in the study data. However, the data presented here accurately reflect the costs to employers and health plans for Medicare patients.
A final limitation of the present study is that the results of standard clinical measures of disease severity such as spirometry are not available in administrative claims data. In the absence of this information, an attempt was made to proxy disease severity via an utilisation-based index that evaluated respiratory-related inpatient and ED utilisation in the pre-period. Furthermore use of other respiratory medications, including SABDs, which could also be a measure of disease severity were not included in the analysis. To the extent that this index does not adequately assess disease severity, the regression results, which were adjusted for this utilisation-based measure, may be biased because of the selection of patients into specific groups based on COPD severity. Future work investigating variation in healthcare utilisation and cost outcomes by LABD treatment type among patients with COPD will benefit from the inclusion of spirometry measures.
Conclusions
It was found that COPD-related healthcare costs and the risk of COPD-related inpatient admission vary by LABD type. Specifically, patients treated with tiotropium at index incurred lower COPD-related healthcare costs than those treated with other LABDs. Additionally, it was found that COPD patients treated with tiotropium monotherapy at index had the lowest risk of COPD-related inpatient admission, a significant component of the cost of care for this condition.
Transparency
Declaration of funding
This work was supported by Boehringer-Ingelheim Pharmaceuticals, Inc (BIPI) and Pfizer Inc. All authors meet criteria for authorship as recommended by the International Committee of Medical Journal Editors (ICMJE) and were fully responsible for all content and editorial decisions, and were involved at all stages of manuscript development.
Declaration of financial/other relationships
Z.C., E.D. and N.S. were all employees at Thomson Reuters at the time of manuscript development. Thomson Reuters provides custom consulting services to all major pharmaceutical companies. K.H.Z., R.P.-R. and C.L.B. are employees of Pfizer Inc. which co-sponsored this analysis. J.S. and H.S. are employees of BIPI which sponsored this study.
Supplementary Material
Download MP3 Audio (3.6 MB)Acknowledgements
The authors wish to acknowledge the contributions of Boris Ivanov, who served as the primary SAS programmer. Liisa Palmer, PhD and Kathleen Wilson assisted with editing and formatting this manuscript.
References
- Rennard SI. COPD: overview of definitions, epidemiology and factors influencing its development. Chest 1998;113(4 Suppl): 235-241S
- American Lung Association, Trends in COPD (Chronic Bronchitis and Emphysema): Morbidity and Mortality, February 2010. Available at: http://www.lungusa.org/finding-cures/our-research/epidemiology-and-statistics-rpts.html <http://www.lungusa.org/finding-cures/our-research/epidemiology-and-statistics-rpts.html.> Accessed July 26, 2010
- Miller JD, Foster T, Boulanger L, et al. Direct cost of COPD in the U.S.: an analysis of medical expenditure panel survey (MEPS) data. COPD 2005;3:311-318
- Halpern MT, Stanford RH, Borker R. The burden of COPD in the U.S.A.: Results of the confronting COPD survey. Respir Med 2003;97(Suppl C):S81-89
- Cannon HE. Assessing the need for a clinical COPD care program in a managed care organization. J Manag Care Pharm 2004;10(4 Suppl):S17-21
- Mapel DW, Hurley JS, Frost FJ, et al. Health care utilization in chronic obstructive pulmonary disease: a case-control study in a health maintenance organization. Arch Intern Med 2000;160:2653-2658
- Hilleman DE, Dewan N, Malesker M, et al. Pharmacoeconomic evaluation of COPD. Chest 2000;118:1278-1285
- Pauwels RA, Buist AS, Calverley PM, et al. GOLD Scientific Committee. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. NHLBI/WHO global initiative for chronic obstructive lung disease (GOLD) workshop summary. Am J Respir Crit Care Med 2001;163:1256-1276
