
Abstract
Objective:
A pharmacoeconomic analysis was undertaken to determine costs, consequences, and cost-effectiveness of a partially hydrolyzed 100% whey-based infant formula, NAN-HA®, manufactured by Nestlé S.A, Switzerland (PHF-W), branded under BEBA HA® in Switzerland, in the prevention of atopic dermatitis (AD) in ‘at risk’ Swiss children when compared to standard cow’s milk formula (SF).
Methods:
Based on a 12-month time horizon including 6 months of formula consumption, an economic model was developed synthesizing treatment pathways, resource utilization, and costs associated with the treatment of AD in healthy ‘at risk’ Swiss newborns who could not be exclusively breastfed. Model inputs were retrieved from the literature, official formularies, and expert opinion. The treatment pathways considered a medical treatment approach, supplemented in some instances by a change of formula. The final outcome was the expected cost per avoided case of AD, yielding an incremental cost effectiveness ratio (ICER) for PHF-W vs SF. Outcomes were presented from three perspectives: the Swiss public healthcare system (MOH), the subject’s family, and society (SOC). A secondary analysis compared PHF-W to whey-based extensively hydrolyzed formula (EHF) in prevention.
Results:
The model yielded 1653 avoided AD cases by selecting PHF-W over SF in a birth cohort of 22,933 ‘at risk’ infants. The base case analyses generated an expected ICER of CHF 982 from the MOH perspective as well as savings of CHF 2202 and CHF 1220 from the family and SOC perspectives, respectively. PHF-W yielded CHF 11.4M savings against EHF when the latter was assumed to be used in prevention. One-way and probabilistic sensitivity analyses confirmed the robustness of the model.
Conclusion:
Under a range of assumptions, this analysis has established the dominance from the family and societal perspectives and cost-effectiveness from the MOH perspective of PHF-W vs SF in the prevention of AD among ‘at risk’ Swiss infants.
Introduction
One of the most common skin disorders seen in infants and children, atopic dermatitis (AD) is an inflammatory, non-contagious, and pruritic skin disorder which has its onset during the first 6 months of lifeCitation1. The prevalence amongst children aged 6–7 years as measured in the International Study of Asthma and Allergies in Childhood (covering 66 centers in 37 countries distributed throughout the world) ranged between 2.6–22%Citation2. The lifetime prevalence of AD in North America and industrialized European countries is estimated at 10–20% in younger school childrenCitation3. Infants who have a parent or sibling with a history of allergy are deemed to be at higher risk of developing AD. For those subjects, the risk of developing allergic manifestations is roughly one in three, further increasing to 70% if both parents have a history of allergyCitation4–6. Clinical and experimental data indicate that early exposure to dietary allergens may be crucial for the development of allergies such as food allergies and ADCitation7.
The World Health Organization (WHO) and numerous regional and national guidelines (including those of Switzerland) recommend exclusive breastfeeding for the first 4–6 months of lifeCitation8–13. When the infant cannot be breastfed or breastfeeding duration is shorter than recommended, Swiss infants are assigned infant formulas, in most cases, standard cow’s milk-based infant formulas (SF). Extensively hydrolyzed infant formulas (EHF) have been indicated for treatment and, in some countries, prevention of cow’s milk and food allergy. Amino acid-based formulas (AAF) are available for allergy treatment, but at a much higher cost.
Partially hydrolyzed formula is thought to have similar hypoallergenic properties as EHF but is associated with lower rates of discontinuation due to a host of factors such as better taste, better texture, and less bitternessCitation6,Citation7,Citation14. So far, only one specific brand of 100% whey-based partially hydrolyzed formula, NAN HA®, manufactured by Nestlé S.A, Switzerland (PHF-W) and branded under BEBA HA® in Switzerland, has been shown in randomized trials to be effective in the prevention of AD.
Early nutritional intervention with PHF-W or EHF in ‘at risk’ children has significant influence on the incidence of AD and, in cases where breastfeeding was insufficient, a hypoallergenic formula was advisedCitation15. This statement is supported by two recently published meta-analyses: the first by Szajewska and HorvathCitation16, the second by Alexander and CabanaCitation17. In the first meta-analysis, a significantly higher relative risk (RR) of developing AD was reported for subjects consuming SF vs PHF-W (RR of PHF-W vs SF of 0.68 at 12 months, p-value = 0.04)Citation16. The second meta-analysis reported a statistically significant risk reduction of 44% with PHF-W for atopic manifestations while a sub-group analysis of AD results yielded a reduced incidence of AD by 55% [30–70%] for PHF-W vs SFCitation17.
In 2009, Baehler et al.Citation8 published, on behalf of the Nutrition Committee of the Swiss Society of Pediatrics and the Swiss Association of Pediatric Immunologists and Allergists, a set of guidelines pertaining to the prevention of allergic manifestations in early childhood in Switzerland, with a particular emphasis on nutrition. In this set of guidelines, the authors argued that ‘at risk’ infants who are not exclusively breastfed should be fed partially hydrolyzed formula as an alternative to SF, and that EHF preparations should only be given in special cases, after consulting a pediatrician.
