
Abstract
Objective:
To evaluate the economic impact of intravenous iron (in the form of intravenous iron preparation of ferric carboxymaltose) in three different clinical settings of iron deficiency anemia: chemotherapy-induced anemia in breast cancer, chemotherapy-induced anemia in digestive cancer, and perioperative anemia in knee and hip surgery.
Methods:
The economic model compared the usual therapeutic strategies of anemia without intravenous iron and strategies including intravenous iron, in each of the three clinical settings selected. Costs related to anemia treatment by erythropoiesis-stimulating agents (ESA), blood transfusion, and intravenous iron were estimated and compared inside each setting. Cost savings were calculated from the French healthcare payer perspective. Data included in the economic model were obtained from scientific literature, public health agencies, and medical experts.
Results:
The most prominent annual cost savings were observed in chemotherapy-induced anemia in breast cancer (€997 and €360 per patient for metastatic and non-metastatic breast cancers, respectively; global cost saving, €33.6 million). This large impact of intravenous iron on costs was mainly explained by both a lower number of women treated and lower ESA dosing. Mean annual cost saving in digestive cancers and knee and hip surgery were estimated to €168 and €216 per patient and global cost savings of €7.5 and €12.1 million, respectively. Overall, annual cost savings in these three settings were estimated to €53 million including €39 million for ESA cost savings. Sensitivity analysis showed that strategies including intravenous iron remained cost-effective even with wide variations in the assumptions, particularly for cost savings on ESA.
Limitations:
Economic model based on literature data and expert opinions.
Conclusions:
The present economic model suggests that use of intravenous iron, according to recommendations of international guidelines, is cost saving, particularly in chemotherapy-induced anemia in breast cancers.
Introduction
Anemia occurs commonly and significantly increases healthcare costsCitation1–3. Absolute iron deficiency related to depletion of iron stores or functional iron deficiency are the main causes of anemia and can result from several causes including inadequate iron absorption, iron loss from blood loss, or iron sequestration related to chronic inflammationCitation4.
Outside the nephrology community, where erythropoiesis-stimulating agents (ESA) and intravenous iron have been standard since 1992, anemia remains under-treated in some clinical settings. Mild-to-moderate anemia (hemoglobin between 9–11 g/dL) has been reported in up to 75% of patients with cancer undergoing chemotherapy or radiotherapyCitation5,Citation6. Chemotherapy-induced anemia is a major issue causing fatigue and poorer quality-of-lifeCitation5,Citation7. Despite the high incidence of iron deficiency anemia in cancer patients, the recent AnemOnHe study performed in 2009–2010 reported that iron parameters were assessed only in one anemic patient among fiveCitation8. Anemia related to blood loss is also frequent during orthopedic surgery. After unilateral total hip replacement, from 30–70% of patients have substantial blood loss and receive allogeneic blood transfusion, and from 20–50% after unilateral total knee replacementCitation9–12.
For acute management of severe anemia, transfusion remains the standard of care. However, in mild-to-moderate anemia, several large clinical trials have demonstrated both safety and efficacy of ESA, particularly in cancer patients, resulting in fewer transfusions and improved quality-of-lifeCitation13.
Recently, the Food and Drug Administration changed the product labeling of ESA and added a black-box warning because some reports suggested that thrombotic cardiovascular events and more rapid tumor progression in some cancers could be associated with ESA treatmentCitation14. Taken together with the Market Authorization of new formulations of intravenous iron with low toxicity intravenous iron has acquired a central role in the treatment of anemia, either as a primary treatment or in combination with ESACitation15. Indeed, when iron is combined with ESA, the intravenous route is required; according to the experts of the EORTC, there is no evidence of increased response with the addition of oral iron supplementation, but there is an improved response to ESA with the addition of intravenous ironCitation16,Citation17.
Intravenous iron has been shown to optimize the response to ESA in cancer patients with chemotherapy-related anemia and to improve their quality-of-lifeCitation18. Moreover, the randomized study of Pedrazoli et al.Citation19 in solid tumor cancer patients with no absolute or functional iron deficiency showed that chemotherapy-induced anemia could nevertheless be improved with ESA combined to iron supplementation in comparison with ESA alone. Pre-operative intravenous iron alone accelerates hemoglobin level recovery and reduces transfusion requirements after surgery for hip fractureCitation20,Citation21.
