
Abstract
Objective:
This study was designed to evaluate the cost utility of tocilizumab in rheumatoid arthritis (RA) patients, with inadequate responses to traditional disease-modifying anti-rheumatic drugs (tDMARDs) from a payer’s perspective in Italy.
Methods:
An individual patient simulation model was used to project lifetime medical costs (payer’s perspective) and quality-adjusted life-years (QALYs). Treatment sequences starting with tocilizumab or the most commonly prescribed biologics (etanercept, adalimumab, or infliximab) were compared. The addition of tocilizumab to standard of care, without the replacement of anti-tumor necrosis factor (TNF)-α treatments, was also evaluated. Patient characteristics, treatment efficacy, and quality-of-life data were based on three phase 3 tocilizumab clinical trials (TOcilizumab Pivotal Trial in Methotrexate Inadequate respONders [OPTION], Tocilizumab in cOmbination With traditional DMARD therapy [TOWARD], and TociLIzumab Safety and THE Prevention of Structural Joint Damage [LITHE]). Mixed-treatment comparison was used to estimate response probabilities. Resource utilization, treatment acquisition, administration, and monitoring costs were estimated using Italian secondary sources. Uncertainty in model parameters was evaluated by probabilistic sensitivity analysis.
Results:
Replacement of anti-TNF-α treatments with tocilizumab reduced total costs over a patient’s lifetime (base-case analysis: tocilizumab sequence, €141,100 vs standard of care sequence, €143,500). Patients receiving tocilizumab realized more QALYs than patients receiving standard of care (9.8881 vs 9.3502 QALYs). Therefore, according to the base-case analysis, the tocilizumab sequence dominated the standard of care. In a sensitivity analysis, the model base-case result was robust to input changes. When tocilizumab was added to standard of care, without replacing anti-TNF-α treatments, the incremental cost-effectiveness ratio was €17,100 per QALY.
Conclusion:
The analysis demonstrates that, in Italy, replacing another biologic DMARD with tocilizumab or adding tocilizumab to the current standard of care is a cost-effective strategy in the treatment of RA patients with inadequate responses to tDMARDs.
Introduction
Rheumatoid arthritis (RA) is a chronic, progressive, systemic autoimmune disease that affects joint function and leads to increased disability. The annual prevalence of RA in Italy is ∼272,004 cases (0.46% of the total population)Citation1. The impact of RA on healthcare resource use and productivity loss is considerableCitation2.
Traditional disease-modifying anti-rheumatic drugs (tDMARDs; e.g., methotrexate, leflunomide) are generally used as first-line treatmentsCitation3, primarily because they are available as generics and are inexpensive. Biologic DMARDs (bDMARDs; e.g., etanercept, adalimumab, infliximab) are used in combination with tDMARDs, usually methotrexate, as second-line treatmentsCitation3. Etanercept in combination with methotrexate is the most commonly prescribed treatment after tDMARD failure.
Tocilizumab is a new humanized interleukin-6 (IL-6) receptor monoclonal antibody with a novel mechanism of action that provides a unique treatment option for patients with RA. The efficacy and safety of tocilizumab in patients with an inadequate response to tDMARDs was demonstrated in three phase 3 trialsCitation4–6. The introduction of tocilizumab offers an alternative to anti-tumor necrosis factor-α (anti-TNF-α) cycling, which is often considered an ineffective treatment strategyCitation7.
Several economic evaluations in Italy assessed the cost-effectiveness of bDMARDs, including abatacept, etanercept, and infliximab, compared with methotrexate or other tDMARDsCitation8–10. However, tocilizumab had not been considered in cost-effectiveness analyses in the Italian healthcare environment. Given the clinical effectiveness of tocilizumab, this study was conducted to assess the cost-utility of tocilizumab treatment (RoActemra; Roche, Basel, Switzerland) in Italy compared with other bDMARDs that represent standard of care.
