
Abstract
Objectives:
To compare ASAS (Assessment in Ankylosing Spondylitis Response Criteria), 20 response patterns between anti-TNF biological agents in patients with ankylosing spondylitis by means of a mixed treatment comparison of different randomized, controlled trials (RCTs) on the efficacy of biological therapies.
Methods:
A systematic review of literature was performed to identify a number of similarly designed double-blind, randomized, placebo-controlled trials investigating the efficacy of the TNF-α inhibitors etanercept, infliximab, and adalimumab in the treatment of ankylosing spondylitis patients, conducted over an 18-year period. The end-point of interest was ASAS20 response criteria at 24 weeks. Results were analyzed simultaneously using Bayesian mixed treatment comparison techniques. Results were expressed as odds ratio (OR) of ASAS20 response and associated 95% credible intervals (CrIs). The probability of being the best treatment was also reported.
Results:
Three RCTs were selected for data extraction and further analysis. By mean of MTC, all anti-TNF agents demonstrated to be more efficacious in inducing an ASAS20 response than placebo. Infliximab shows a 72% probability of being the best treatment of all. Adalimumab and etanercept show probabilities of 13% and 15%, respectively. No differences were observed when comparing directly an anti-TNF-α agent against another. When compared with placebo, Infliximab increases the probability of response by ∼7-times (OR = 6.8), Adalimumab by ∼4-times (OR = 4.4), and Etanercept by 5-times (OR = 4.9). Differences in trials procedures, the use of a fixed-effect model, and the small number of trials included represent limitations of this study
Conclusions:
Even if the mixed treatment comparisons between infliximab, adalimumab, and etanercept did not show a statistically significant difference, this analysis suggests that infliximab, compared to placebo, is expected to provide the highest rate of ASAS20 response in SA patients naive to biologic treatments.
Introduction
Ankylosing Spondylitis (AS) is a chronic form of arthritis belonging to the broader category of spondyloarthropathies, or arthritis that primarily affects the spine. AS is an inflammatory disease of unknown origin that mainly involves the spinal joints and frequently progresses into ankylosis of the affected jointsCitation1. Up to half of patients have concomitant peripheral joint arthritisCitation2. Recent experiences strongly suggest a familial aggregation for AS. Individuals presenting the genetic marker HLA-B27 have at least a 1% chance of developing AS. However, the actual relationship between the gene and the disease’s development is still not completely clearCitation1–3.
Unlike other, more common inflammatory joint disorders, such as rheumatoid arthritis and psoriatic arthritis, where some patients achieve control of disease activity using non-biological DMARDs, the use of biological treatments is often required to treat AS patients in order to control disease activityCitation4–11. Although good efficacy and safety profiles have been extensively proven for all anti-TNF therapies in patients with AS, a more precise understanding of the therapeutic role of each anti-TNF agent used to treat AS is required to allow a more accurate choice of treatment options for these patientsCitation12,Citation13. Patients presenting an inadequate response to previous non-biological therapies are treated with the biological agents or tumor necrosis factor (TNF) blockers etanercept, infliximab, and adalimumab. Etanercept is a dimeric fusion protein consisting of the extracellular ligand-binding portion of the human 75 kilodalton (p75) tumor necrosis factor receptor (TNFR) linked to the Fc portion of human IgGCitation9. Infliximab is a chimeric monoclonal antibody IgG1κ with an approximate molecular weight of 149.100 daltons. It is composed of human constant and murine variable regionsCitation10. Adalimumab is a recombinant fully human IgG1 monoclonal antibody specific to human tumor necrosis factor (TNF). Adalimumab was created using phage display technology resulting in an antibody with human-derived heavy and light chain variable regions and human IgG1 κ constant regionsCitation11. Such drugs present biological and clinical differences that may result in different efficacy outcomes in different pathologies where they are commonly usedCitation9–11. For such a reason, also, this study was performed.