In randomized trials in oncology, adverse events were not more frequent or more severe with combination of ESA and intravenous iron supplementation compared to ESA aloneCitation18,Citation19,Citation22–24. Decreasing the ESA dosing and avoiding allogeneic blood transfusion while maintaining efficacy could have potential important economic consequences. Blood transfusion is not a risk-free therapy and allogeneic blood is a scarce and expensive resource. However, the economic consequences of a more extended use of intravenous iron in anemia have not been assessed. Therefore, the aim of this study was to evaluate the economic impact of intravenous iron (in the form of intravenous iron preparation of ferric carboxymaltose; Ferinject ) in three different clinical settings: chemotherapy-induced anemia in breast cancer, chemotherapy-induced anemia in digestive cancer and perioperative anemia in knee and hip surgery.
Methods
For the comparative cost study with or without intravenous iron, clinical settings were selected according to the following criteria: (1) iron deficiency was the main cause of anemia, (2) prevalence of anemia was high (≥20%), (3) the main treatments of anemia were ESA and/or blood transfusion, (4) iron deficiency was under-treated (with intravenous iron infrequently used) and treatment with intravenous iron was justified. Three clinical settings were selected on these criteria: (1) chemotherapy-induced anemia in breast cancer; (2) chemotherapy-induced anemia in digestive cancers; and (3) perioperative anemia in knee and hip surgery.
For each of the three clinical settings, interviews of experts allowed identifying the standard therapeutic strategies for use of ESA and blood transfusion. The impact of intravenous iron on ESA and blood transfusion was assessed on the basis of clinical data from literature. Articles reporting trials that evaluated the consequences of intravenous iron supplementation on the treatment of anemia were selected. These data were approved by experts. When specific data were lacking, they were replaced by expert opinions.
Clinical and epidemiological data were obtained from medical literature (selected from Medline) and from public databases. The costs taken into account in the study were only direct costs related to anemia treatment by ESA, blood transfusion and intravenous ferric carboxymaltose. Costs presented are those that would be paid by the French national health service. Costs of treatment of anemia during hospitalization, costs of medications (for hospital pharmacy or town drugstore) and costs of nursing at home was obtained were obtained from French official healthcare databases.
For each of the three clinical settings selected, costs related to ESA consumption and/or use of blood transfusion with and without ferric carboxymaltose prescription were compared.
In order to test the robustness of the model, cost-saving sensitivity analyses were performed by varying one parameters at once (one-way sensitivity analysis). Parameters were varied to obtain cost saving equals to zero (equilibrium point). In breast cancers, the parameters tested were the decrease of blood transfusion and the ESA dosing decrease with intravenous iron (with 10% or 0% decrease of patients receiving ESA). In digestive cancers, the parameters tested were ESA dosing decrease with intravenous iron (with 10% or 0% decrease of patients receiving ESA). In knee/hip surgery, the parameter tested was the decrease of blood transfusion.
Results
Chemotherapy-induced anemia in breast cancer
Strategies of treatment in breast cancer ()
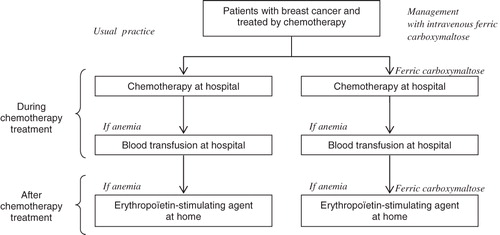
The chemotherapy-induced anemia in breast cancer is usually managed (a) by autologous blood transfusions performed at the hospital when hemoglobin level is < 8 g/dL or (b) by erythropoiesis-stimulating agent injection when hemoglobin level is in the range 8–10 g/dL; ESA injections are performed at home by a nurse after the chemotherapy cycles.
Figure 1. Comparison of treatment strategies in chemotherapy-induced anemia in breast cancer.