According to the literature, treatment for AD accounts for a significant amount of health services financial resources and clinical time as well as placing a burden on the child, family, and societyCitation18. KempCitation19 has concluded that moderate-to-severe AD had a greater negative impact than type 1 diabetes mellitus on the family of an affected child. A 2006 study of 33 Italian children with AD reported a mean cost of CHF 1254 per year for the familyCitation20. Two studies were published for German settings. The first was published in 1999 and estimated the annual cost of AD to be DM 4827 from the societal perspectiveCitation21. The second study (2003), based on 91 German children, reported annual healthcare costs ranging from $164 in mild cases to $911 in severe casesCitation22.
A previously published pharmacoeconomic analysis (PEA) by our group reported the cost-effectiveness of PHF-W in the prevention of AD for ‘at risk’ children in FranceCitation23. A review of the published literature did not yield any economic evaluation on the prevention of AD in Swiss children. The present study is a PEA focusing on the Swiss setting with a view to determining the costs, consequences, and cost-effectiveness of PHF-W vs SF in the prevention of AD in ‘at risk’ children.
Methods
Product of interest
The product of interest was PHF-W and the main comparator was SF. Whey-based EHF (EHF-Whey) and AAF were included as alternatives to PHF-W or SF in some treatment pathways of the base case economic model, while EHF-Whey was also subject to secondary analyses exploring a scenario wherein it was also indicated for prevention. Casein-based EHF was not taken into account in the present study since it is not indicated for younger children in Switzerland.
Disease of interest
This study focused on AD as it was found to be the most quantifiable of all allergic manifestations which could be associated with milk consumption.
Population of interest
The study centered on healthy yet ‘at risk’ subjects ranging from newborns to 3-year olds who were not exclusively breastfed; ‘at risk’ were children with at least one parent or sibling with a diagnosed or reported history of allergies.
Perspective
Three perspectives were considered in this economic evaluation. The first perspective was that of the Swiss public healthcare system, herein designated as the Ministry of Health (MOH), in which all the resource utilization and costs attributed to the MOH were taken into account.
Given the aforementioned economic and personal burden that AD inflicts on the entire family of the affected subjects, the second perspective focused on the costs attributable to the family of the child. The third perspective, that of society as a whole, included both the MOH and the family’s perspectives.
Time horizon
In the base case analysis, a time horizon of 12 months, including an initial 6 months of formula consumption, was adopted as it represented the time during which most cases of AD first occur while extending beyond the period of milk consumption. Sensitivity analyses (SAs) were carried out by changing the time horizon to 6 months (the period of initial milk consumption) and to 3 years, at which point most AD symptoms would have abated or may have started to develop into other allergic manifestations such as atopic rhinitis or asthma.
Type of economic evaluation
A cost-effectiveness approach was chosen as it offered the best means to measuring the costs and outcomes that are most relevant to both the children and their parents as well as the MOH.
Clinical outcomes
The occurrence of AD was determined by obtaining the incidence rate of AD with one preparation, e.g., SF, and the RR of developing AD when comparing one preparation to the other, e.g., PHF-W vs SF. These incidence rates and RRs were reported in a meta-analysis by Szajewska and HorvathCitation16.
A recently published brief report by Iskedjian et al.Citation24 provided an explanation of how RRs of developing AD at 6, 12, 24, and 36 months in subjects who had consumed PHF-W vs SF, were extracted from both incidence and cumulative incidence rates at those same time points.
The total cases of AD attributable to each formula of interest were obtained and then converted into the final clinical outcome of the model, i.e., the avoided cases of AD when consuming PHF-W rather than SF. Using avoided cases as a benchmark was required, as this economic evaluation explored the prevention of AD when PHF-W was consumed.
Economic outcomes and incremental ratios
The intermediate economic outcomes were the aggregated costs associated with the MOH perspective, the perspective of the family, and the societal perspective.
The expected cost per avoided case of AD was the final outcome of the cost-effectiveness analysis. This outcome was expressed as an incremental cost per avoided case of AD, which would serve as the incremental cost-effectiveness ratio (ICER) of this economic evaluation. The ICER in this study was the difference in costs between PHF-W and SF divided by the negative value of the difference in the number of cases between PHF-W and SF. The application of a negative coefficient is required as this is an analysis of avoided or preventive cases. The simplified mathematical formulation of the ICER is summarized below:
Expert opinion
Expert opinion was sought by consulting a Swiss clinical expert (Dr Dominique Belli) with an expertise in Pediatrics and Nutrition at a teaching hospital. Expert opinion was required in order to determine and authenticate treatment pathways and secondly to identify and help estimate resources utilized in the management of AD symptoms in a Swiss setting.
Summary of model structure
The cost-effectiveness analysis was carried out by using MS Excel® 2003 to construct a spreadsheet-based decision-analytic economic model (presented in ), depicting the medical practices associated with the treatment of AD in Switzerland.
Figure 1. Decision tree model depicting the treatment patterns of atopic dermatitis in Switzerland in a population ranging from newborns to 3-year olds.
