
Abstract
Objective:
With increasing healthcare resource constraints, it has become important to understand the incremental cost-effectiveness of new medicines. Subcutaneous denosumab is superior to intravenous zoledronic acid (ZA) for the prevention of skeletal-related events (SREs) in patients with advanced solid tumors and bone metastases. This study sought to determine the lifetime cost-effectiveness of denosumab vs ZA in this setting, from a US managed-care perspective.
Methods:
A lifetime Markov model was developed, with relative rate reductions in SREs for denosumab vs ZA derived from three pivotal Phase 3 trials involving patients with castration-resistant prostate cancer (CRPC), breast cancer, and non-small-cell lung cancer (NSCLC), and bone metastases. The real-world SRE rates in ZA-treated patients were derived from a large commercial database. SRE and treatment administration quality-adjusted life year (QALY) decrements were estimated with time-trade-off studies. SRE costs were estimated from a nationally representative commercial claims database. Drug, drug administration, and renal monitoring costs were included. Costs and QALYs were discounted at 3% annually. One-way and probabilistic sensitivity analyses were conducted.
Results:
Across tumor types, denosumab was associated with a reduced number of SREs, increased QALYs, and increased lifetime total costs vs ZA. The costs per QALY gained for denosumab vs ZA in CRPC, breast cancer, and NSCLC were $49,405, $78,915, and $67,931, respectively, commonly considered good value in the US. Costs per SRE avoided were $8567, $13,557, and $10,513, respectively. Results were sensitive to drug costs and SRE rates.
Limitations:
Differences in pain severity and analgesic use favoring denosumab over ZA were not captured. Mortality was extrapolated from fitted generalized gamma function beyond the trial duration.
Conclusion:
Denosumab is a cost-effective treatment option for the prevention of SREs in patients with advanced solid tumors and bone metastases compared to ZA. The overall value of denosumab is based on superior efficacy, favorable safety, and more efficient administration.
Introduction
Bone is one of the most common sites of distant metastases among patients with cancer: up to 75% of patients with advanced prostate and breast cancers will develop metastatic bone disease, as will ∼40% of patients with advanced lung cancerCitation1.
Bone metastases can induce bone destruction (primarily through increased osteoclast activity), which places patients at risk of skeletal-related events (SREs)Citation2,Citation3. SREs include pathological fractures that may impair ambulation; spinal cord compressions that can result in numbness or weakness, urinary or fecal incontinence, and paralysis; the need for radiation therapy to bone to control local tumor burden and manage pain; and the need to undergo surgery to bone to prevent or treat pathologic fracturesCitation4,Citation5. SREs secondary to bone metastases can be painful and debilitating, and can result in reduced health-related quality-of-life (HRQoL)Citation6. SREs are also costly to manageCitation7. In the US, patients with bone metastases secondary to breast cancer who experienced an SRE incurred significantly higher total medical costs compared with those who did not experience an SRE over a 60-month period ($115,542 vs $67,369Citation8), with most of the total economic burden—nearly 60%—relating to SREs requiring hospitalizationCitation8. The mean reimbursed amount per hospital admission associated with SREs across tumor types has been estimated at ∼$31,000–$42,000 for bone surgery, $22,000–$27,000 for pathologic fracture, and $44,000–$60,000 for spinal cord compressionCitation9.
The bisphosphonate zoledronic acid (4 mg given intravenously [IV] once every 3–4 weeks) is frequently utilized in the US to delay or prevent SREs in patients with bone metastases secondary to advanced solid tumorsCitation10. However, a significant proportion of patients still experience SREs despite treatment with IV zoledronic acidCitation11–13. In addition, zoledronic acid is associated with renal toxicity, such that serum creatinine monitoring is required before each dose, and dose reduction or dose delay is required in patients with renal impairmentCitation14. Furthermore, zoledronic acid is specified to be infused intravenously over no less than 15 minutesCitation14.
Denosumab (XGEVA®) is a fully human monoclonal antibody against RANK ligand that inhibits osteoclast-mediated bone destructionCitation15. In three large, pivotal Phase 3 international clinical trials, denosumab 120 mg subcutaneously (SC) every 4 weeks demonstrated superior efficacy over IV zoledronic acid for the prevention of SREs in patients with bone metastases secondary to castration-resistant prostate cancer (CRPC)Citation16, advanced breast cancerCitation17, and other advanced solid tumorsCitation18. Overall, denosumab significantly delayed time to first on-study SRE (HR: 0.83; 95% CI: 0.76–0.90; p < 0.001) as well as time to first and subsequent on-study SREs (HR: 0.82; 95% CI: 0.75–0.89; p < 0.001) compared with zoledronic acid (n = 2862 denosumab; n = 2861 zoledronic acid)Citation19. Denosumab also delayed the onset of moderate or severe pain compared with zoledronic acidCitation20–22, and maintained HRQoL in patients with solid tumors and bone metastasesCitation23,Citation24. Unlike zoledronic acid, denosumab can be used in patients regardless of renal status or concomitant use of nephrotoxic agents, with no renal monitoring or dose adjustments requiredCitation25.
With increasing healthcare resource constraintsCitation26, it is important to understand the relative benefits and costs of new treatmentsCitation27, and this is particularly informative to payers when making formulary decisions. Since the approval of denosumab for the prevention of SREs by the US Food and Drug Administration in November 2010, there has been great interest in the assessment of its relative economic valueCitation28,Citation29. A recently published cost-effectiveness analysisCitation30 was intended to delineate the cost-effectiveness of denosumab vs zoledronic acid for the prevention of SREs among patients with CRPC and bone metastases. However, it was associated with a number of limitations, including the under-estimation of the true incidence of skeletal complications in oncology, thus limiting the accurate assessment of the cost-effectiveness of denosumab and zoledronic acid in this patient group31. Furthermore, corresponding data in other tumor types have not yet been published.