Methods
To synthesize available evidence and extrapolate clinical trial data, an economic model was developed to assess the cost utility of tocilizumab in combination with methotrexate in RA patients with an inadequate response to tDMARDs. The design of the economic analysis follows guidelines set by the Outcome Measures in Rheumatoid Arthritis Clinical Trials (OMERACT) Economics Working GroupCitation11,Citation12.
The model attempts to predict patient outcomes until death. A patient lifetime horizon ensures that all relevant costs and health-related quality-of-life (QoL) impairment are captured in the analysis. Such a model timeframe is in line with most economic analyses in RACitation13–18. The model uses efficacy and QoL data from three phase 3 clinical trials that evaluated tocilizumab in combination with methotrexate, compared with methotrexate alone or an alternative tDMARD aloneCitation4–6. Given that the clinical trial outcomes are available at 6 months, the model is designed to evaluate patient transitions at 6-month intervals (model cycle length).
Patients entered the model after an inadequate response to tDMARDs and progressed through a sequence of treatments that reflect real-life practice scenarios (). In Italy, the standard practice for patients whose tDMARD therapy fails is to prescribe a sequence of bDMARDs in combination with methotrexate. It is assumed that etanercept would be the first bDMARD in the standard-of-care sequence, followed by adalimumab, rituximab, and abatacept. The comparator sequence (with tocilizumab) assumes the replacement of etanercept with tocilizumab, with all subsequent treatments remaining the same (). Comparison of treatment sequences offers an evaluation of patient outcomes mimicking real life and is often used when modeling in RACitation18–20.
Figure 1. Treatment sequences modeled.
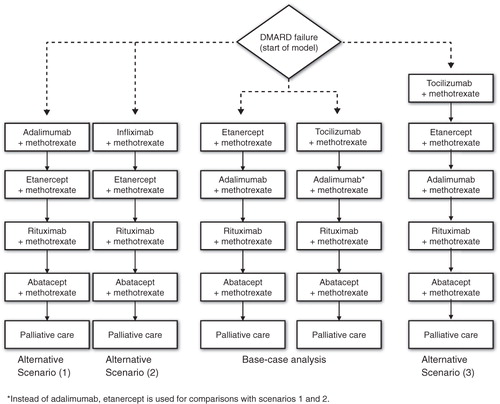
For completeness, the analysis considered three alternative scenarios. The first scenario reversed the order of the first two biologic treatments, using adalimumab ahead of etanercept as standard treatment. In this scenario, the evaluation compared the replacement of adalimumab, rather than etanercept, by tocilizumab; etanercept followed in the sequence after both treatment comparators. The second scenario was the same as the previous one but assumed that the comparison was with infliximab instead of adalimumab. The third scenario assumed no anti-TNF-α treatment replacement and evaluated the addition of tocilizumab in combination with methotrexate at the start of the standard-of-care sequence.
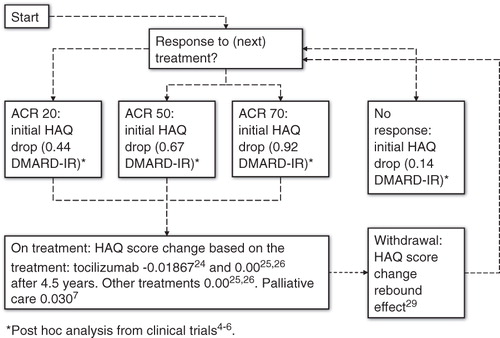
American College of Rheumatology (ACR) response rates were used as a measure of initial treatment efficacy. Based on ACR response rates, simulated individuals were allocated to one of four categories: no response, ACR20 response, ACR50 response, or ACR70 response. Those with no response moved to the next treatment in the sequence, whereas those with a response remained on treatment until withdrawal, with significant changes in QoL and costs.
