
Abstract
Objectives:
To evaluate the utilization patterns of the anti-tumor necrosis factor (anti-TNF) agents Humira (adalimumab), Enbrel (etanercept), and Remicade (infliximab) in patients with rheumatoid arthritis (RA) and compare medication costs during the first year of treatment. (Humira is a registered trademark of Abbott Laboratories, IL; Enbrel is a registered trademark of Immunex Corporation, CA; and Remicade is a registered trademark of Janssen Biotech, Inc., PA).
Methods:
This retrospective analysis of medical and pharmacy claims included patients who were aged ≥18 years, had ≥2 RA diagnosis codes, and had ≥365 days of persistence with the index anti-TNF. Patients excluded had claims for anti-TNF agents within 6 months before the index date. Refill patterns for adalimumab and etanercept, number of infliximab infusions, time between infusions, and dose per infusion were analyzed for 12 months. Direct anti-TNF medication costs were compared among anti-TNFs for the initial treatment year.
Results:
Infliximab-treated patients (n = 457) were significantly older than adalimumab- (n = 337) or etanercept-treated patients (n = 902). Time between refills was longer than recommended for 28% and 30% of adalimumab and etanercept refill periods, respectively. Potential cumulative time without therapy was 33 days for adalimumab and 43 days for etanercept. Statistically significant differences in mean per-patient anti-TNF medication costs for the first year were reported for adalimumab, etanercept, and infliximab ($14,991, $13,361, and $18,139, respectively; p < 0.0001); however, a cost assessment using labeled dosing of the anti-TNF agents with optimal treatment compliance yielded comparable annual medication costs.
Limitations:
This analysis only evaluated utilization patterns for selected anti-TNF agents and was not inclusive of other medications that patients may have been using for RA. Absolute patient adherence could not be assessed due to lack of information on how patients were self-administering adalimumab and etanercept or if samples of the agents were made available.
Conclusions:
This study identified gaps in patients’ refills compared with prescriber recommendations. The infliximab-treated group had infusion patterns consistent with prescribing information. Potential clinical and economic implications of dose attenuation with adalimumab and etanercept should be explored further.
Introduction
Tumor necrosis factor inhibitors (anti-TNFs) are biologic agents used in treating rheumatoid arthritis (RA). Humira (adalimumab) and Enbrel (etanercept) are subcutaneously injected anti-TNFs, which may be self-administered, with prescribing recommendations for biweekly or weekly administration (adalimumab: 40 mg every other week with concomitant methotrexate, with potential dose frequency increase to 40 mg/week without concomitant methotrexate; etanercept: 50 mg/week with or without concomitant methotrexate)Citation1,Citation2. Infliximab is a weight-based anti-TNF approved for use with concomitant methotrexate in RA. (Humira is a registered trademark of Abbott Laboratories, IL; Enbrel is a registered trademark of Immunex Corporation, CA; and Remicade is a registered trademark of Janssen Biotech, Inc., PA). Infliximab is administered via intravenous infusion at weeks 0, 2, and 6 and every 8 weeks thereafterCitation3. Induction dosing for RA is recommended at 3 mg/kg with a potential dose increase to 10 mg/kg or dosing every 4 weeks, during the maintenance period, to optimize patient response. To date, there have not been any published head-to-head anti-TNF studies demonstrating superiority in clinical efficacy or effectiveness among adalimumab, etanercept, or infliximab in RA. A United States (US)-based systematic review concluded that there is insufficient evidence to determine which anti-TNF regimen should be preferred in first-line treatment of RACitation4. Given this insight, variable dosing and patient adherence may contribute to any differences in observed clinical effectiveness and economic outcomes.