Hypotheses for modeling cost savings with intravenous ferric carboxymaltose in breast cancer
In 2005, 49,814 new cases of breast cancer have been diagnosed in FranceCitation25. In breast cancer, the incidence of anemia varies with the stage of the disease and particularly with the presence of metastasis. Metastatic disease is diagnosed at presentation in 5–15% of patients (estimated incidence: 4981 women); 28% of women without initial metastasis have metastases during the course of the disease (12,553 women)Citation26. Therefore, it is assumed that the prevalence of women with metastatic breast cancer is 17,535 and with non-metastatic breast cancer is 44,833.
The percentages of women receiving blood transfusion or erythropoiesis-stimulating agent have been estimated respectively to 8% and 30% (i.e., 3587 and 13,450 women) for non-metastatic breast cancer; these percentages are estimated to be 40% for transfusion and 80% for ESA among women with metastatic breast cancers (i.e., 3587 and 13,450 women) (expert opinion).
The impact of intravenous ferric carboxymaltose on the decrease of the number of blood transfusions at hospital and the decrease of ESA dosing at home was evaluated. The following parameters were applied: a decrease of 55% of the number of patients receiving blood transfusion due to persistent anemia during chemotherapyCitation22; a decrease of 10% of the number of women receiving ESA at home after the end of the chemotherapy (expert opinion)Citation24; a decrease of 25% of the ESA dosing when intravenous ferric carboxymaltose was administered together with ESA (1000 mg/2 months)Citation24.
The following standard dosing schedules were selected for ESA: 40,000 IU of epoetin beta once a week for 4 months if administered alone and 30,000 IU once a week for 4 months if administered in association with intravenous ferric carboxymaltose.
The following dosing schedules were selected for intravenous ferric carboxymaltose when administered at the hospital: one 1000 mg injection during the first and second chemotherapy cycles for patients with metastases and during the third and fourth chemotherapy cycles in patients without metastasis. There were six cycles of chemotherapy. Overall, the patients received 2000 mg of intravenous ferric carboxymaltose during chemotherapy treatment. When administered at home concomitantly with ESA, intravenous ferric carboxymaltose 1000 mg was injected once in every 2 months for 4 months.
Cost savings for chemotherapy-induced anemia in breast cancer
The medical costs related to ESA, blood transfusion, and intravenous ferric carboxymaltose are reported in . Based on the previous assumptions, the annual cost saving is estimated to be €33.6 million for ESA administration and €2.0 million for blood transfusion ().
Table 1. Summary of the different direct costs included in the economic modeling (French healthcare payer perspective).
Table 2. Estimation of annual cost savings related to intravenous ferric carboxymaltose treatment in different clinical settings (French healthcare payer perspective).
Sensitivity analysis
Taking the decrease of 55% of the number of patients receiving blood transfusion down to 37% led to a cost saving equal to 0. The sensitivity of ESA dosing decrease (25%) was assessed according to two hypotheses: 10% or 0% decrease of patients receiving ESA. Equilibrium points were achieved at −3% and 9% of ESA dosing decrease, respectively ().
Table 3. One-way cost-saving sensitivity analyses.
Chemotherapy-induced anemia in digestive cancer
Strategies of treatment in digestive cancer ()
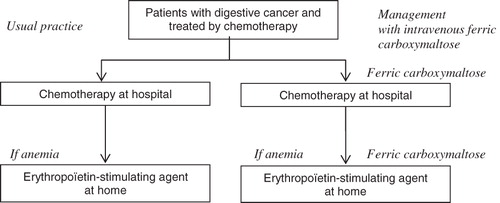
In digestive cancers, chemotherapy-induced anemia is treated mainly by ESA; blood transfusion is infrequent. ESA injections are performed at the hospital during the chemotherapy cycle and at home by a nurse.
Figure 2. Comparison of treatment strategies in chemotherapy-induced anemia in digestive cancer.