Given the absence of head-to-head ACR response data and the sequential form of the model structure, results from a Bayesian mixed-treatment comparison (MTC) were used to assign appropriate ACR data according to the position of each treatment in the sequence. ACR response probabilities for tocilizumab and etanercept, each in combination with methotrexate, were derived from Bergman et al.Citation21 Data from another MTC in an anti-TNF-α failure population were used for ACR responses to rituximab and abatacept, each in combination with methotrexate (Supplementary Digital Content Appendix A). Because of a lack of evidence about efficacy after bDMARD (etanercept or tocilizumab) failure, the response rates of adalimumab in combination with methotrexate were reduced by 30%Citation7.
Disease severity and, consequently, QoL are reflected in the model by changes in patient Health Assessment Questionnaire (HAQ) scoresCitation18,Citation20. Patient characteristics (such as age, sex, baseline HAQ score, and weight) were obtained from the clinical trialsCitation4–6. These parameters were maintained across the simulated cohort at the start of the model, assuming an homogeneous group of patients. As patients progressed through treatment, individual simulation was used to monitor HAQ score changes and projected costs and outcomes. Individual simulation was preferred to cohort analysis for computational reasons; accrued health benefits and costs depend on a large number of values for the HAQ score parameterCitation22,Citation23.
Response to treatment was assumed to have an impact on disease severity, as measured by individual HAQ score. Data on the relationship between ACR responses and patient HAQ scores were obtained from the clinical trials and corresponded to the first 24 weeks after baseline, suggesting that the higher the observed response, the greater the drop in HAQ score (Citation4–7,Citation21,Citation24–26). For the first 6 months of a new treatment, the model assumed a HAQ score reduction according to the level of response: ACR20, ACR50, or ACR70. This HAQ score benefit was assumed to be response-related, not treatment-related, and therefore was applied universally to all bDMARDs.
Table 1. Economic model parameters.
After response to treatment, the model assumes no HAQ score progressionCitation25,Citation26. Moreover, the model incorporates data from a recent analysis of the three clinical trials for HAQ score progression during administration of tocilizumab in combination with methotrexateCitation24. The analysis suggested a functional improvement for patients receiving tocilizumab, reflected by a negative slope of the patient average HAQ score. Observations before week 24 were excluded because initial response to treatment was expected during this period, and a decline in HAQ score was already modeled. Because the data cut-off used in the analysisCitation24 is at 4.5 years, the model conservatively assumes no improvement after that time point for patients continuing on tocilizumab combination therapyCitation25,Citation26. Once patients exhaust all possible treatment options and enter palliative care, they experience disease deterioration reflected by a significant HAQ score increase of 0.03 every 6 monthsCitation7.
Data from Geboreck et al.Citation27 suggest that withdrawal rates at 6 months, for etanercept and infliximab, are 8% and 12%, respectively. These estimates are congruent with data from Bansback et al.Citation28 The current model assumes a withdrawal risk equal to the average of the two estimates for all treatments. At the point of withdrawal, patients were assumed to lose the acquired benefit with response to treatment and rebound to a higher HAQ scoreCitation29. A summary of HAQ score change from treatment response to withdrawal for each modeled individual is presented in Citation7,Citation24–26.
Figure 2. Change in individual HAQ scores.
Health-related QoL
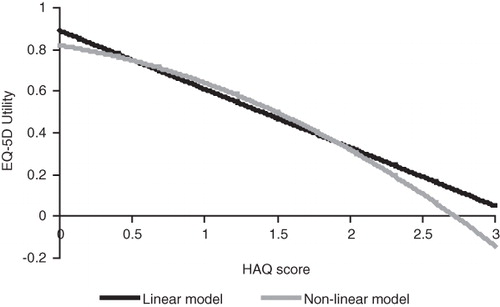
A mechanism of mapping utility from patient HAQ score was incorporated into the model to derive health-related QoL estimates (equation 1). This technique is similar to that of previously published cost-utility studies and reimbursement submissions of biologic treatments in RACitation28,Citation29. The method is modified herein to reflect data from the clinical trials. The utility mapping model is presented in detail in Supplementary Digital Content Appendix B.
The base-case analysis uses equation (1), reflecting the assumption that decreases in HAQ level are more valuable (as measured by change in utility) for severely disabled patients than for patients who are less disabled. Sensitivity analyses tested alternative utility mapping scenarios assuming a linear relationship between the two model parameters ().