Observational studies have compared economic differences among anti-TNFs and specifically evaluated infliximab dosing. Comparative cost analyses have reported annual infliximab treatment costs in patients with RA to be significantly higher than those of adalimumab or etanercept, with an estimate as high as 55% more costlyCitation5–9. Health plan dosing studies have reported patients treated with infliximab receiving induction and maintenance doses consistent with dosages recommended by the US Food and Drug Administration (FDA)Citation10–14. A retrospective chart review of infliximab use in a large western US managed care organization found average infliximab induction and maintenance doses of 3.5 ± 0.6 mg/kg and 4.2 ± 1.4 mg/kg, respectivelyCitation10. Braid et al.Citation11 examined Medicare claims data from 2001–2003, reporting that the average infliximab utilization was 366.7 mg and a mean of 7.1 infusions/year; 78% of all infliximab utilization was <400 mg. A separate study of patients with RA treated in 16 rheumatology clinics between 1999 and 2002 showed mean induction and maintenance doses of 3.38 mg/kg vs 4.51 mg/kg (p < 0.001)Citation12. Additionally, analysis of managed care data has reported an infliximab adherence rate of 80.9%Citation15.
The literature is limited regarding adherence evaluations in patients with RA who are prescribed adalimumab or etanercept. A systematic literature review of adherence with biologics in RA highlighted 4 studies reporting adalimumab or etanercept adherence rates in US data sources ranging from 52–85% (with 41–51% of patients achieving a medication possession ratio ≥80%)Citation15,Citation16. These data reveal variable adherence rates for adalimumab and etanercept and signal potential patient compliance challenges, as evidenced by nearly one-half of patients having medication possession ratios <80%. Evaluating refill patterns for adalimumab and etanercept provides a different discernment of adherence. This retrospective analysis evaluated refill patterns for adalimumab and etanercept as well as dosing and infusion patterns for infliximab, and it compared anti-TNF costs in patients with RA persistently treated during the first year of therapy.
Patients and methods
Sample selection
Medical and pharmacy claims from January 1, 2000, to December 31, 2006, were obtained from the PharMetrics LifeLink Health Plan DatabaseCitation17, a national commercial database with claims from >80 health plans. The first claim for the anti-TNF agent served as the index date for each patient. Patients included in the analysis were aged ≥18 years, were continuously enrolled in a health plan for 6 months pre-index and 12 months post-index, had ≥2 International Classification of Diseases, Ninth Edition, Clinical Modification (ICD-9-CM) diagnosis codes (714.xx) for RA during the pre-index period, had no pre-index biologics (i.e., infliximab, etanercept, adalimumab, abatacept, or rituximab), and had ≥365 days of persistence (i.e., number of days between the first and last claims for index anti-TNF agent). Exclusion criteria included: a diagnosis of ankylosing spondylitis, psoriatic arthritis, psoriasis, Crohn’s disease, or ulcerative colitis at any time; post-index anti-TNF switching; or an abatacept or rituximab claim at any time. Data were assessed for the first year of persistent treatment. Baseline demographics and RA disease severity were reported. Pharmacy refill patterns, infusion patterns, and anti-TNF medication costs were evaluated for the 12-month post-index period.
Comorbidity and RA disease severity
Comorbidities were measured using the Charlson Comorbidity Index (CCI)Citation18, a weighted index that allows for prospective comorbidity and mortality risk classification in longitudinal studies. As the CCI score increases, a patient’s risk of comorbid mortality increases. Disease severity was measured using MedStat disease stagingCitation19, which employs ICD-9-CM codes to classify patients with a particular disease who require similar treatment and have similar expected outcomes. Disease severity was classified using a 5-point scale (Stage 0 = no complications, Stage 1 = specific disease with no complications, Stage 2 = specific disease with local complications, Stage 3 = specific disease with multiple sites of systemic complications, Stage 4 = death). The MedStat methodology uses a cumulative approach; for example, stage 1.01 for RA is based on ICD-9-CM codes 714.0, 714.2, and 714.4, which correspond to the American College of Rheumatology diagnostic criteria of a history of morning stiffness and 1 of the following: 3 joints with swelling or effusion, swelling or effusion of the hand or wrist joints, symmetrical bilateral joint swelling, subcutaneous nodules, RA (as evidenced by radiograph of any joint), or rheumatoid factor titer of 1:160. In addition, to have a disease stage of 3.0, a patient must have been previously classified as stage 2.0. Once an individual meets the criteria for a particular stage, he or she cannot revert to a lesser stage. This methodology has been used to compare disease severity in retrospective analyses when detailed clinical outcome data were unavailableCitation20.