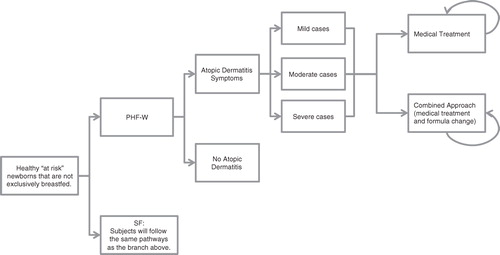
The model applied a series of 3-month cycles, starting with the birth cohort. Subjects were assigned to one of two arms receiving either PHF-W or SF allowing for a juxtaposition of costs and consequences between the two formulas.
Using the AD incidence rates adapted by Iskedjian et al.Citation24 from the Szajewska and HorvathCitation16 meta-analysis, subjects within each arm were then divided into two groups: those subjects with AD and those subjects without AD. For those subjects who were affected by AD, a disease severity was assigned as per expert opinion.
Subjects with AD were sent to their first medical visit and presented with an age-specific plan to manage their AD. At 6 months of age or younger, subjects were treated in one of two ways: a medical treatment approach or an approach combining the medical treatment approach with one or more changes of infant formula. Beyond 6 months of age, AD symptoms were only managed using the medical treatment approach.
Medical treatment approach
Upon entering this arm, subjects were prescribed medications and referred to a specialist according to the severity of their AD. According to expert opinion, all mild cases were to be treated by emollients only and, in case of no response after 2 weeks, by Class II topical corticosteroids for another 2 weeks. Fifty per cent (50%) of moderate cases were to be treated with Class II topical corticosteroids for a period of 2 weeks after which treatment was halted in the case of response or upgraded to topical immunosuppressants (tacrolimus or pimecrolimus) for a further 2 weeks in case of non-response. In the remaining 50% of moderate cases and 100% of severe cases, subjects were to be treated for a period of 1 month with Class II or III topical corticosteroids followed by a pro-active management regimen lasting 5 months and consisting of tapering down the use of topical corticosteroids and replacing them by pimecrolimus or tacrolimus.
Combined management approach
In the combined approach to the management of AD symptoms, subjects were also assigned a new infant formula (EHF-Whey) while being prescribed medications in accordance to the medical treatment approach above. In case of response, subjects continued consuming the new milk formula until 6 months of age. For subjects who did not respond, AAF was assigned.
Epidemiological and clinical parameters applied in the model
The initial cohort entering the model represented the target population of this study: the ‘at risk’ population of newborn subjects who were not exclusively breastfed in Switzerland. The number of infants born in Switzerland in 2009 was obtained from the Office Fédéral de la Statistique (OFS)Citation25. The Swiss Federal Office of Public Health reported the rates of exclusive breastfeeding for the first 6 months of age for the year 2003Citation2Citation6. Three studies provided an approximation of the rate of newborns who were ‘at risk’ of developing ADCitation4–6. Thus, the initial cohort was defined by the following mathematical formula:
(Birth cohort in Switzerland)×(1− Average Exclusive Breastfeeding rate)×(Rate of ‘at risk’ infants)
Two main factors, namely, the age of the subject (which was inherent to the model) as well as the severity (mild, moderate, or severe) of the AD manifestation, were used to characterize the cases of AD occurring in the model. These rates were obtained from expert opinion. The medical treatment approach and the combined management approach were divided into first- to second-line treatments; expert opinion provided the expected average response rates (defined as an improvement of AD symptoms) for each line of treatment.
Although AD does not affect mortality, general mortality rates were applied in the dynamic model according to published sourcesCitation27.
Resource utilization and costs
In the base case analysis, it was assumed that infant formulas used for prevention were covered at 90% by the MOH as is currently the case in Switzerland with EHF-Whey for treatment. This scenario where the cost of PHF-W and SF is reimbursed by the MOH (although no milk formula is currently reimbursed for prevention, and SF is neither intended to replace breastfeeding nor would it be appropriate for prevention of AD), made it possible to carry out a direct comparison of the most commonly used infant formula, SF, with the only 100% whey-based partially hydrolyzed formula that has been proven effective in prevention of AD symptoms, PHF-W.
A set of SAs explored scenarios in which all infant formulas were covered by the MOH at various rates or in which PHF-W was included in a setting where no other formula was reimbursed for prevention.
Although EHF-Whey is indicated for the treatment of AD symptoms, not their prevention, some physicians may choose to recommend EHF-Whey as a preventive measure. This possibility was explored in a SA which is described in the upcoming section ‘Comparisons with EHF-Whey’.