Figure 3. Utility–HAQ score mapping models.
Treatment-related costs and resource utilization
The economic evaluation reflects the Italian National Health Service perspective with all relevant healthcare costs. The acquisition costs of bDMARDs were calculated based on hospital prices. For methotrexate, which is available in public pharmacies, a public price that included distribution margins was used. Dosage information was combined with acquisition prices to estimate the annual costs of treatment ()Citation31. All bDMARDs were considered in combination with methotrexate.
Table 2. Treatment acquisition costs (hospital acquisition prices)Citation31.
For infusion administrations (tocilizumab, abatacept, infliximab, and rituximab; Citation31--33), healthcare personnel time was estimated based on an Italian retrospective study, which assessed resource consumption for 100 RA patients treated with infliximabCitation31: rheumatologist time per cycle was 15 minutes, and nurse time was 20 minutes (calculated on a 180-minute infusion). For tocilizumab, rituximab, and abatacept, the model assumed the same rheumatologist time, whereas nurse time was recalculated proportionally to the time of infusion. For subcutaneous administration (etanercept and adalimumab), an average of 4.5 minutes was assumedCitation32. The costs per minute for nurses and rheumatologists were assumed to be €0.43 and €0.97, respectivelyCitation33.
Table 3. Treatment administration costsCitation31–33.
Direct medical costs, other than drug acquisition and administration costs, were obtained from an Italian retrospective, prevalence-based, multi-center study of 200 patients ()Citation2. Direct medical costs were associated with the four ACR response classes to reflect costs per patient associated with disease severity. The HAQ score for each ACR response class was associated with different HAQ scores based on the National Databank for Rheumatic Disease ()Citation9; 2002 prices were inflated to 2009 prices using data from the Italian Institute for StatisticsCitation34. Future costs and quality-adjusted life-years (QALYs) were discounted at an annual 3.0% rate.
Table 4. Annual direct medical costs per patient based on ACR functional classCitation2.
Table 5. HAQ score-related direct medical costsCitation9,Citation34.
All assumptions were presented to and validated by the involved clinical and health economic experts. Several sensitivity analyses tested the robustness of the model to input changes. Moreover, parameter uncertainty was addressed by fitting appropriate distributions to model variables and running probabilistic sensitivity analysis (PSA). Supplementary Digital Content Appendix C presents details on the sampling distributions used.
Results
Ten thousand simulation trials were run. On average, the medical cost for standard of care was estimated to be higher than the sequence with tocilizumab (€143,500 vs €141,100). The drivers of this cost difference were the lower price of tocilizumab and the decreased use of medical resources. Moreover, patients in the tocilizumab sequence realized more utility benefits than patients in the standard-of-care sequence, which translated to an increment of ∼0.54 (9.3502 vs 9.8881) QALYs. Therefore, given current prices in Italy, RA patients with an inadequate response to tDMARDs incur lower costs and have higher QoL; in other words, the tocilizumab sequence dominated the standard-of-care sequence ().
Table 6. Economic model results.
Several analyses tested the sensitivity of the model to input changes. (Note that sensitivity analysis is presented with changes to the base-case scenario, as in [comparison with etanercept].) Model estimates were fairly robust to input changes, and the tocilizumab sequence dominated the standard-of-care sequence in most comparisons. The model was sensitive to changes in HAQ score progression during treatment. Changes to this parameter had an impact on patient QoL. As scenario C in illustrates, when HAQ score progression was assumed to be zero for tocilizumab, the incremental QALY benefit was reduced from 0.54 to 0.06 QALYs in the base case analysis. Other changes to the model structure (withdrawal, scenario B) or parameter values (scenarios A, D, E, F, G, H, I) had little impact on the model results ().