Hypotheses for modeling cost savings with intravenous ferric carboxymaltose in digestive cancer
Main digestive cancers include colorectal and stomach cancer. Their incidence is estimated at 37,413 new cases in 2005 for colorectal cancer and 7126 for stomach cancer in 20002Citation7,Citation28. Ludwig and FritzCitation6 evaluated that 62% of patients with cancer had chemotherapy-induced anemia. According to the results from the European Cancer Anemia Survey (ECAS), 23.5% of patients with cancer are treated with ESACitation29. Overall, the population of digestive cancer patients in France who received ESA was estimated to be 6489 (14.6%).
The impact of intravenous ferric carboxymaltose on the decrease of ESA dosing at home was evaluated on the same basis as for breast cancer. The following parameters were applied: a decrease of 10% of the number of patients treated by ESA at home after the end of chemotherapy (expert opinion)Citation24; a decrease of 25% of ESA dosing when intravenous ferric carboxymaltose (1000 mg/2 months) was administered together with ESACitation24.
The following standard dosing schedules were selected for ESA: 40,000 IU once a week for 4 months if administered alone and 30,000 IU once a week for 4 months if administered in association with intravenous ferric carboxymaltose. The following dosing schedules were selected for intravenous ferric carboxymaltose when administered at home: 1000 mg once in every 2 months for 4 months.
Cost savings for chemotherapy-induced anemia in digestive cancer
Based on the previous assumptions, the annual cost saving is estimated to be €7.5 million ().
Sensitivity analysis
The sensitivity of ESA dosing decrease (25%) was assessed according to two hypotheses: 10% or 0% decrease of patients receiving ESA. Equilibrium points were achieved at −3% and 9% of ESA dosing decrease, respectively ().
Perioperative anemia in knee and hip surgery
Strategies of treatment in knee and hip surgery ()
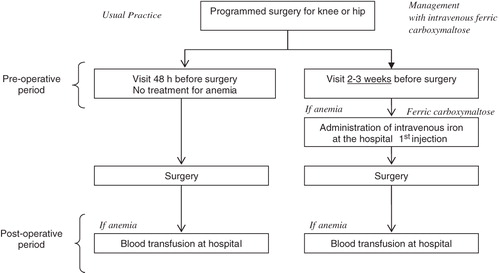
Patients with anemia before knee or hip surgery are generally not treated. If anemia is diagnosed after the operation, autologous blood transfusion is the most frequent treatment. According to experts, since knee and hip operations are programmed, treatment with intravenous iron before operation, which is supported by published data, could be appropriate in patients with iron deficiency anemia before surgeryCitation20,Citation21.
Figure 3. Comparison of treatment strategies in knee and hip surgery.
Hypotheses for modeling cost savings with intravenous ferric carboxymaltose in knee and hip surgery
The estimation of the number of knee and hip surgery operations in France was estimated to involve 187,375 patients in 2008. These operations are mainly performed in private clinics (61%).
According to the experts, anemia is present in 30% of patients after knee or hip operation; these patients, mainly elderly patients, could benefit from intravenous ferric carboxymaltose treatment (56,213 patients).
In the study of Cuenca et al.Citation20, 15% of patients who received intravenous iron before operation for hip repair received blood transfusion vs 36.8% of patients who did not receive intravenous iron (59% decrease of blood transfusions with intravenous iron).
The dosing schedule selected for intravenous ferric carboxymaltose was one intravenous injection of 500 mg 2 or 3 weeks before operation.
Cost savings for knee and hip surgery
Based on the previous assumptions, the annual cost savings related to the use of intravenous ferric carboxymaltose in the preoperative period of knee and hip surgery were estimated to be €12.1 million ().
Sensitivity analysis
By varying the decrease of 59% of the number of patients receiving blood transfusion down to 18% led to a cost saving equal to 0 ().