In order to allow a more accurate choice of treatment, it is also necessary to compare the efficacy of all therapies available, a comparison that has so far not been performed. To date, there are no published RCTs providing data on a head-to-head comparison of the efficacy of etanercept, infliximab, and adalimumab in the treatment of AS. This kind of RCT would require very large patient caseloads, as the differences in terms of efficacy between the biological treatments would appear to be small, and consequently the cost of conducting this sort of trial would be very high. Mixed Treatment Comparison (MTC), an extension of more conventional and commonly used meta-analysis, allows us to make multiple pair-wise comparisons across a range of different treatmentsCitation14–18. The results obtained using this statistical analysis technique provide an objective approach to the difficult choice of treatment, when similarly relevant data are unavailable. More specifically, using MTC we aimed to compare the results in terms of efficacy obtained in different RCTs performed on each anti-TNF therapy in patients with AS. Compared to common meta-analysis, where multiple studies are used to estimate the efficacy of a single agent vs placebo or other reference treatments, Mixed Treatment Comparison enables the estimation of different parameters from different studies with similar comparisons, and makes it possible to obtain further data by assembling and analyzing data of several similar studies on the same subjectCitation14–18. The main objective of this study was to determine parameters that may prove useful in clinical practice and in real-world medical decisions. For this reason, we concentrated our efforts on determining relative efficacy profiles of currently licensed doses of commonly used biological treatments for AS.
Methods
Identification of eligible studies and data extraction
A literature search was performed to identify all RCTs performed to assess the efficacy of different anti-TNF treatments (etanercept, infliximab, adalimumab) in patients with AS. The MEDLINE and EMBASE databases were both intensively searched, and search terms included a combination of free-text and thesaurus terms relevant to AS agents. The search terms are reported in . The primary end-point for analysis was the ASAS20 response criteria from baseline to month 6Citation19. Studies with shorter follow-up periods were excluded from the study. The ASAS criteria for 20% clinical improvement (ASAS20) is met when an improvement of at least 20% and one unit is obtained in at least three of the following four domains: patient’s global assessment of disease activity, inflammation assessed as morning stiffness, function and pain, without worsening of 20% and one unit in the remaining domains.
Table 1. Research terms and proceeding used in EMBASE and MEDLINE for literature search.
Only RCTs reporting data on placebo-controlled, double-blind studies with a follow-up of at least 24 weeks on the efficacy, expressed as ASAS20, of an anti-TNF agent in patients affected by AS were included. For each selected study, details regarding study design, patients’ demographic and morbidity characteristics, treatment interventions, end-points and duration of follow-up were analyzed. Unless otherwise stated, imputation for non-response was assumed to be through last observation carried forward.
Data analysis
An evaluation of the primary trial end-point, ASAS20, was conducted to identify any differences, in terms of efficacy, between the three anti-TNF agents analyzed. A large number of tools are currently available to assess the current status of a patient affected by AS in all different aspects of disease, such as limitation of motion of the spine or pain, but standardization and validation of many of these tools is still lacking, while for ASAS, born from an international Assessment in AS, the standardization is clearly assessed. The choice of ASAS20 as the primary end-point is due to the fact that all the reported pivotal trials reported ASAS20 as the primary end-point.
For subsequent analysis, we used the reported number of patients in each response category in the treatment and placebo groups of each RCT eligible for analysis. These frequencies were processed by a Bayesian MTC analysis, fixed effect model. It is also fundamental to determine whether a fixed-effect model or a random-effect model is more appropriate for pooling results from different studiesCitation14. The residual deviance of models obtained using random effects and fixed effects was compared: when the residual deviance obtained by a random-effect model is lower than fixed model residual deviance, a random-effect model may be more appropriate, however, when residual deviance is similar, a fixed-effect model seemed to be the most suitable option. WinBUGS 1.4 statistical software (MRC Biostatistics Unit, Cambridge, UK) was used to perform analysis. WinBUGS provides Bayesian estimates, and the analysis was conducted without prior assumptions concerning coefficient sizes. This study reports results as summary statistics for Odds Ratio (OR): the mean value that is the most likely value and the correspondent 95% credible interval (95% CrIs) that contains the true value of the OR with 95% probability. MTC reports results as an evaluation of OR of response as ASAS20 for each biological agent compared to placebo and also the OR of response, again in terms of ASAS20, between each combination of two biological agents. The probability of best treatment was also reported for each biological agent.