In the model, it was assumed that infant formulas were consumed for the first 6 months of life. In the Szajewska and HorvathCitation16 meta-analysis, a wide variety of SF brands, two specific brands of EHF-Whey (Profylac®, ALK, Hørsholm, Denmark and Cow and Gate Pepti Junior®, Trowbridge, UK) and one brand of EHF-Casein (Nutramigen®, Mead Johnson, Illinois, USA) were included as comparators to PHF-W. Thus, for the present analysis, with the absence of a specific brand as a comparator, the cost of SF was based on the brand with the highest market share in Switzerland, namely Aptamil-1® (Danone, St-Ouen, France). Given that the two brands which had been used by Szajewska and HorvathCitation16 as EHF-Whey comparators are not readily available in Switzerland, the cost of EHF-Whey was based on the average cost of two common preparations: Althera® and Alfaré® (Nestlé, Vevey, Switzerland). The cost of the AAF was derived from Neocate (Nutricia, Schiphol, The Netherlands). The price of each infant formula was obtained from a survey of pharmacies. It was assumed that SF, PHF-W, and EHF-Whey were covered at a rate of 90%, whereas AAF was fully paid by the family, as is currently the case in Switzerland. The mean daily quantity of infant formula consumed in the dynamic model was determined according to an increasing scheme ranging from 84.6–141 g over 6 months, based on the instructions for the preparation of PHF-W, according to the proportions of infants who were either fully or partially breastfed.
According to expert opinion, all first-line medical visits are with a general pediatrician. Subsequently, 10% of subjects with mild AD and all subjects with moderate or severe AD are immediately referred to a specialist (either a dermatologist or an allergist) for one visit in the case of mild AD and two additional visits for moderate or severe cases. In addition to medical visits, the clinical expert indicated that 1.5% of moderate or severe cases would be hospitalized for an average of 5 days. The estimated cost of these interventions was obtained from expert opinion.
According to the expert panel, all subjects would have initiated the use of emollient creams for a period of 2–3 months for mild cases and a period of 6 months for moderate and severe cases, twice daily, at a rate of 250 g of emollient cream per 3-month period. Applied in the model was the only brand of emollient which is always reimbursed (at a rate of 90%) by the MOH.
Also, according to expert opinion, treatment of AD symptoms may consist of only emollients, Class II or III topical corticosteroids, and/or immunosuppressants (tacrolimus or pimecrolimus), depending on the age of the subject, the severity of AD symptoms, and the success of each line of treatment. The cost of medications and emollients was obtained from the Compendium Suisse des MédicamentsCitation28.
According to expert opinion, 40% of subjects with moderate or severe AD would be administered the Specific IgE Test and the Prick Test, while 5% of subjects with severe AD would also be administered the Oral Provocation Test. The costs of these laboratory tests were obtained from a survey of a medical laboratory in Canton Fribourg.
When analysing the family and societal perspectives, indirect costs due to leisure time and/or productivity loss were included in the model. These indirect costs were determined by taking into account the population rate of participation in the workforce in Switzerland (published by the OFS for 2009)Citation29 as well as the average gross hourly wage and weekly hours of work for each economic activity in Switzerland published for 2008 by the International Labour OrganizationCitation30,Citation31.
The cost of travel to and from the physician’s office, for an assumed distance of 10 km, was established by using an average of the cost of public transportation (bus and metro), the cost of using a taxi, and the cost of operating a personal car in GenevaCitation32,Citation33. The cost of operating a personal car was approximated by using the per kilometer rate for a taxi (i.e., excluding service charges and the additional fare for waiting in traffic).
Discounting
All costs beyond 1 year were discounted, but outcomes were analyzed with or without discounting given that the discounting of outcomes is still controversialCitation34. Discount rates of 2.5, 5, and 10% were applied as per the draft guidelines of the Swiss Federal Social Insurance OfficeCitation35.
Comparisons to EHF-Whey
A secondary analysis was undertaken to explore a scenario wherein EHF-Whey was assumed to be used in prevention. The Szajewska and HorvathCitation16 meta-analysis had reported no significant difference between the RR of PHF-W vs EHF-Whey, which implied the same efficacy to be applicable to both formula preparations. Accordingly, this secondary analysis consisted of a cost-minimization exercise based on the difference in the acquisition cost of the formula itself. The same combined management pattern was applied to subjects consuming PHF-W, whereas subjects consuming a preparation of EHF-Whey were assumed to be switched to AAF immediately.
Variability and uncertainty
To address previously discussed as well as other uncertainties in the model, the effect of various parameters on the outcomes of the economic model was determined by carrying out a series of one-way SAs. One additional set of SAs explored the impact of introducing PHF-W as a new program wherein PHF-W would be the first infant formula to be covered by the MOH. Sensitivity analyses were completed wherein the MOH paid for 100%, 60%, 35%, and 15% of PHF-W costs, while an additional SA was carried out with the MOH only paying the difference between PHF-W and SF costs.
Furthermore, probabilistic SAs were carried out by simultaneously varying multiple parameter values. As such, a set of 10,000 Monte Carlo simulations was carried out using Oracle Crystal Ball® 11.1.2 to test the robustness of the economic model by simultaneously varying key parameter values according to pre-set ranges and types of distribution.
Results
Base-case analysis
For a birth cohort of 80,000 newborns in Switzerland in 2009, the starting cohort entering the model had 22,933 ‘at risk’ newborns, assumed to be taking either PHF-W or SF. The epidemiological and clinical parameters that were assigned to the model and the list of economic inputs are presented in Tables and .
Table 1. Epidemiological and clinical parameters applied in the model.