Discussion
The direct costs of different strategies for anemia treatment either without iron or with the new intravenous iron formulation, ferric carboxymaltose, in three clinical settings were evaluated and compared. These clinical settings have been selected because of the large number of patients untreated for anemia. The uses of ESA and blood transfusion are the followings in these clinical settings: (1) both blood transfusion and ESA in chemotherapy-induced anemia of breast cancers; (2) mainly ESA in chemotherapy-induced anemia of digestive cancers; and (3) mainly blood transfusion after knee and hip surgery. In these different clinical situations, anemia is related to absolute (depletion of iron stores) and/or functional iron deficiency (failure to release iron from stores). In contrast with oral iron, which fails in functional iron deficiency, intravenous iron is efficient both in functional and absolute deficiency by bypassing the intestinal barrier and iron sequestration in macrophages. The 2011 guidelines of the National Comprehensive Cancer Network (NCCN) recommend the use of intravenous iron in treating functional iron deficiency of cancer patientsCitation30,Citation31.
In this economic model, the most important cost savings were evidenced with chemotherapy-induced anemia in breast cancer. In this clinical setting, both blood transfusion and ESA participate in anemia treatment, but cost savings were mainly related to a decrease of ESA consumption. In chemotherapy-induced anemia for breast and digestive cancers, therapeutic schedules with intravenous iron were estimated to save each year ∼€39 million. In France, it is estimated that the global cost for ESA was €308 million in 2007Citation32; even a modest percentage of cost savings could have huge economic consequences. A recent European study showed that most cancer patients receiving ESA were treated according to guidelines except infrequent iron supplementationCitation33. In a recent observational study (AnemOnHe), only 2% of anemic patients with blood cancer and 26% of anemic patients with solid cancer received intravenous ironCitation8. These low rates of intravenous iron evidence that there is opportunity for both better management of anemia and cost savings in cancer patients.
There are some limitations in this study. The study is based on a model which is, by definition, a simplification of clinical actual situations. Another limitation is the assumption that the decreases of ESA consumption or number of blood transfusions are transposable from the literature studies and expert opinions. Nevertheless, the sensitivity study suggests that the conclusions are robust and stable over a range of parameters estimates and assumptions. Wide variations of these parameters were necessary to achieve the equilibrium point, particularly for parameters related to ESA consumptions.
The present cost modelling was based on carboxymaltose iron and other intravenous iron preparations were not evaluated. Important cost savings could be expected also with other intravenous preparations such iron sucrose, low molecular weight iron dextran or iron isomaltoside. Interestingly, Steiner et al.Citation34 compared ferric carboxymaltose and iron sucrose in iron deficiency anemia from a healthcare payer perspective in Switzerland. Although acquisition costs of ferric carboxymaltose was 40% higher than iron sucrose, the global cost was reduced by 35% in bowel inflammatory diseases and by 33% in patients with gynecological indications. These cost savings were related to the decrease in personnel costs associated with fewer infusions of ferric carboxymaltose.
It could also be argued that another limitation of the cost modeling was the absence of estimates for indirect costs related to anemia. Indeed, untreated anemia has clinical consequences and additional costs, which are, however, difficult to implement in modeling. Studies performed from ‘real life’ healthcare databases reported that treating a patient who is anemic is associated with considerably higher expenditures compared to a non-anemic patientCitation1,Citation3. Iron deficiency symptoms include fatigue, lethargy, or lack of energy, and it is probable that these symptoms influence negatively clinical outcomes. The cost of serum ferritin test and other tests to explore iron deficiency and the cost of iron stores replenishment with intravenous iron are low in comparison with their potential medical and cost saving consequences. Therefore, in addition to direct costs estimated in the present study, important indirect cost savings could also be expected in anemia patients receiving intravenous iron.
Finally, it is reassuring that the significant cost savings that were estimated in relation to iron supplementation, particularly in chemotherapy-induced anemia, are consistent with economic studies performed in other countries. This suggests that the results of the present study are generalizable to other countries. Thus, AuerbachCitation35 in 2008 estimated that the routine use of intravenous iron in the US could save $1301 per patient for a 12-week period over the total cost of anemia therapy. The study of Hedenus et al.Citation36 in Swedish patients with anemic lymphoproliferative disease (without chemotherapy) estimated that the decrease of ESA dosing to achieve target hemoglobin in the intravenous iron group compared to no intravenous iron group saved €1178 per patient for 12 weeks of treatment.