Results
Identified studies
A total of 1022 articles were extracted from EMBASE and MEDLINE using the research terms reported in (Adalimumab or Etanercept or Infliximab and Ankylosing Spondylitis). Of the selected articles only 69 remained after the research term ‘double-blind’ was added. Of the 22 articles selected, only 10 remained after a term search on ‘ASAS’ was included. In any case, only three articles met the inclusion criteria established previously and were consequently included in the study for data extractionCitation20–22. The selected articles are shown in . Length of study, number of patients included, demographic characteristics, different disease duration and eventual concomitant medication, severity of disease, and outcome measures were considered. Consequently, all data were recorded and analyzed using a MTC with the analytic methodologies described above. The studies identified differ as regards some features and were intensively analyzed for their differences in order to understand whether these differences could invalidate the results of the MTC. One study reported data from an RCT on etanercept, one study on adalimumab, and one study on infliximab. The populations of the different studies were similarly represented, in terms of gender and disease duration. The BASDAI score, which is reported for all studies, is similar in all studies, and a statistical examination of any considerable differences did not show any significance. Data such as ESR, CRP, and presence of HLA-B27 gene polymorphism are not reported in all studies.
Table 2. Selected articles and data which were considered for further analysis. Length of study, number of patients included, demographic characteristics, different disease duration and eventual co-medications, severity of disease, and outcome measures were considered.
Populations object of the study
All populations from the three RCTs were examined for 24 weeks. Genders were equally represented in all populations and mean age was similar, mean BASDAI scores were similar as well as percentage of patients characterized by positive HLA-B27. The only difference observed regarded duration of disease in the active arm of Infliximab-based RCT, that was 7.7 years, with respect to all other populations studied whose disease duration was at least 10 years. This difference does not represent in our opinion a statistically relevant problem as the BASDAI score of the same population was similar to the ones reported for other populations.
ASAS20 responses
All anti-TNF agents proved to be more efficacious in inducing an ASAS20 response than placebo. Data concerning the OR of response in terms of ASAS20, in patients with AS and naïve for biological treatment, for the different anti-TNF agents included in the study compared to placebo are reported in . Infliximab was the anti-TNF agent that gives the highest OR of response when compared to placebo (OR = 6.88; 95% CI =3.66–13.46). Adalimumab, when compared to placebo, gives an OR of response of 4.48 (95% CI = 2.63–9.16), whereas etanercept, when compared to placebo, gives an OR of 4.95 (95% CI = 2.71–8.16). Further analysis, performed in order to make direct comparisons between the three anti-TNF agents included in the study, showed no significant differences between them.
Figure 1. Graphical expression of MTC between Adalimumab, Etanercept and Infliximab against placebo and comparison of the three drugs between each other.
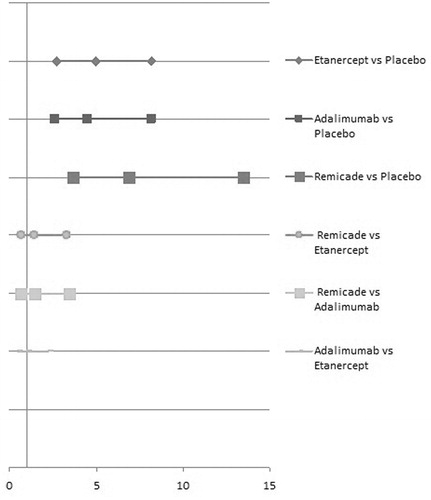
Infliximab showed a 72% probability of being the best treatment of all. Adalimumab and etanercept show probabilities of 13% and 15%, respectively (see ).
Table 3. Fixed effects MTC showing Odds Ratio and Credible Intervals for comparison between Adalimumab, Etanercept, and Infliximab, and probability of being best treatment for each drug.
Discussion
To date, this is the first study that uses MTC to compare the three anti-TNFα drugs currently used in the treatment of patients affected by AS. Since there are no head-to-head studies comparing these three agents in the treatment of AS, MTC could play an important role in obtaining new comparative evidence. Indeed, MTC allows the simultaneous multiple meta-analysis of different pair-wise comparisons across a range of different interventions. Literature reports an increasing use of the mixed treatment comparison approach in several diseases, and it has been used to analyze stroke prevention, anti-depressants, psychological interventions in heart disease, and the prevention of vertebral fractures in women with post-menopausal osteoporosisCitation23–26.