Adalimumab and etanercept pharmacy refill measures
Adalimumab and etanercept pharmacy refills were assessed by capturing mean number of treatment days authorized by the prescriber and submitted on the pharmacy claim in the days supply field and by performing a prescription gap analysis calculation of the length of time between the initial and subsequent fill service dates. The sum of the difference between the actual time to refill and the prescriber-authorized days supply was used to calculate the gaps (or potential cumulative time without therapy).
Formula for prescription gap analysis
Mean and median numbers of adalimumab and etanercept prescription fills per patient for the first year were also examined. Percentages of patients refilling adalimumab or etanercept prescriptions during the first year were graphically displayed.
Infliximab infusions and dosing measures
Infliximab infusions were evaluated by calculating mean number of days between infusions billed using Healthcare Common Procedure Coding System code J1745. Mean number of infusions by treatment period was reported. A proxy formula was used to estimate infliximab dose at each infusion, because neither doses nor units were recorded on the procedure claims. Infliximab doses were calculated by dividing the health plan’s allowed amount for each claim by the wholesale acquisition cost for a 100-mg vial during the year of claim payment. The health plan’s allowed amount on each claim included the total amount paid by the plan and the patient. The health plan’s allowed amount was used because it represents the full cost of infliximab billed to the plan and will not overinflate costs to the same degree as charged amountsCitation21. The allowed amount, however, does not represent the costs that a health plan reimbursed for infliximab, as that information is typically not publicly available. Only patients with complete claim information (i.e., no negative or null value in the allowed amount field) were included in the dosing analysis. Results for infliximab infusions and doses were reported for induction (index to day 56), maintenance (day 57 to day 365), and the first year overall (index to day 365).
Direct anti-TNF medication cost assessments
Inflation-adjusted plan-paid anti-TNF medication costs were reported for the first year. Adalimumab and etanercept direct medication costs included costs on pharmacy claims. Infliximab direct medication costs included drug costs and any administration/infusion fees submitted on the same medical claim. A secondary cost analysis was conducted by calculating annual costs for each anti-TNF based on expected cumulative utilization for 1 year of persistent treatment (using dosing within the FDA-approved prescribing information and assuming 100% treatment adherence). Adalimumab cost calculations were based on a dosage of 40 mg every other weekCitation1. Etanercept cost calculations were based on a dosage of 50 mg once weeklyCitation2. Infliximab cost calculations were based on initial doses of 3 mg/kg administered intravenously at weeks 0, 2, and 6 and every 8 weeks thereafter, with a dose increase to 5 mg/kg (every 8 weeks) after 6 monthsCitation22. The cost of the entire infliximab vial and administration costs were accounted for in calculations.
Statistical analyses
Pairwise comparisons were used to assess differences in baseline characteristics using t tests (generalized linear models). Differences in costs were tested using Wilcoxon rank sum tests. Statistical significance was defined as a 2-sided α-level of ≤0.05. All statistical analyses were performed using SAS release 9.1.3 (SAS Institute, Inc., Cary, NC).
Results
Demographic and clinical characteristics of RA patient sample
Data from 1696 patients with RA (adalimumab = 337, etanercept = 902, infliximab = 457) were included. The mean age overall was 49.9 years; 76% of patients were women. Infliximab-treated patients were significantly older than adalimumab- or etanercept-treated patients (52.5, 49.2, and 48.8 years, respectively; both comparisons, p < 0.0001). Infliximab-treated patients had statistically higher RA disease staging compared with their etanercept-treated counterparts (1.57 vs 1.46, respectively; p = 0.008), but no difference was found when compared with adalimumab (p = 0.0739). No significant differences were noted among mean CCI scores ().
Table 1. Patient clinical and demographic characteristics.
Adalimumab and etanercept pharmacy refill measures
Among patients who received adalimumab, mean number of prescriber-authorized treatment days on adalimumab pharmacy claims was 34 days. Of etanercept users, mean number of prescriber-authorized treatment days on etanercept pharmacy claims was 32 days. Actual time between prescription refills was longer than expected, based on the prescriber-authorized days supply, for 28% of all adalimumab refill periods and 30% of all etanercept refill periods ().