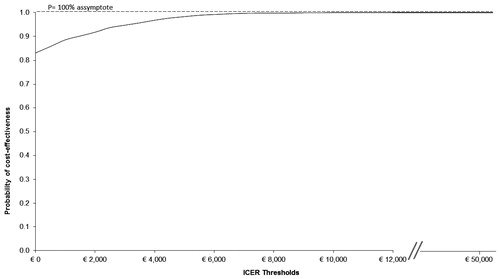
In PSA, more than 80% of the samples fell within the fourth quadrant, suggesting that the tocilizumab sequence dominated the alternative (). There were no samples represented in the second quadrant, where tocilizumab would be dominated by the alternative (). The probability that the intervention was cost-effective was 100% when considering a cost-effectiveness threshold of €50,000 per QALY gained ().
Figure 4. Cost-effectiveness scatter plot.
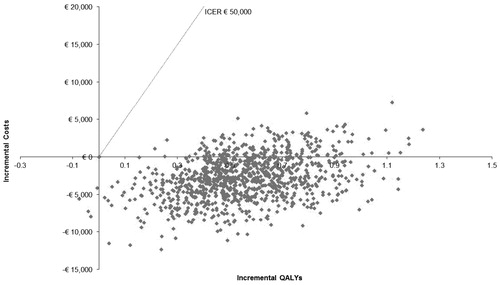
Figure 5. Cost-effectiveness acceptability curve.
In the first alternative scenario, in which adalimumab was prescribed before etanercept, the model produced similar results (). In the second scenario, in which infliximab was prescribed before etanercept, the incremental cost-effectiveness ratio (ICER) was estimated at €2600 per QALY gained. In the third scenario, in which the analysis assumed no anti-TNF-α treatment replacement and the addition of tocilizumab to the clinician’s treatment options, the ICER was €17,100 per QALY gained.
Discussion
Three large, multinational, randomized, phase 3 clinical trials demonstrated favorable results for tocilizumab in combination with methotrexate, compared with methotrexate alone, in patients with an inadequate response to at least one tDMARD. The present study synthesizes evidence from these studies with data from the published literature, extrapolates patient outcomes to lifetime, and translates the clinical evidence to a cost-utility analysis.
Other economic studies in the treatment of RA focus on the initial clinical benefit and cost of interventions (6-month time frame)Citation8,Citation10. In such cases, the analysis is based entirely on clinical trial data, and no assumptions are necessary for the long-term disease progression in patients. However, given the chronic nature of RA, a long-term time frame of analysis is more relevant to decision-makers. Cost-effectiveness results from short-term analyses are likely to be under-estimated because not all relevant costs and QALYs are included.
Because no head-to-head comparisons between tocilizumab and anti-TNF-α agents (adalimumab and etanercept) have been made, the model considers relative efficacy between these biologics, as estimated by an MTC. The response probability of adalimumab is further adjusted to reflect its anti-TNF-α inadequate response (TNF-IR) position in the standard-of-care sequence. Although the adjustment represents loss of treatment efficacy from anti-TNF-α cycling, this adjustment is conservatively assumed to appear also after tocilizumab, where anti-TNF-α cycling is not modeled. A second MTC among rituximab, abatacept, and tocilizumab was used to provide relative efficacy data in TNF-IR positions for these treatments. Given the uncertainty surrounding these estimates, a sensitivity analysis based on ACR response rates was conducted; ACR response was not a major driver of the model results.
Further assumptions on the lifetime disease severity of simulated individuals were necessary to complete the analysis. The simulation of individual HAQ score progression was used to represent changes in disease severityCitation18,Citation20. Therefore, HAQ score change at treatment initiation was based on clinical trial evidence, which reflected only tocilizumab. However, that the observed improvement was response-related, not treatment-related, is a reasonable assumption; hence, the benefit from response was applied universally to all treatments.
To extrapolate HAQ score beyond clinical trial duration, an assumption was necessary. In the past, similar economic evaluations have assumed a positive HAQ score progression, reflecting a slow deterioration in disease severityCitation20. More recently, a distinction was made between the levels of deterioration associated with bDMARDs and tDMARDs. Based on data from long-term extension trials, patients receiving anti-TNF-α treatments were assumed to experience stable HAQ score progression while on treatmentCitation24,Citation25. Our model uses data on HAQ score progression for tocilizumab, which suggest a clear improvement of HAQ score in patients who continue to receive tocilizumab for up to 4.5 years (for when data exist).