In conclusion, the present economic model suggests that use of intravenous iron, according to recommendations of international guidelines, is cost saving, particularly in chemotherapy-induced anemia in breast cancers.
Transparency
Declaration of funding
The study was sponsored by Vifor Pharma.
Declaration of financial/other relationships
LM and JW are employees of Vifor Pharma; the other authors have no financial interests to disclose directly or indirectly related to the research in the manuscript.
Acknowledgments
This study was presented in part at the ISPOR 16th Annual International Meeting, May 21–25, 2011, Baltimore, MD, USA. The authors would like to thank for their help Jacques N. Biot, Peter Branhaufer, Lorraine Zakin and Francis Beauvais.
Notes
*Ferinject is a registered trade name of Vifor Pharma AG, Switzerland.
References
- Lyman GH, Berndt ER, Kallich JD, et al. The economic burden of anemia in cancer patients receiving chemotherapy. Value Health 2005;8:149-56
- Nissenson AR, Wade S, Goodnough T, et al. Economic burden of anemia in an insured population. J Manag Care Pharm 2005;11:565-74
- Ershler WB, Chen K, Reyes EB, et al. Economic burden of patients with anemia in selected diseases. Value Health 2005;8:629-38
- Andrews NC. Disorders of iron metabolism. N Engl J Med 1999;341:1986-95
- Groopman JE, Itri LM. Chemotherapy-induced anemia in adults: incidence and treatment. J Natl Cancer Inst 1999;91:1616-34
- Ludwig H, Fritz E. Anemia in cancer patients. Semin Oncol 1998;25:2-6
- Littlewood TJ. Erythropoietin for the treatment of anemia associated with hematological malignancy. Hematol Oncol 2001;19:19-30
- Spielmann M, Luporsi E, Ray-Coquard I, et al. Diagnosis and management of anaemia and iron deficiency in patients with haematological malignancies or solid tumours in France in 2009–2010: The AnemOnHe study. Eur J Cancer in press
- Bierbaum BE, Callaghan JJ, Galante JO, et al. An analysis of blood management in patients having a total hip or knee arthroplasty. J Bone Joint Surg Am 1999;81:2-10
- Feagan BG, Wong CJ, Lau CY, et al. Transfusion practice in elective orthopaedic surgery. Transfus Med 2001;11:87-95
- Rosencher N, Kerkkamp HE, Macheras G, et al. Orthopedic Surgery Transfusion Hemoglobin European Overview (OSTHEO) study: blood management in elective knee and hip arthroplasty in Europe. Transfusion 2003;43:459-69
- Bong MR, Patel V, Chang E, et al. Risks associated with blood transfusion after total knee arthroplasty. J Arthroplasty 2004;19:281-7
- Seidenfeld J, Piper M, Flamm C, et al. Epoetin treatment of anemia associated with cancer therapy: a systematic review and meta-analysis of controlled clinical trials. J Natl Cancer Inst 2001;93:1204-14
- Shander A, Spence RK, Auerbach M. Can intravenous iron therapy meet the unmet needs created by the new restrictions on erythropoietic stimulating agents? Transfusion 2010;50:719-32
- Lyseng-Williamson KA, Keating GM. Ferric carboxymaltose: a review of its use in iron-deficiency anaemia. Drugs 2009;69:739-56
- Bokemeyer C, Aapro MS, Courdi A, et al. EORTC guidelines for the use of erythropoietic proteins in anaemic patients with cancer. Eur J Cancer 2004;40:2201-16
- Bokemeyer C, Aapro MS, Courdi A, et al. EORTC guidelines for the use of erythropoietic proteins in anaemic patients with cancer: 2006 update. Eur J Cancer 2007;43:258-70
- Auerbach M, Ballard H, Trout JR, et al. Intravenous iron optimizes the response to recombinant human erythropoietin in cancer patients with chemotherapy-related anemia: a multicenter, open-label, randomized trial. J Clin Oncol 2004;22:1301-7