Table 2. Pharmacy refill patterns for adalimumab and etanercept.
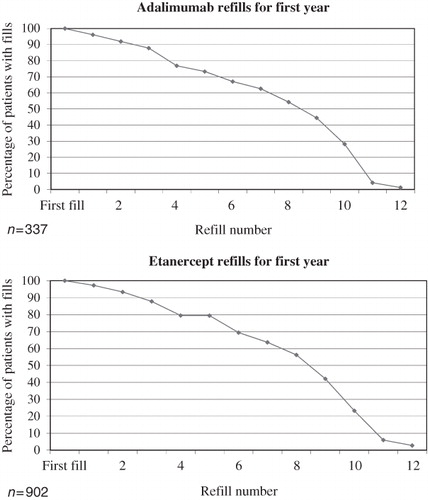
Gap analyses revealed that the potential cumulative time without therapy was 33 days for adalimumab and 43 days for etanercept within the 12-month post-index period. The mean (standard deviation [SD])/median number of pharmacy fills per patient for the first year were 9.97 (SD 3.79)/11 for adalimumab and 9.77 (SD 3.81)/11 for etanercept. The percentage of patients continuing to refill adalimumab and etanercept prescriptions decreased during the first year ().
Figure 1. Pharmacy refill patterns for adalimumab and etanercept during the first year of treatment.
Infliximab infusions and dosing
The majority of infliximab-treated patients (98.5%; n = 450) received no more than 8 infusions during the first year of treatment. The mean (SD)/median numbers of infusions were 2.71 (SD 0.61)/3, 5.15 (SD 1.28)/5, and 7.86 (SD 1.48)/8 for the induction, maintenance, and first-year periods, respectively. The mean times between induction infusions were as follows: 1st and 2nd = 19 days; 2nd and 3rd = 29 days. The mean times between maintenance infusions spanned 52 to 57 days ().
Table 3. Time intervals between infliximab infusions (n = 457).
A subset of 425 evaluable infliximab-treated patients with complete claim information was included in the dosing analysis. Calculated mean (SD)/median infliximab doses per infusion were 397 (SD 164) mg/370 mg, 455 (SD 193) mg/405 mg, and 437 (SD 168) mg/397 mg for induction, maintenance, and first-year periods, respectively.
Direct anti-TNF medication cost assessments
Significant differences in mean and median direct anti-TNF medication costs existed among the treatment groups. Mean (SD) anti-TNF medication costs for the first year were $14,991 (SD $9396), $13,361 (SD $9182), and $18,139 (SD $9958) for adalimumab, etanercept, and infliximab, respectively (p < 0.0001). Median annual anti-TNF medication costs were $14,979, $14,225, and $17,012 for adalimumab, etanercept, and infliximab, respectively (p < 0.0001). A post hoc analysis of the distribution of cost data for each of the anti-TNFs showed no differences in how the cost data were skewed among the agents. A secondary cost assessment showed that estimated annual costs of adalimumab, etanercept, and infliximab were comparable, even when accounting for administration costs ($18,886, $20,190, and $18,533, respectively), if the anti-TNFs were used according to the prescribing instructions ().
Table 4. Annual cumulative anti-TNF cost considerations using doses within the United States FDA-approved prescribing information (first year of persistent treatment).
Discussion
This study was conducted to investigate adalimumab, etanercept, and infliximab utilization patterns while also comparing medication costs in RA. The strengths of this study included: exclusion of patients with other conditions for which the anti-TNFs are indicated and may have different recommended dosing as a confounder of the results, selection of patients with RA newly starting the anti-TNF, and inclusion of patients maintaining persistence on the initiated anti-TNF without switching to another anti-TNF.