The objective of this study was to compare the evidence of efficacy of TNFα blockers in terms of ASAS20 response. Since these drugs are very expensive and may only be used in patients with AS after failure of NSAID treatment, it is extremely important to both physicians and decision-makers that the most effective treatment available is chosen. As no head-to-head evidence is available in the literature, MTC evidence structures provide a generalization of Meta-Analysis evidence structures. Instead of simply analyzing a set of Randomized Clinical Trials comparing treatment A vs treatment B, MTC analysis makes it possible to compare trial A vs trial B, trial A vs trial C, trial A vs trial D, trial B vs trial C, and so on. A further advantage of using Bayesian meta-analysis is the possibility of calculating the probabilities of which treatment gives the greatest benefit.
The three studies included in this MTC were placebo-controlled trials having the same primary end-point: ASAS20 response. As mentioned above, these studies do not differ in terms of disease diagnosis criteria, concomitant medication, or in the demographic characteristics of the populations. The fact that the studies had similar disease and demographic characteristics excludes these factors as causing heterogeneity across trials, and therefore the indirect estimate is not affected by bias generated by significant differences.
The result of this MTC suggests that infliximab is expected to provide the greatest ASAS20 response of the anti-TNFα blockers studied in comparison to placebo in the treatment of AS. Infliximab shows a 72% probability of being the best treatment of all those compared with placebo. Adalimumab and etanercept show probabilities of 13% and 15%, respectively.
The lack of a statistically significant difference in the direct comparison between infliximab, adalimumab, and etanercept (one compared to another) can be attributed to the small number of trials examined and sample dispersion. However, adalimumab and etanercept showed a statistically significant difference vs placebo in improving clinical symptoms evaluated by ASAS20.
This information may help physicians choose the best probable treatment management. The Bayesian MTC approach is able to allow a probabilistic interpretation of clinical data and ranking of the interventions. The estimated size of the treatment effect and the associated uncertainty of each intervention are translated into one measure: the probability that a certain treatment, amongst compared treatments, might provide the best outcome. If one considers that infliximab’s 72% probability of providing the best ASAS20 response corresponds to a 28% probability of making the wrong decision, if a biological treatment is prescribed to AS patients in an effort to prescribe the most efficacious treatment of the anti-TNFα agents currently available. To put this in perspective, in the absence of head-to-head studies, each treatment would have a 33% chance of being the best treatment, and thus associated with a 66% probability of making the wrong decision.
Measuring the probability of choosing the most effective treatment may be helpful to physicians in decision-making settings, in which the compliance, tolerability, and safety of each treatment also have to be considered. Moreover, in the case of spondyloarthritis we can also consider the differences in stopping radiological disease progression and not merely the improvement in the clinical surrogate measure, i.e. ASAS20.
The challenge of actual treatments is to prevent radiological damage; however, it remains to be seen whether patients may benefit from a long-term anti-TNF therapy, and whether ankylosis can be delayed or prevented, in which case it will be the most relevant outcome to evaluate. Even if there are no head-to-head RCTs evaluating the differences in stopping radiological progression between the three agents currently used, some data is available on the effect of each one, considered separately. In 2007, Baraliakos et al.Citation27 reported that there is some radiographic progression after 2 and 4 years of infliximab therapy in AS patients, and a comparison with the historical OASIS cohort suggests that infliximab may decelerate the progression of structural changes. In 2010, the same author reported that a definite influence on radiographic progression after long-term continuous treatment with infliximab compared with conventional therapy has not yet been provenCitation28. Recently, van der Heijde et al.Citation29 did not find radiographic progression in patients with AS after 2 years of treatment with adalimumab, as assessed using the modified Stoke AS Spine Score (mSASSS) system, when compared with radiographic data from TNF antagonist-naïve patients. In 2009, the same author reported there was no significant difference in the change in the mSASSS from baseline between patients who received etanercept vs those from the OASIS groupCitation30.
There is no comparative data regarding the safety of treatment using anti-TNF-α agents in AS; however, even long-term studies of each of the three agents analyzed report good safety profiles for all of them when compared to placebo.