Moreover, recent observational data collected in patients treated with biologics other than tocilizumab suggest a reduced impact on disease progression in real life compared with data from clinical trialsCitation35. The current analysis considers this by assigning stable HAQ progression to tocilizumab in a sensitivity analysis. In this scenario, the tocilizumab regimen continues to dominate the standard of care (case C in ).
The QoL associated with RA and the benefits from each treatment were based on a post-hoc analysis of clinical trial data. A method to obtain QALYs from HAQ score was used. Similar methods of HAQ and EQ-5D mapping are commonly used in RA modelingCitation28,Citation29. The present study improves this technique by introducing a non-linear relationship between the two parameters. This reflects the assumption that improvements in QoL are more valuable for patients with severe RA.
Treatment costs are shown to be important drivers of the economic model, whereas the implications to resource use of adopting tocilizumab as a standard of care are not large-scale (sensitivity analysis G). Therefore, the generalizability of the model results to other countries depends on the relative difference between tocilizumab and the other bDMARD prices.
The analysis does not include adverse events (AEs) from treatment. However, since the included treatments have a similar safety profile, inclusion of AEs would not have any impact on the incremental cost-effectiveness results. Although the implications of AEs on costs and patient utility are not introduced into the model, they are indirectly reflected in the treatment withdrawal rates. In addition, the disutility associated with treatment-related AEs has been captured in the EQ-5D utility data collected in the tocilizumab phase 3 trials.
Further research is necessary to provide information about the relative efficacy of the treatments in different populations (DMARD-IR and TNF-IR). The availability of head-to-head comparisons would help in validating the MTC results this economic analysis uses. Moreover, data on long-term disease progression would improve assumptions of the economic model and provide the platform for long-term assessment of biologic treatments. Nevertheless, as illustrated in the sensitivity analysis, although these developments would improve accuracy, a significant change in the direction of the results is unlikely.
Conclusion
The analysis demonstrates that, in Italy, replacing another bDMARD with tocilizumab or adding tocilizumab to the current standard of care is a cost-effective strategy in the treatment of RA patients with an inadequate response to tDMARDs.
Declaration of interest
This study was funded by F. Hoffmann-La Roche Ltd. Roche was specifically involved in the collection of drug costs and RA management costs from published sources, preparation of mixed treatment comparisons, mapping Health Assessment Questionnaire (HAQ) data to EuroQoL-5D (EQ-5D), analysing clinical trial data for specific modeling purposes, running modeling analyses, and presenting and discussing results.
Transparency
Declaration of financial/other interests
M.B., S.C., and W.R. have disclosed that they received funds as consultants of F. Hoffmann-La Roche Ltd, and A.D. reports that he received funds as a consultant from the same. W.B., N.W., and G.G. have disclosed that they are employees of F. Hoffmann-La Roche Ltd.
Supplementary Material
Download PDF (164.5 KB)Acknowledgment
Maribeth Bogush, PhD, and David Murdoch, MB ChB, provided writing assistance for this manuscript, which was paid for by F. Hoffmann-La Roche Ltd.