Results revealed insights regarding real-world use of these drugs. Although higher treatment costs were associated with infliximab, this may have been influenced by observed differences in patient populations, including disease severity. Examining costs of persistent treatment (with 100% treatment adherence) according to labeled dosing, however, revealed minute numerical differences in costs of all 3 anti-TNF agents. The difference between infliximab’s mean observed cost and expected annual cost, when dosed within prescribing guidelines, was −$394. Differences between mean observed costs and expected annual costs, relative to labeled dosing, for adalimumab and etanercept were approximately 10 to 17 times that observed for infliximab (−$3895 and −$6829, respectively). Given the assumed patient weight in the modeled expected annual cost calculation for infliximab, these differences would be reduced if the assumed patient weight increased.
Although mean age and female predominance in the overall study population were consistent with published clinical trial and observational studies of patients with RACitation5–10,Citation12,Citation13,Citation23,Citation24, other differences in patient types were observed. Infliximab-treated patients were significantly older than adalimumab- and etanercept-treated patients and had a higher RA disease stage compared with etanercept, indicative of a more complex disease profile. Similar demographic and clinical differences among patients with RA receiving anti-TNF agents have been reported elsewhereCitation23,Citation24. Additionally, it has been reported that infliximab-treated patients may present with statistically higher medical and pharmacy costs at baseline compared with patients treated with etanerceptCitation23. These differences may drive utilization of healthcare services and total costs, in addition to drug costs, and should be considered in future comparative analysesCitation25,Citation26.
Infliximab infusions and dosing results reported real-world utilization consistent with prescribing information; patients appeared to receive infliximab according to the FDA-recommended schedule of weeks 0, 2, and 6 and every 8 weeks thereafter. Dose increases and more frequent administrations are also supported by the FDA-approved prescribing information and have been proven to have an associated clinical benefitCitation1,Citation27–32. This current analysis suggests that while there was a dose increase from induction to maintenance, the increase was modest. Infliximab dose increases have been cited in the literature as occurring frequently within managed care and having an association with increased costsCitation33,Citation34; however, researchers recently hypothesized that dose increases within the FDA-recommended range and/or physician administration may be associated with significantly longer treatment persistence when compared with adalimumab and etanerceptCitation24. Another study reported that a smaller proportion of patients receiving infliximab discontinued therapy compared with patients on etanerceptCitation23.
Furthermore, persistency with anti-TNF agents has a directly proportional effect on pharmacy costs and an inversely proportional effect on non-pharmacy costsCitation35. In a study of 1242 patients with RA receiving infliximab, etanercept, or adalimumab, pharmacy costs were higher, and all other non-pharmacy costs (e.g., inpatient, outpatient, labs) were lower in patients with ≥80% treatment persistency compared with patients with <80% treatment persistency. Investigators also found that patients receiving infliximab had significantly higher persistence than patients receiving adalimumab or etanerceptCitation35.
The current analysis was conservative, as persistency was normalized (as an inclusion criterion) across treatment groups. Despite this persistency requirement, there was variance in the refill patterns for adalimumab and etanercept. Approximately one-third of actual pharmacy fills had a longer time to patient refill. Because of this discrepancy between the prescriber recommendation and the patients’ refill behavior, some adalimumab-treated patients may have had an approximate cumulative time of 5 weeks without medication over the course of the first year of treatment; some etanercept-treated patients may have had an approximate cumulative time of 6 weeks without medication. These refill patterns may signal questionable adherence behavior, contributing to under-utilization of adalimumab and etanercept, and require further investigation.
Lastly, plan-paid medication costs were significantly different for adalimumab, etanercept, and infliximab, with infliximab associated with higher costs. While the observed cost differences are consistent with other studiesCitation4–7,Citation9,Citation33,Citation35–37, this analysis attempted to address cost in the context of treatment adherence. Our evaluation of costs in the context of observed treatment adherence is a methodological approach distinctive from that of a recent analysis using the same database. Schabert et al.Citation9 also used the PharMetrics LifeLink Health Plan DatabaseCitation17 to calculate annual treatment costs of adalimumab, etanercept, and infliximab. In their analysis, the yearly observed treatment costs in RA were $17,700, $14,314, and $20,390 for adalimumab, etanercept, and infliximab, respectively. The authors attributed the higher observed costs of adalimumab and infliximab to potential dose increases but did not include evidence of observed dose increases in the analysis nor consider reduced treatment adherence as a potential driver of lower observed costs. Cost differences in this current study may be associated with differences in observed utilization patterns – more specifically, inconsistent adalimumab and etanercept refill behavior and consistent infliximab administrations during the first year. Health plans may have been paying less for adalimumab and etanercept prescriptions, but patients may have been using them in a manner inconsistent with prescribing information.