As regards patient compliance to anti-TNFα therapy for AS, Pavelka et al.Citation12 reported the follow-up of patients with AS in ATTRA, the Czech National Registry, which showed that it is an efficacious and safe method of treatment and that compliance to anti-TNF therapy was better than amongst RA patients, which suggests a good compliance profile for all anti-TNFα agents.
Another important issue to consider when choosing first-line treatment for AS patients is the cost-effectiveness of each agent. For instance, limited data is available on the optimal dosage of infliximab in AS. In clinical practice, certain patients might not need doses of infliximab higher than 3 mg/kg, but most patients require doses of 5 mg/kg, which leads to an increase in costs. Antibody formation may lead to a loss of efficacy (secondary non-response)Citation28. No dose adjustment is required for adalimumab and etanercept.
These results do have certain limitations. Data from this analysis were extracted analysing only three RCTs, and this may limit the extensibility of the results. As mentioned above, there were differences in trial procedures and populations, although they do not seem to invalidate the results obtained, and, in any case, the MTC technique is able to recognize this possibility and to assess the uncertainty of the estimated RRs. Another limitation of this study is that it is not possible to perform a randomized effect model MTC, on account of the small sample. Indeed, in order to take account of unmeasured or unknown differences in covariates that may act as effects across trials, the use of a random-effect approach should allow us to highlight the possibility of the presence of heterogeneity in the compared trials. In this analysis only a fixed-effect model was used. Another limitation is the small number of trials and anti-TNFα drugs available for comparison.
Conclusions
The result of this study may be relevant for clinical decision-making, contributing to improving the rate of positive ASAS20 response in patients with AS, and it may be relevant also from a social point of view, given the burden of AS affecting the population of working age.
Although the mixed treatment comparisons between infliximab, adalimumab, and etanercept did not show a statistically significant difference, this analysis suggests that infliximab, compared to placebo, is expected to provide the highest rate of ASAS20 response in AS patients.
Transparency
Declaration of funding
This study was performed with unrestricted funds from ANTIAGE (non-lucrative National Association for intra-articular therapy by ultrasound guidance), of which AM is President.
Declaration of interest
The authors declare that no funds were allocated by any sponsors for the execution of this study. AM, BL, and EB have previously received grants as consultants and speakers from Abbott, Pfizer, Merck, Wyeth, andSchering-Plough. JME peer reviewers may have received honoraria for their review work. The peer reviewers on this manuscript have disclosed any relevant financial relationships.
References
- Sieper J. Developments in the scientific and clinical understanding of the spondyloarthritides. Arthritis Res Ther 2009;11:208
- Wittoek R, Mielants H. Clinical assessment in the spondyloarthropathies. Adv Exp Med Biol 2009;649:1–16
- Sengupta R, Stone MA. The assessment of ankylosing spondylitis in clinical practice. Nat Clin Pract Rheumatol 2007;3:496–503
- Brandt J, Sieper J, Braun J. Infliximab in the treatment of active and severe ankylosing spondylitis. Clin Exp Rheumatol 2002;20:S106–10
- Sfikakis PP. The first decade of biologic TNF antagonists in clinical practice: lessons learned, unresolved issues and future directions. Curr Dir Autoimmun 2010;11:180–210
- McCormack PL, Wellington K. Etanercept: in ankylosing spondylitis. BioDrugs 2004;18:199–205; discussion 206
- Breban M, Vignon E, Claudepierre P, et al. Efficacy of infliximab in refractory ankylosing spondylitis: results of a six-month open-label study. Rheumatology (Oxford) 2002;41:1280–5
- Braun J, Davis J, Dougados M, et al. First update of the international ASAS consensus statement for the use of anti-TNF agents in patients with ankylosing spondylitis. Ann Rheum Dis 2006;65:316–20