References
- Salaffi F, De Angelis R, Grassi W. MArche Pain Prevalence INvestigation Group (MAPPING) study. Prevalence of musculoskeletal conditions in an Italian population sample: results of a regional community-based study, I: the MAPPING study. Clin Exp Rheumatol 2005;23:819–28
- Leardini G, Salaffi F, Montanelli R, et al. A multicenter cost-of-illness study on rheumatoid arthritis in Italy. Clin Exp Rheumatol 2002;20:505–15
- Smolen JS, Landewé R, Breedveld FC, et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs. Ann Rheum Dis 2010;69:964–75
- Smolen JS, Beaulieu A, Rubbert-Roth A, et al. OPTION Investigators. Effect of interleukin-6 receptor inhibition with tocilizumab in patients with rheumatoid arthritis (OPTION study): a double-blind, placebo-controlled, randomized trial. Lancet 2008;371:987–97
- Genovese MC, McKay JD, Nasonov EL, et al. Interleukin-6 inhibition with tocilizumab reduces disease activity in rheumatoid arthritis with inadequate response to disease-modifying antirheumatic drugs: the tocilizumab in combination with traditional disease-modifying antirheumatic drug therapy study. Arthritis Rheum 2008;58:2968–80
- Fleischmann R, Burgos-Vargas R, Ambs P, et al. LITHE: tocilizumab inhibits radiographic progression and improves physical function in rheumatoid arthritis (RA) patients (Pts) at 2 yrs with increasing clinical efficacy over time [abstract]. Arthritis Rheum 2009;60(10 Suppl):637
- National Institute for Health and Clinical Excellence. NICE technology appraisal guidance (130): adalimumab, etanercept and infliximab for the treatment of rheumatoid arthritis. Issued October 2007. http://www.nice.org.uk/nicemedia/pdf/TA130guidance.pdf. Accessed March 30, 2011
- Benucci M, Li Gobbi F, Sabadini L, et al. The economic burden of biological therapy in rheumatoid arthritis in clinical practice: cost-effectiveness analysis of sub-cutaneous anti-TNFα treatment in Italian patients. Int J Immunopathol Pharmacol 2009;22:1147–52
- De Portu S, Mantovani LG, Olivieri I. Analisi di costo-utilità di abatacept nell’artrite reumatoide in Italia. Farmeconomia e Percorsi Terapeutici 2008;9:19–26
- Leardini G, Ganguly R, Singh A. Cost-effectiveness analysis of etanercept versus infliximab and anakinra in the treatment of rheumatoid arthritis in Italy [abstract 1152]. 67th Annual Scientific Meeting of the American College of Rheumatology (ACR), 23-28 October 2003, Orlando, FL
- Gabriel S, Drummond M, Maetzel A, et al. Patient Perspective Group. OMERACT 6 Economics Working Group report: a proposal for a reference case for economic evaluation in rheumatoid arthritis. J Rheumatol 2003;30:886–90
- Maetzel A, Tugwell P, Boers M, et al. OMERACT 6 Economics Research Group. Economic evaluation of programs or interventions in the management of rheumatoid arthritis: defining a consensus-based reference case. J Rheumatol 2003;30:891–6
- Kielhorn A, Porter D, Diamantopoulos A, et al. UK cost-utility analysis of rituximab in patients with rheumatoid arthritis that failed to respond adequately to a biologic disease-modifying antirheumatic drug. Curr Med Res Opin 2008;24:2639–50
- Wailoo AJ, Bansback N, Brennan A, et al. Biologic drugs for rheumatoid arthritis in the Medicare program: a cost-effectiveness analysis. Arthritis Rheum 2008;58:939–46
- Vera-Llonch M, Massarotti E, Wolfe F, et al. Cost-effectiveness of abatacept in patients with moderately to severely active rheumatoid arthritis and inadequate response to tumor necrosis factor-(alpha) antagonists. J Rheumatol 2008;35:1745–53
- Brennan A, Bansback N, Nixon R, et al. Modelling the cost effectiveness of TNF-(alpha) antagonists in the management of rheumatoid arthritis: results from the British Society for Rheumatology Biologics Registry. Rheumatology (UK) 2007;46:1345–54
- Spalding JR, Hay J. Cost effectiveness of tumour necrosis factor-alpha inhibitors as first-line agents in rheumatoid arthritis. Pharmacoeconomics 2006;24:1221–32