As reported in , 1-year anti-TNF agent cost considerations are comparable when administered and taken by the patient according to prescribing information. Similar findings of comparable cost, in the context of optimal dosing and adherence, have been reported by the Agency for Healthcare Research and QualityCitation38. Previous adherence research with the anti-TNF agents has shown that patient adherence among Medicare or commercial enrollees with RA is higher with infliximab than with etanerceptCitation22. Lower treatment adherence could put the patient at risk for inadequate control of RA symptoms and disease activity and could influence the use and cost of outpatient and inpatient services. Future research should be directed to exploring the impact of inconsistent refill behavior on clinical outcomes and total payer costs, including medical and pharmacy, rather than focusing on only pharmacy costs.
Limitations
Several limitations exist within this analysis. This study was limited to the first year of anti-TNF treatment, partly due to the study-defined persistence requirement. This represents a unique method in contrast to other observational studiesCitation5–13. Given that patients with RA may be treated for variable time periods with the selected index anti-TNF agent, the 1-year persistence requirement for the index anti-TNF agent provided a more informative comparison of initial utilization patterns. This persistency requirement, however, excluded individuals who discontinued treatment or switched treatments.
Limiting results to a 1-year time frame prohibits any conclusions regarding infusion and refill patterns beyond the first year of anti-TNF therapy. Other disease severity measures and comorbidity instruments, such as the Index of Coexistent Diseases and the RA Duke Severity of Illness Checklist, have greater specificity for predicting health outcomes and costs in RACitation39,Citation40 but were not feasible for use in a claims-based analysis. This study was conducted by analyzing claims retrospectively from an administrative database lacking clinical measures, reasons for patients refilling later than expected, or indicators of patient death.
This analysis was limited in scope, as it evaluated utilization patterns only for selected anti-TNF agents and did not include other concomitant medications that patients may have been using for RA. The perspective of this analysis was also limited to that of the health plan’s pharmacy budget perspective and, therefore, did not include other costs relevant from a patient perspective (e.g., co-payments, co-insurance, time and costs associated with travel). Future analyses may want to incorporate these types of direct and indirect costs to estimate the total cost of care for anti-TNFs.
Lastly, absolute patient adherence could not be assessed because we did not have information on how patients were self-administering adalimumab and etanercept or if samples of the agents were made available. This analysis was limited to a refill pattern assessment, which provided a window into theoretical patient adherence, with potential drug on-hand as an intermediary measure. The measurement of absolute patient adherence with the self-administered anti-TNF agents, accounting for all possible means of patients acquiring the drug, is a warranted area of research.
Conclusions
This observational study reported differing RA patient populations based on index anti-TNF agents. Refill patterns for adalimumab and etanercept revealed gaps in the time that patients refilled compared to prescriber recommendations; however, infliximab infusion patterns were consistent with prescribing information. Future comparative effectiveness and economic research of anti-TNF agents should adjust for differences in baseline characteristics and observed compliance with prescriber recommendations. Potential clinical and economic implications of dose attenuation with adalimumab and etanercept should be explored further.
Transparency
Declaration of funding
This study was funded by Janssen Scientific Affairs, LLC, Horsham, PA.
Declaration of financial relationships
CTC and RSM have disclosed that they are employees of Janssen Scientific Affairs, LLC. AKC has disclosed that he has no relevant financial relationship to declare.
Acknowledgments
The authors would like to thank Cynthia Schmeichel, BS, MS, PhD, and Mike Ingham, MSc, from Janssen Scientific Affairs, LLC, for their careful review and editorial assistance with the manuscript, as well as Boxiong Tang, MD, for his contribution to the design and interpretation of the study at the time of his employment with the sponsor.