- GOLD - the Global Initiative for Chronic Obstructive Lung Disease. Available at: http://www.goldcopd.com/ <http://www.goldcopd.com/> Accessed August 2009
- Sin DD, McAlister FA, Man P, et al. Contemporary management of chronic obstructive pulmonary disease: Scientific review. JAMA 2003;290:2301-2312
- Tashkin DP, Cooper CB. The role of long-acting bronchodilators in the management of stable COPD. Chest 2004;125:249-259
- Vincken W, van Noord JA, Greefhorst AP, et al. Improved health outcomes in patients with COPD during 1 yea treatment with tiotropium. Eur Respir J 2002;19:209-216
- Mahler DA, Donohue JF, Barbee RA, et al. Efficacy of salmeterol xinafoate in the treatment of COPD. <http://www.ncbi.nlm.nih.gov/pubmed/10208192?itool=EntrezSystem2.PEntrez.Pubmed.Pubmed_ResultsPanel.Pubmed_RVDocSum&ordinalpos=43> Chest 1999;115:957-965
- Aalbers R, Ayres J, Backer V, et al. Formoterol in patients with chronic obstructive pulmonary disease: a randomized, controlled, 3-month trial. Eur Respir J 2002;19:936-943
- Calverley P, Pauwels R, Vestbo J, et al. Combined salmeterol and fluticasone in the treatment of chronic obstructive pulmonary disease: a randomised controlled trial. Lancet 2003;361:449-456
- Friedman M, Menjoge SS, Anton SF, et al. Healthcare costs with tiotropium plus usual care versus usual care alone following 1 year of treatment in patients with chronic obstructive pulmonary disorder (COPD). Pharmacoeconomics 2004;22:741-749
- Akazawa M, Hayflinger C, Stanford RH, et al. Economic assessment of initial maintenance therapy for chronic obstructive pulmonary disease. Am J Manag Care 2008;14:438-448
- Delea TE, Hagiwara M, Dalal AA, et al. Healthcare use and costs in patients with chronic bronchitis initiating maintenance therapy with fluticasone/salmeterol vs other inhaled maintenance therapies. Curr Med Res Opin 2009;25:1-13
- Chang S, Hansen LG. Health Research Data for the Real World: The MarketScan® Databases. Thomson Reuters. July 2009. Web site http://thomsonreuters.com/products_services/healthcare/healthcare_products/pharmaceuticals/epidemiolgy_res/mktscan_res_db Accessed January 16, 2010
- The Kaiser Family Foundation, Examining Sources of Coverage Among Medicare Beneficiaries: Supplemental Insurance, Medicare Advantage, and Prescription Drug Coverage Findings from the Medicare Current Beneficiary Survey, 2006. Available at: http://www.kff.org/medicare/upload/7801.pdf <http://www.kff.org/medicare/upload/7801.pdf> Accessed July 26, 2010
- Goetzel RZ, Hawkins K, Ozminkowski RJ, et al. The health and productivity cost burden of the “Top 10” physical and mental health conditions affecting six large U.S. employers in 1999. J Occup Environ Med 2003;45:5-14
- Crown WH, Finkelstein S, Berndt FR, et al. The impact of treatment-resistant depression on health care utilization and costs. J Clin Psychol 2002;63:963-971
- Durden E, Ben Joseph R, Huse D, et al. The economic costs of obesity to self-insured employers. J Occup Environ Med 2008;50:991-997
- Schulman K, Kehles J. Economic burden of metastatic bone disease in the U.S. Cancer 2007;109:2334-2342
- US Department of Labor Bureau of Labor Statistics Consumer Price Index. Available at: http://www.bls.gov/cpi/cpifact4.htm Accessed August 2009
- Charlson ME, Pompei P, Ales KL, et al. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chron Dis 1997;40:373-383
- D'Hoore W, Bouckaert A, Tilquin C. Practical considerations on the use of the Charlson Comorbidity Index with administrative data bases. J Clin Epidemiol 1996;49:1429-1433
- Nelder JA, Wedderburn R. Generalized linear models. J R Stat Soc, Ser A (General) 1972;135:370-384
- Najafzadeh M, Marra CA, Sadatsafavi M, et al. Cost effectiveness of therapy with combinations of long acting bronchodilators and inhaled steroids for treatment of COPD. Thorax 2008;63:962-967
- Aaron SD, Vandemheen KL, Fergusson D, et al. Tiotropium in combination with placebo, salmeterol, or fluticasone-salmeterol for treatment of chronic obstructive pulmonary disease: a randomized trial. Ann Intern Med 2007;146:545-555