- Chen YF, Jobanputra P, Barton P, et al. A systematic review of the effectiveness of adalimumab, etanercept and infliximab for the treatment of rheumatoid arthritis in adults and an economic evaluation of their cost-effectiveness [abstract]. Health Technol Assess 2006;10:248
- Jobanputra P, Barton P, Bryan S, et al. The effectiveness of infliximab and etanercept for the treatment of rheumatoid arthritis: a systematic review and economic evaluation. Health Technol Assess 2002;6:1–110
- Barton P, Jobanputra P, Wilson J, et al. The use of modelling to evaluate new drugs for patients with a chronic condition: the case of antibodies against tumour necrosis factor in rheumatoid arthritis. Health Technol Assess 2004;8:1–91
- Bergman GJ, Hochberg MC, Boers M, et al. Indirect comparison of tocilizumab and other biologic agents in patients with rheumatoid arthritis and inadequate response to disease-modifying antirheumatic drugs. Semin Arthritis Rheum 2010;39:425–41
- Brennan A, Chick SE, Davies R. A taxonomy of model structures for economic evaluation of health technologies. Health Econ 2006;15:1295–310
- Davies R, Roderick P, Raftery J. The evaluation of disease prevention and treatment using simulation models. Eur J Operational Res 2003;150:53–66
- van Vollenhoven R, Ducournau P, Wintfeld N, et al. Health Assessment Questionnaire-Disability Index scores in patients with rheumatoid arthritis treated with tocilizumab plus conventional anti-rheumatic drugs. Presented at: ISPOR 12th Annual European Congress, 24-27 October 2009, Paris, France
- Landewé RB, Boers M, Verhoeven AC, et al. COBRA combination therapy in patients with early rheumatoid arthritis: long-term structural benefits of a brief intervention. Arthritis Rheum 2002;46:347–56
- Weinblatt ME, Keystone EC, Furst DE, et al. Change over time in the safety, efficacy, and remission profiles of patients with rheumatoid arthritis receiving adalimumab for up to 7 years. Presented at: American College of Rheumatology 2007 Annual Scientific Meeting, 10-11 November 2007, Boston, MA
- Geborek P, Crnkic M, Petersson IF, et al. Etanercept, infliximab and leflunomide in established rheumatoid arthritis: clinical experience using a structured follow up programme in southern Sweden. Ann Rheum Dis 2002;61:793–8
- Bansback N, Brennan A, Ghatnekar O. Cost effectiveness of adalimumab in the treatment of patients with moderate to severe rheumatoid arthritis in Sweden. Ann Rheum Dis 2005;64:995–1002
- Brennan A, Bansback N, Reynolds A, et al. Modelling the cost-effectiveness of etanercept in adults with rheumatoid arthritis in the UK. Rheumatology 2004;43:62–72
- Boggs R, Sengupta N, Ashraf T. Estimating health utility from a physical function assessment in rheumatoid arthritis (RA) patients treated with adalimumab (HUMIRA) [abstract UT3]. Presented at: 7th International Society of Pharmacoeconomics and Outcomes Research, 19-22 May 2002, Arlington, VA
- Favalli EG, Marchesoni A, Colombo GL, et al. Pattern of use, economic burden and vial optimization of infliximab for rheumatoid arthritis in Italy. Clin Exp Rheumatol 2008;26:45–51
- Rubio-Terrés C, Ordovàs Baines JP, Pla Poblador R, et al. Grupo de Investigadores del Estudio PRAXIS. [Use and cost of biological disease-modifying anti-rheumatic drugs in Spain (PRAXIS study)] [Spanish]. Farm Hosp 2007;31:71–92
- Benucci M, Iannazzo S, Zaniolo O, et al. Rituximab in the treatment of rheumatoid arthritis patients in Italy: a budget impact analysis. Clin Exp Rheumatol 2010;28:722–7
- ISTAT Italian Institute of Statistics 2009. Coefficienti per tradurre valori monetari dei periodi sottoindicati in valori del 2010 (a). http://www.istat.it/prezzi/precon/rivalutazioni/val_moneta_2010.zip. Accessed February 7, 2011
- Wolfe F, Michaud K. The loss of health status in rheumatoid arthritis and effect of biologic therapy: a longitudinal observation study. Arthritis Res Ther 2010;12:R35