References
- Humira (adalimumab) [package insert]. North Chicago, IL: Abbott Laboratories, 2009
- Enbrel (etanercept) [package insert]. Thousand Oaks, CA: Immunex Corporation, 2009
- Remicade (infliximab) [package insert]. Horsham, PA: Centocor Ortho Biotech Inc, 2010
- Donahue KE, Gartlehner G, Jonas DE, et al. Systematic review: comparative effectiveness and harms of disease-modifying medications for rheumatoid arthritis. Ann Intern Med 2008;148:124-34
- Bullano MF, McNeeley BJ, Yu YF, et al. Comparison of costs associated with the use of etanercept, infliximab, and adalimumab for the treatment of rheumatoid arthritis. Manag Care Interface 2006;19:47-53
- Wu E, Chen L, Birnbaum H, et al. Cost of care for patients with rheumatoid arthritis receiving TNF-antagonist therapy using claims data. Curr Med Res Opin 2007;23:1749-59
- Daniel GW, McNeeley B, Huang X, et al. Dosing patterns and health plan costs among RA patients treated with tumor necrosis factor antagonists. Poster presented at: American College of Rheumatology; San Francisco, CA; October 24–29, 2008
- Kievit W, Adang EM, Fransen J, et al. The effectiveness and medication costs of three anti-tumour necrosis factor α agents in the treatment of rheumatoid arthritis from prospective clinical practice data. Ann Rheum Dis 2008;67:1229-34
- Schabert VF, Watson C, Gandra SR, et al. Annual costs of tumor necrosis factor inhibitors using real-world data in a commercially insured population in the United States. J Med Econ. 2012;15: published online 25 November 2011, doi:10.3111/13696998.2011.644645
- Stockl K, Jarrar M, Tandon N. Dosing patterns of anti-TNF therapy in patients with rheumatoid arthritis in a managed care setting. Dis Manag Health Outcomes 2004;12:189-96
- Braid MJ, Ziskind M, Tandon N. Infliximab dosing and cost analysis of Medicare rheumatoid arthritis patients. Poster presented at: The European League Against Rheumatism; Vienna, Austria; June 8–11, 2005
- Abarca J, Malone DC, Armstrong EP, et al. Longitudinal analysis of the use of etanercept versus infliximab determined from medical chart audit. J Manag Care Pharm 2004;10:538-42
- Wu E, Chen L, Birnbaum H, et al. Retrospective claims data analysis of dosage adjustment patterns of TNF antagonists among patients with rheumatoid arthritis. Curr Med Res Opin 2008;24:2229-40
- Nair KV, Tang B, Van Den Bos J, et al. Categorization of infliximab dose changes and healthcare utilization and expenditures for patients with rheumatoid arthritis in commercially-insured and Medicare-eligible populations. Curr Med Res Opin 2009;25:303-14
- Blum MA, Koo D, Doshi JA. Measurement and rates of persistence with and adherence to biologics for rheumatoid arthritis: a systematic review. Clin Ther 2011;33:901-13
- Koncz T, Pentek M, Brodszky V, et al. Adherence to biologic DMARD therapies in rheumatoid arthritis. Expert Opin Biol Ther 2010;10:1367-78
- PharMetrics LifeLink Health Plan Database. PharMetrics, Inc. Watertown, MA: IMS Health, 2010
- Charlson ME, Pompei P, Ales KL, et al. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis 1987;40:373-83
- Medstat Disease Staging Software Version 5.24. Ann Arbor, MI: Thomson Medstat Inc, 2006
- Gonnella JS, Louis DZ, Gozum MV, et al, eds. Disease staging: clinical criteria. Ann Arbor, MI: The MEDSTAT Group, Inc, 2003
- Ollendorf DA, Lidsky L. Infliximab drug and infusion costs among patients with Crohn’s disease in a commercially-insured setting. Am J Ther 2006;13:502-6
- Stern R, Wolfe F. Infliximab dose and clinical status: results of 2 studies in 1642 patients with rheumatoid arthritis. J Rheumatol 2004;31:1538-45