Table 2. Economic parameters applied in the model.
presents the results of the base case analysis from three different perspectives (MOH, family, and society) when comparing subjects who consumed PHF-W to those who consumed SF. The expected numbers of cases attributed to PHF-W and SF were 2287 and 3940, respectively, yielding a total of 1653 avoided cases of AD by selecting PHF-W over SF.
Table 3. Base case results presented from the perspective of the Ministry of Health, of the family of the subject and of society as a whole.
The total direct and indirect costs associated with PHF-W and SF were CHF 21,620,537 and CHF 23,636,558, respectively, yielding savings with PHF-W. From the MOH and societal perspectives, the highest cost was attributable to formula while the cost of time lost was the main cost driver from the perspective of the subject’s family. The expected incremental costs per avoided case of AD (i.e., the expected ICERs) were CHF 982, −CHF 2202 (savings) and −CHF 1220 (savings) from the MOH, family, and societal perspectives, respectively.
PHF-W vs EHF analysis
PHF-W was dominant over EHF-Whey in the scenario where the latter was used in the prevention of AD symptoms given the assumption that both formulas are equally effective in the prevention of ADCitation16,Citation24. The savings for the cohort with the use of PHF-W over EHF-Whey amounted to ∼CHF 11.4 million, including savings of CHF 10.2 million from the MOH perspective.
One-way sensitivity analyses
presents the results of most of the one-way SAs which were undertaken to evaluate the effect of key parameters on the outcomes of the economic model. The greatest variation from the base case ICERs of the MOH and societal perspectives was observed when applying the upper bound of the 95% CI of the RR of developing AD. In that SA, the advantage of PHF-W over SF in prevention was greatly diminished. From the perspective of the family of the subject, the greatest variation from the base case ICER was noted in the SA, wherein the MOH did not cover the cost of infant formulas, thus shifting this cost driver over to the family.
Table 4. Results of the one-way sensitivity analyses presented from the perspective of the Ministry of Health, of the family of the subject and of society as a whole.
In the one-way SA where PHF-W was introduced into a new program where there was no formula previously covered for prevention of AD under the MOH (i.e., SF was not covered), an ICER of −CHF 1220 was again obtained when viewed from the perspective of society as a whole. However, from the MOH perspective, the ICERs were higher than the base case when the MOH paid 90%, 60%, 35%, and 15% of PHF-W costs (CHF 8541, CHF 5639, CHF 3220, and CHF 1286, respectively), but similar to the base case when the MOH covered the difference of PHF-W and SF costs (CHF 1061). A cost-neutral ICER was observed when the MOH paid for 1.71% of PHF-W costs.
Probabilistic sensitivity analyses
The parameters which were varied in the probabilistic SAs, their distributions, and their ranges are presented in . Also presented in and are the results of these probabilistic SAs from all three perspectives (MOH, the subject’s family, and society). The average Monte Carlo ICER from the MOH perspectives was CHF 675, with a 99% probability of cost-effectiveness of PHF-W vs SF. From the perspectives of the family and society, the average Monte Carlo ICERs displayed savings (and probabilities of showing cost-effectiveness or dominance) of CHF 994 (20.5%, 79.3%) and CHF 319 (44.6%, 55.2%), respectively.
Figure 2. Results of the Monte Carlo simulations from the Ministry of Health, family, and societal perspectives. These findings are presented for a population of 80,000 newborns (as in Switzerland in 2009), of which 22,903 were deemed to be ‘at risk’ and not exclusively breastfed. The presented incremental cost-effectiveness ratios were obtained by dividing the average incremental costs by the average avoided cases of AD which were generated from the 10,000 Monte Carlo simulations. The base case incremental cost-effectiveness ratios were CHF 982, −CHF 2,202, and −CHF 1,220 from the MOH, family, and societal perspectives, respectively. MOH, Ministry of Health.
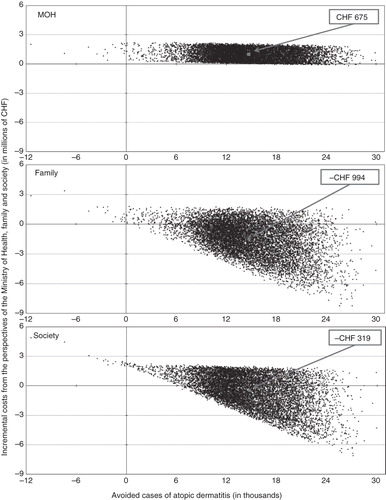
Table 5. Parameter estimates and distributions for variables tested in the Monte Carlo sensitivity analysis.
Median ICERs of CHF 672, −CHF 928, and −CHF 183 were observed from the MOH, family, and societal perspectives, respectively, with a 72%, 12%, and 19% probability for Monte Carlo results to fall below a line linking the base case ICERs to the origin.
Discussion
To our knowledge, this is one of the first studies based on a Swiss setting pertaining to the cost-effectiveness of PHF-W in the prevention of AD in ‘at risk’ children. This study falls in line with a previous study that was undertaken for FranceCitation23.
The obtained incremental cost per avoided case of AD was very attractive at CHF 982 from the MOH perspective, while PHF-W demonstrated dominance over SF from the family and societal perspectives.