- European Medicines Agency. Enbrel 25mg powder and solvent for solution for injection: summary of product characteristics (online). http:www.emea.eu. Accessed September 5, 2006
- Maini RN, Breedveld FC, Kalden JR, et al. Therapeutic efficacy of multiple intravenous infusions of anti-tumor necrosis factor α monoclonal antibody combined with low-dose weekly methotrexate in rheumatoid arthritis. Arthritis Rheum 1998;41:1552–63
- Bennett AN, Peterson P, Zain A, et al. Adalimumab in clinical practice. Outcome in 70 rheumatoid arthritis patients, including comparison of patients with and without previous anti-TNF exposure. Rheumatology (Oxford) 2005;44:1026–31
- Pavelka K, Forejtová S, Stolfa J, et al. Anti-TNF therapy of ankylosing spondylitis in clinical practice. Results from the Czech national registry ATTRA. Clin Exp Rheumatol 2009;27:958–63
- Migliore A, Bizzi E, Laganà B, et al. The safety of anti-TNF agents in the elderly. Int J Immunopathol Pharmacol 2009;22:415–26
- Jansen JP, Crawford B, Bergman G, et al. Bayesian meta-analysis of multiple treatment comparisons: an introduction to mixed treatment comparisons. Value Health 2008;11:956–64
- Ades AE, Sculpher M, Sutton A, et al. Bayesian methods for evidence synthesis in cost-effectiveness analysis. Pharmacoeconomics 2006;24:1–19
- Ades AE, Welton N, Lu G. Introduction to mixed treatment comparisons. Bristol, United Kingdom: University of Bristol, 2007
- Caldwell D, Ades A, Higgins J. Simultaneous comparison of multiple treatments: combining direct and indirect evidence. BMJ 2005;331:897–900
- Lu G, Ades AE. Combination of direct and indirect evidence in mixed treatment comparisons. Stat Med 2004;23:3105–24
- van Tubergen A, van der Heijde D, Anderson J, et al. Comparison of statistically derived ASAS improvement criteria for ankylosing spondylitis with clinically relevant improvement according to an expert panel. Ann Rheum Dis 2003;62:215–21
- van der Heijde D, Kivitz A, Schiff MH, et al. Efficacy and safety of adalimumab in patients with ankylosing spondylitis: results of a multicenter, randomized, double-blind, placebo-controlled trial. Arthritis Rheum 2006;54:2136–46
- Davis JC, Jr, Van Der Heijde D, Braun J, et al. Recombinant human tumor necrosis factor receptor (etanercept) for treating ankylosing spondylitis: a randomized, controlled trial. Arthritis Rheum 2003;48:3230–6
- van der Heijde D, Dijkmans B, Geusens P, et al. Ankylosing Spondylitis Study for the evaluation of recombinant infliximab therapy study group. Efficacy and safety of infliximab in patients with ankylosing spondylitis: results of a randomized, placebo-controlled trial (ASSERT). Arthritis Rheum 2005;52:582–91
- Cooper NJ, Sutton AJ, Lu G, et al. Mixed comparison of stroke prevention treatments in individuals with nonrheumatic atrial fibrillation. Arch Intern Med 2006;166:1269–75
- Cipriani A, Furukawa TA, Salanti G, et al. Comparative efficacy and acceptability of 12 new-generation antidepressants: a multiple-treatments meta-analysis. Lancet 2009;373:746–58
- Welton N, Caldwell D, Adamopoulous, E, et al. Mixed treatment comparison meta-analysis of complex interventions: psychological interventions in coronary heart disease. Am J Epidemiol 2009;169:1158–65
- Jansen JP, Bergman GJ, Huels J, et al. Prevention of vertebral fractures in osteoporosis: mixed treatment comparison of bisphosphonate therapies. Curr Med Res Opin 2009;25:1861–8
- Baraliakos X, Listing J, Brandt J, et al. Radiographic progression in patients with ankylosing spondylitis after 4 yrs of treatment with the anti-TNF-alpha antibody infliximab. Rheumatology (Oxford) 2007;46:1450–3
- Baraliakos X, Braun J. Anti-TNF-alpha therapy with infliximab in spondyloarthritides. Expert Rev Clin Immunol 2010;6:9–19
- van der Heijde D, Salonen D, Weissman BN, et al. ATLAS study group assessment of radiographic progression in the spines of patients with ankylosing spondylitis treated with adalimumab for up to 2 years. Arthritis Res Ther 2009;11:R127
- van der Heijde D, Landewé R, Einstein S, et al. Radiographic progression of ankylosing spondylitis after up to two years of treatment with etanercept. Arthritis Rheum 2008;58:1324–3