- Harley CR, Frytak JR, Tandon N. Treatment compliance and dosage administration among rheumatoid arthritis patients receiving infliximab, etanercept, or methotrexate. Am J Manag Care 2003;9(6 Suppl):S136-43
- Yazici Y, Krasnokutsky S, Barnes JP, et al. Changing patterns of tumor necrosis factor inhibitor use in 9074 patients with rheumatoid arthritis. J Rheumatol 2009;36:907-13
- Lajas C, Abasolo L, Bellajdel B, et al. Costs and predictors of costs in rheumatoid arthritis: a prevalence-based study. Arthritis Rheum 2003;49:64-70
- Michaud K, Messer J, Choi HK, et al. Direct medical costs and their predictors in patients with rheumatoid arthritis: a three-year study of 7,527 patients. Arthritis Rheum 2003;48:2750-62
- Rahman MU, Strusberg I, Geusens P, et al. Double-blinded infliximab dose escalation in patients with rheumatoid arthritis. Ann Rheum Dis 2007;66:1233-38
- Durez P, Van den Bosch F, Corluy L, et al. A dose adjustment in patients with rheumatoid arthritis not optimally responding to a standard dose of infliximab of 3 mg/kg every 8 weeks can be effective: a Belgian prospective study. Rheumatology (Oxford) 2005;44:465-8
- van VollenhovenRF, Brannemark S, Klareskog L. Dose escalation of infliximab in clinical practice: improvements seen may be explained by a regression-like effect. Ann Rheum Dis 2004;63:426-30
- Sidiropoulos P, Bertsias G, Kritikos HD, et al. Infliximab treatment for rheumatoid arthritis, with dose titration based on disease activity score: dose adjustments are common but not always sufficient to assure sustained benefit. Ann Rheum Dis 2004;63:144-8
- Flendrie M, Creemers MCW, van Riel PLCM. Titration of infliximab treatment in rheumatoid arthritis patients based on response patterns. Rheumatology (Oxford) 2007;46:146-9
- Ariza-Ariza R, Navarro-Sarabia F, Hernández-Cruz B, et al. Dose escalation of the anti-TNF-α agents in patients with rheumatoid arthritis. A systematic review. Rheumatology (Oxford) 2007;46:529-32
- Gilbert TD Jr., Smith D, Ollendorf DA. Patterns of use, dosing, and economic impact of biologic agent use in patients with rheumatoid arthritis: a retrospective cohort study. BMC Musculoskelet Disord 2004;5:36
- Ollendorf DA, Massarotti E, Birbara C, et al. Frequency, predictors, and economic impact of upward dose adjustment of infliximab in managed care patients with rheumatoid arthritis. J Manag Care Pharm 2005;11:383-93
- Tang B, Rahman M, Waters HC, et al. Treatment persistence with adalimumab, etanercept, or infliximab in combination with methotrexate and the effects on health care costs in patients with rheumatoid arthritis. Clin Ther 2008;30:1375-84
- Weycker D, Yu EB, Woolley JM, et al. Retrospective study of the costs of care during the first year of therapy with etanercept or infliximab among patients aged ≥65 years with rheumatoid arthritis. Clin Ther 2005;27:646-56
- Ollendorf DA, Klingman D, Hazard E, et al. Differences in annual medication costs and rates of dosage increase between tumor necrosis factor-antagonist therapies for rheumatoid arthritis in a managed care population. Clin Ther 2009;31:825-35
- Effective Healthcare: Rheumatoid Arthritis Medicines. A guide for adults. Agency for Healthcare Research and Quality. Consumer summary guide. Rockville, MD: AHRQ Publication Number 08-EHC004-2A, 2008
- Gabriel SE, Crowson CS, O’Fallon WM. A comparison of two comorbidity instruments in arthritis. J Clin Epidemiol 1999;52:1137-42
- Navarro-Cano G, del Rincón I, Pogosian S, et al. Association of mortality with disease severity in rheumatoid arthritis, independent of comorbidity. Arthritis Rheum 2003;48:2425-33