The robustness of the model was confirmed by both the one-way SAs and Monte Carlo simulations, as most yielded ICERs were similar to or in line with those obtained in the base case. There was, however, one exception, namely the one-way SA wherein the upper bound of the 95% confidence interval of the RR of developing AD symptoms when using PHF-W vs SF, i.e., the case where the efficacy was minimized. In that scenario, SF was dominant over PHF-W as it had been granted greater efficacy than PHF-W in preventing AD symptoms, a situation that two meta-analyses have deemed improbableCitation16,Citation17. This was confirmed by the probabilistic SA in which dominance of SF over PHF-W was only observed in only 0.18% of Monte Carlo simulations while the opposite, i.e., dominance of PHF-W over SF, resulted in 55.2% of cases. Incremental cost-effectiveness of PHF-W vs SF was observed in ∼44.6% of cases. The probabilistic SA seems more conservative, yet possibly more plausible, than the base case analysis because of the range of parameter values applied. This range tended to push the model towards being more conservative by presenting higher probabilities of the simulations, randomly selecting values lower than those of the base case. Accordingly, an average ICER of CHF 675 from the MOH appears very attractive for reimbursement. The observed incremental ratios were similar to those observed in a similar cost-effectiveness analysis which was undertaken in a French setting (where the base case expected ICERs were €1343, −€624 and €729, from the MOH, family, and societal perspectives, respectively)Citation23, and comparable to previously published European estimates of the burden of ADCitation20–23.
The main cost driver from the MOH and societal perspectives was the cost of infant formula. From the perspective of the family, the main cost driver was the cost of time lost, defined as costs incurred due to either productivity or leisure time loss due to child care, based on whether the family members participate in the workforce in Switzerland or not. All productivity costs were attributed to the family even though some families would have access to paid ‘sick days’ or ‘family days’ through their employers, and would not technically have to suffer a loss of revenue because of time spent on child care. This approach was adopted as not all parents have access to these social benefits (these services might not be offered by the employer, or the parents may be self-employed), and parents who take paid time off for child care might have to make up their lost productivity time by staying longer at work upon their return, which would simply transfer past productivity loss to future productivity or leisure time loss. Alternatively, the cost associated with these ‘sick days’ or ‘family days’ could be applied to a third party, the employers, which would increase the expected ICERs from the family perspective but would not affect the expected ICERs from the societal perspective as overall costs would remain the same (as demonstrated in the SA where the cost of leisure time was excluded while the cost of productivity time lost was shifted to the employers, i.e., society). Hence, in the interest of an effective and streamlined base case analysis, it was assumed that all costs of productivity and leisure time loss would be attributable to the family of the subject.
In order to be conservative, this study did not take into account broader allergic manifestations such as atopic rhinitis or asthma due to the lack of clearly demonstrable evidence linking these disorders to the population of interest. Furthermore, intangible outcomes such as pain or suffering were not monetized in this cost-effectiveness analysis. A literature search yielded two studies reporting utility scores for ADCitation37,Citation38. However, upon reviewing those studies, the published utility scores could not be deemed reliable or adaptable enough to serve in a cost-utility approach for a study in infants. In any case, the results of this cost-effectiveness analysis suggest the PHF-W would be an appropriate candidate for adoption by public programs when prescribed in the prevention of ‘at risk’ infants who have not been exclusively breastfed.
A further analysis comparing PHF-W and EHF-Whey in the prevention of AD symptoms yielded a cost saving of ∼CHF 11.4 million which entails for the cohort ∼CHF 2.7 per child per day of milk consumption. That amount takes into account the increased costs of the replacement formula, i.e., EHF-Whey for PHF-W and AAF for EHF-Whey, for ∼3% of the cohort who present AD symptoms. This suggests that EHF-Whey may be appropriate for use as treatment but not in prevention, particularly when one takes into account issues such as non-compliance due to taste or texture.
Limitations
As in all predictive modelling exercises, the current model may contain a certain amount of bias. Nevertheless, whenever possible, the base case analysis was undertaken by selecting the more conservative approach that applied the bias against the product of interest (PHF-W). Moreover, numerous SAs (both one-way and probabilistic in nature) which were performed in order to observe the effect of particular parameters on the overall output of the model confirmed its robustness.
The first limitation of the model was the fact that it was limited to infants who were at risk of developing AD symptoms. This limitation, however, did not present a bias in favor of PHF-W as it downplayed its preventive nature by minimizing the starting cohort of the model. A broader rate of infants ‘at risk’ of developing AD for other reasons than heredity could not be found in the available literature.
In the Szajewska and HorvathCitation16 meta-analysis, some of the included studies limited their scope to exclusively formula-fed infants while other studies included infants who were not exclusively formula-fed. Nonetheless, these latter studies did not report a difference in the breastfeeding rates between PHF-W and comparator arms. Hence, in the present study, it was assumed that breastfeeding did not impact on the clinical efficacy of infant formulas that were consumed at the same time.