- Pedrazzoli P, Farris A, Del Prete S, et al. Randomized trial of intravenous iron supplementation in patients with chemotherapy-related anemia without iron deficiency treated with darbepoetin alpha. J Clin Oncol 2008;26:1619-25
- Cuenca J, Garcia-Erce JA, Martinez AA, et al. Role of parenteral iron in the management of anaemia in the elderly patient undergoing displaced subcapital hip fracture repair: preliminary data. Arch Orthop Trauma Surg 2005;125:342-7
- Cuenca J, Garcia-Erce JA, Munoz M, et al. Patients with pertrochanteric hip fracture may benefit from preoperative intravenous iron therapy: a pilot study. Transfusion 2004;44:1447-52
- Bastit L, Vandebroek A, Altintas S, et al. Randomized, multicenter, controlled trial comparing the efficacy and safety of darbepoetin alpha administered every 3 weeks with or without intravenous iron in patients with chemotherapy-induced anemia. J Clin Oncol 2008;26:1611-8
- Henry DH, Dahl NV, Auerbach M, et al. Intravenous ferric gluconate significantly improves response to epoetin alfa versus oral iron or no iron in anemic patients with cancer receiving chemotherapy. The Oncologist 2007;12:231-42
- Hedenus M, Birgegard G, Nasman P, et al. Addition of intravenous iron to epoetin beta increases hemoglobin response and decreases epoetin dose requirement in anemic patients with lymphoproliferative malignancies: a randomized multicenter study. Leukemia 2007;21:627-32
- Institut National de Veille Sanitaire. Evolution de l’incidence et de la mortalité par cancer en France de 1980 à 2005. Fiche: sein. 30 Janvier 2008. Estimations à partir des données des registres du réseau FRANCIM et du CepiDC. http://www.invs.sante.fr/surveillance/cancers/mortalite_1980_2005/donnees_localisation/sein/sein.pdf. Accessed November 21, 2011
- Haute Autorité de Santé. Commission de la transparence. Taxotère. Avis du 15 Février 2006. http://www.has-sante.fr/portail/upload/docs/application/pdf/ct032531.pdf. Accessed November 21, 2011
- Institut de Veille Sanitaire. Bulletin Epidémiologique Hebdomadaire. Numéro thématique - Dépistage organisé du cancer colorectal en France. n°2–3. 13 January 2009, Paris
- Bouvier AM, Remontet L, Jougla E, et al. Incidence of gastrointestinal cancers in France. Gastroenterol Clin Biol 2004;28:877-81
- Schneider M. Fréquence de l'anémie chez les patients français atteints de tumeurs solides ou d'hémopathies malignes: résultats de l’ “European Cancer Anaemia Survey (ECAS)”. Oncologie 2005;7:397-702
- Rodgers et al. Cancer- and Chemotherapy-induced anemia. Clinical Practice Guidelines in Oncology. Version 2. 2012. National Comprehensive Cancer Network (NCCN), United States. http://www.nccn.org/professionals/physician_gls/pdf/anemia.pdf. Accessed November 21, 2011
- Auerbach M. New intravenous iron replacement therapies. Clin Adv Hematol Oncol 2010;8:688-9
- Pigeon M, Courtois J, Rigollot N and Samson S. Les médicaments les plus prescrits en France. Consensus Cardio n° 47, March 2009. http://www.consensus-online.fr/spip.php?article323. Accessed November 23, 2011
- Ludwig H, Aapro M, Bokemeyer C, et al. Treatment patterns and outcomes in the management of anaemia in cancer patients in Europe: findings from the Anaemia Cancer Treatment (ACT) study. Eur J Cancer 2009;45:1603-15
- Steiner S, Brock E, Schneider H. Budget impact of parenteral iron treatment of iron deficiency anaemia in Switzerland. Abstract no. PHM2. Value Health 2007;10:A280
- Auerbach M. Should intravenous iron be the standard of care in oncology? J Clin Oncol 2008;26:1579-81
- Hedenus M, Nasman P, Liwing J. Economic evaluation in Sweden of epoetin beta with intravenous iron supplementation in anaemic patients with lymphoproliferative malignancies not receiving chemotherapy. J Clin Pharm Ther 2008;33:365-74