The Szajewska and HorvathCitation16 meta-analysis from which the clinical efficacy rates were derived might have contributed a certain bias as it included a wide variety of randomized controlled trials with differing sizes and variability in samples. Yet, the very fact that these studies were synthesized using a meta-analytic approach should limit the bias inherent in those data and make them more attractive when compared to the results of a single clinical trial.
Incidence rates of AD are believed to be higher earlier in life. Thus, a bias might have been introduced against PHF-W by assuming equal incidence rates for adjoined 3-month intervals between the periods of 0–6 months and 6–12 months because this would defer some of the incidence to a later point in life which would in turn limit the preventive impact of PHF-W in the first months. Furthermore, a similar bias against PHF-W may have been introduced to the model due to the fact that events were accounted for at the mid-point of each 3-month interval, for ease of mathematical modelling.
In the base case analysis, from the MOH perspective, the main cost driver was the cost of formula, implying that any limitation associated with the computation of infant formula in the model needed to be tested. One such limitation is the fact that the daily quantity of formula consumed by the subjects in the model was assumed to be equal throughout for all formulas, although it may not be the case in practice. Moreover, following a discontinuation, subjects were assumed to change to a different brand of the same formula preparation type of equal price to that of the initial brand. One-way SAs, which were undertaken on the utilization and costs of milk formula, generated ICERs comparable to those found in the base case analysis, again confirming the robustness of the model.
Another bias against PHF-W may have been introduced by assuming that the occurrence of flare-ups coincided with the time of treatment, thus not requiring additional resource utilization or costs. In a real-life setting, flare-ups are believed to happen at any time, within the period of treatment or afterwards.
Finally, the boundaries of the values assigned to the parameters of the Monte Carlo simulations rendered the multivariate analysis even more conservative than the base case analysis, especially that the nature of the uniform distribution signified that the values selected for the Monte Carlo simulations were skewed, resulting in a more conservative approach than the base case.
Finally, the findings of the present analysis are specific to the brand of partially hydrolyzed formula being the focus of the present study, as well to practices and settings within the Swiss healthcare system. Accordingly, caution should be taken before any attempts for generalizability and transferability of results.
Conclusions
Under a certain range of assumptions, this analysis based on predictive modelling has established the cost-effectiveness of BEBA HA®, a specific brand of 100% whey-based partially hydrolyzed formula in the prevention of atopic dermatitis in infants and very young children in Switzerland. PHF-W demonstrated dominance over SF from the family and societal perspectives and attractive cost-effectiveness at CHF 982 from the MOH perspective. PHF-W was also dominant over EHF-Whey from the MOH perspective.
Transparency
Declaration of funding
This study was funded by the Nestlé Nutrition Institute (NNI, Vevey, Switzerland) and conducted at arm’s length by PharmIdeas.
Declaration of financial/other relationships
Dr Patrick Detzel is employed by NNI; Michael Iskedjian, Bechara Farah and Vincent Navarro are employed by PharmIdeas; Dr Dominique Belli received honoraria for his services.
Acknowledgments
We would also like to acknowledge Jade Berbari (of PharmIdeas) for his analytical and editorial input.
References
- Spergel J, Paller A. Atopic dermatitis and the atopic march. J Allergy Clin Immunol 2003;112:S118–27
- Asher M, Montefort S, Björkstén B, et al. Worldwide time trends in the prevalence of symptoms of asthma, allergic rhinoconjunctivitis, and eczema in childhood: ISAAC phases one and three repeat multicountry cross-sectional surveys. Lancet 2006;368:733–43
- Schulz Larsen F, Hanifin J. Epidemiology of atopic dermatitis. Immunol Allergy Clin North Am 2002;22:1–24
- Bergmann R, Edenharter G, Bergmann K, et al. Atopic dermatitis in early infancy predicts allergic airway disease at 5 years. Clin Exp Allergy 1998;28:965–70
- Halken S. Allergy Review Series VI: the immunology of fetuses and infants. The lessons of noninterventional and interventional prospective studies on the development of atopic disease during childhood. Allergy 2000;55:793–802
- Exl B-M. A review of recent developments in the use of moderately hydrolyzed whey formulae in infant nutrition. Nutr Res 2001;21:355–79
- von Berg A, Koletzko S, Filipiak-Pittroff B, et al. The effect of hydrolyzed cow's milk formula for allergy prevention in the first year of life: The German Infant Nutritional Intervention Study, a randomized double-blind trial. J Allergy Clin Immunol 2003;111:533–40
- Baehler P, Baenziger O, Belli D, et al. Empfehlungen für die Säuglingsernährung 2009. Paediatrica 2009;20:13–5
- Lasarte Velillas J. Recomendaciones para la lactancia materna. Comité de Lactancia Materna de la Asociación Española de Pediatría. 2011;1–6 http://www.aeped.es/sites/default/files/lacmat-espanol.pdf [Last Accessed: December 23, 2011]
- Muche-Borowski C, Kopp M, Reese I, et al. Allergieprävention. AWMF Guideline Register 061/16, 2009
- Société Française de Dermatologie. Prise en charge de la dermatite atopique de l'enfant. Texte des recommandations. Ann Dermatol Vénéréol 2005;132:1S9–1S18
- World Health Organization and United Nations Children's Fund. Global strategy for infant and young child feeding. Geneva: NLM Classification: WS 120, 2003
- World Health Organization. World Health Organization's recommendations on breasfeeding. Available at: http://www.who.int/topics/breastfeeding/en. Accessed February 9, 2010
- von Berg A, Filipiak-Pittroff B, Krämer U, et al. Preventative effect of hydrolyzed formulas persists until age 6 years: long-term results from the German Infant Nutritional Intervention Study (GINI). J Allergy Clin Immunol 2008;121:1442–7
- von Berg A, Koletzko S, Filipiak-Pittroff B, et al. Certian hydrolyzed formulas reduce the incidence of atopic dermatitis but not that of asthma: three-year results of the German Infant Nutritional Intervention Study. J Allergy Clin Immunol 2007;119:718–25
- Szajewska H, Horvath A. Meta-analysis of the evidence for a partially hydrolyzed 100% whey formula for the prevention of allergic diseases. Curr Med Res Opin 2010;26:423–37
- Alexander D, Cabana M. Partially hydrolyzed 100% whey protein infant formula and reduced risk of atopic dermatitis: a meta-analysis. J Pediatr Gastroenterol Nutr 2010;50:422–30
- Lewis-Jones S. Quality of life and childhood atopic dermatitis: the misery of living with childhood eczema. Int J Clin Pract 2006;60:984–92
- Kemp A. Cost of illness of atopic dermatitis in children. A societal perspective. PharmacoEconomics 2003;21:105–13
- Ricci G, Bendandi B, Pagliara L, et al. Atopic dermatitis in Italian children: evaluation of its economic impact. JPediatr Health Care 2006;20:312–5
- Gieler U, Hohmann M, Niemeier V, et al. Cost evaluation in atopic eczema. J Dermatol Treat 1999;10:S15–S20
- Weinmann S, Kamtsiuris P, Wickman H, et al. The costs of atopy and asthma in children: assessment of direct costs and their determinants in a birth cohort. Pediatr Allergy Immunol 2003;14:18–26
- Iskedjian M, Dupont C, Kanny G, et al. Economic evaluation of a 100% whey-based, partially hydrolyzed formula in the prevention of atopic dermatitis among French children. Curr Med Res Opin 2010;26:2607–26
- Iskedjian M, Szajewska H, Spieldenner J, et al. Extension of a meta-analysis of the evidence for a partially hydrolyzed 100%-whey formula in the prevention of atopic dermatitis: brief research report. Curr Med Res Opin 2010;26:2599–606
- Office Fédéral des Statistiques. La population de la Suisse 2009. Neuchâtel: Office Fédéral des Statistiques, Report Number: 349-0900, 2010
- Merten S, Dratva J, Ackermann-Liebrich U. Swiss Federal Office of Public Health. Infant feeding during the first 9 months - Swiss National Study 2003. Berne: 2005
- Swiss Life Tables 1998/2003. Office fédéral de la statistique. Available at: http://www.bfs.admin.ch/bfsportal/en/index/themen/01/02/blank/dos/la_mortalite_en_suisse/tabl01.html. Accessed March 1, 2011
- Compendium Suisse des Médicaments. Document. Documed. Available at: http://www.documed.ch/fr/index.php. Accessed March 1, 2011
- Office fédéral de la statistique. Gross activity rate (total population) in 2009. Available at: http://www.bfs.admin.ch/bfs/portal/en/index/themen/03/02/blank/key/erwerbsquote.html Accessed March 1, 2011
- International Labour Organization. Hours of work per week by economic activity in Switzerland in 2008 (Table 4A). Available at: http://laborsta.ilo.org. Accessed March 29, 2011
- International Labour Organization. Wages by economic activity in Germany in 2008 (Table 5A). Available at: http://laborsta.ilo.org. Accessed March 29, 2011
- TPG (Transports Publics Genèvois). Cost of public transportation in Geneva. Available at: http://www.tpg.ch/fr/titres-de-transport/index.php. Accessed March 1, 2011
- Genève Tourisme. Cost of taxi in Geneva.Available at: http://www.geneve-tourisme.ch/?rubrique=0000000415. Accessed March 1, 2011
- Drummond M, Sculpher M, Torrance G, et al. Methods for the economic evaluation of health care programmes. 3rd edn. Oxford, UK: Oxford University Press, 2006
- Swiss Federal Social Insurance Office. Manual for the standardization of clinical and economic evaluation of medical technology (1998 draft). Available at: http://www.ispor.org/PEguidelines/countrydet.asp?c=25&t=1. Accessed May 3, 2011
- Briggs A, Claxton K, Sculpher M. Decision modelling for health economic evaluation. Oxford, UK: Oxford University Press, 2008
- Pitt M, Garside R, Stein K. A cost-utility analysis of pimecrolimus vs. topical corticosteroids and emollients for the treatment of mild and moderate atopic eczema. Br J Dermatol 2006;154:1137–46
- Coyle D, Barbeau M. Cost effectiveness of elidel in the management of patients with atopic dermatitis in Canada. J Cutan Med Surg 2004;8:405–10