We therefore sought to determine the cost-effectiveness of denosumab relative to zoledronic acid for the prevention of SREs among patients with bone metastases secondary to CRPC, breast cancer, or NSCLC, based on a lifetime Markov cohort model from a US managed care perspective. We aimed to obtain incremental cost-effectiveness ratios (ICERs) including cost per quality-adjusted life year (QALY) gained and cost per SRE avoided.
Methods
Design
A lifetime Markov cohort model was constructed from the US managed care perspective. It was structured identically for both treatments (denosumab and zoledronic acid) and across all tumor types (CRPC, breast cancer, and NSCLC), with treatment- and tumor- specific model inputs.
A Markov model is a type of mathematical model containing a finite number of mutually exclusive and exhaustive health states, having time periods (cycles) of uniform length and in which the probability of movement from one state to another depends on the current state and remains constant over timeCitation32.
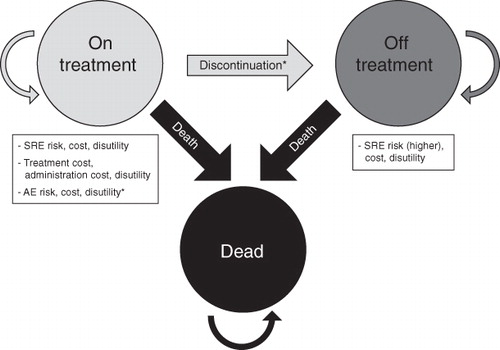
In this analysis, the Markov model consisted of three Markov health states (On Treatment, Off Treatment, and Dead). When a patient was in the ‘On Treatment’ Markov state, there was a risk for SREs, bone-modifying agent treatment-related adverse events (AEs), and death. When a patient was in the ‘Off Treatment’ Markov state, there was a higher risk of SREs, an unchanged risk of death, and no risk of bone-modifying agent treatment-related AEs. In the model, costs were a consequence of treatment, drug administration, SREs, and AEs; declines in utility from baseline (expressed as decrements in QALYs) were a consequence of SREs, the administration of drugs to prevent SREs, and AEs ().
Figure 1. Depiction of Markov model states. *Not included in the base case scenario. SRE, skeletal-related event; AE, adverse event.
The model cycle length was 28 days (or 4 weeks), consistent with the dose frequency of the two treatments and previous published cost-effectiveness analyses of bone-modifying agents in the treatment of bone metastasesCitation33. Given that the nature of a Markov cohort model is to predict the events for each cycle, which does not allow for multiple events within one cycle, a longer cycle length was not considered appropriate as patients are more likely to develop multiple SREs over longer periods of time.
As SREs may occur throughout the entire remaining lifespan of patients with bone metastases, the time horizon for this cost-effectiveness analysis was a lifetime, thus extending far enough into the future to capture all major health and economic outcomesCitation32. Specifically, the model was run for 200 cycles (15.33 years), after which more than 99% of patients had transitioned to the ‘Dead’ health state, with more than 70% of patients transitioning to this state within the first 24–48 cycles (i.e., 2–4 years) of the model, depending on tumor type.
Model event parameters
For each Markov cycle, the model event parameters in this cost-effectiveness analysis included probabilities of SREs, probabilities of death, probabilities of drug discontinuation, and probabilities of AEs. These model probabilities were derived largely from the results of the three pivotal Phase 3 clinical trials, in which SC denosumab 120 mg every 4 weeks was compared with IV zoledronic acid 4 mg every 4 weeks for the prevention of SREs in patients with bone metastases secondary to CRPC (n = 1901)Citation16, advanced breast cancer (n = 2046)Citation17, and other advanced solid tumors (including NSCLC) or multiple myeloma (n = 1776)Citation18. The last of these studies included patients with multiple tumor types. We selected data from patients with NSCLC for inclusion in the model as these patients represented a significant sub-set of the overall study population (702/1776 patients; 40%)Citation18,Citation34 and a suitably homogeneous sub-population. The primary end-point in all three of these studies was time to first on-study SRE (with SREs defined as pathologic fracture, radiation or surgery to bone, or spinal cord compression)Citation16–18.
The model was based on constant rates for SREs, drug discontinuation, and AEs over the lifetime of the patient, and the corresponding probabilities in each cycle were derived from the rates by assuming an exponential relationship between rates and probabilities. This approach is consistent with other published cost-effectiveness literature in this therapeutic areaCitation35. It also presents a straightforward method of extrapolating results beyond the time frame of the clinical trialsCitation16,Citation17.
Probability of skeletal-related events
To ensure that the model better reflected the US managed care perspective, SRE rates in clinical practice in each treatment group were derived by comparing published rates derived from the managed care setting as captured in a large commercial database (PharMetrics integrated claims database, a nationally-representative database of medical and pharmaceutical claims that includes 80 US health plans and covers 55 million patients)Citation10 and SRE rates (total number of SREs divided by total patient follow-up time) reported in the denosumab Phase 3 clinical trialsCitation16,Citation17. An adjustment factor of 2.01 was derived and was used to adjust the trial-based SRE rates for zoledronic acid-treated patients in the model. The SRE rates for denosumab-treated patients were then calculated by applying the treatment effects from the Phase 3 clinical trials. The adjusted annual SRE rates in clinical practice for denosumab and zoledronic acid were 1.500 and 1.903, respectively, in the CRPC model; 0.980 and 1.267, respectively, in the breast cancer model; and 2.242 and 2.634, respectively, in the NSCLC model ().
Table 1. Skeletal-related event and drug discontinuation rates included in the model.
Probability of death
Overall survival was not significantly different between the two treatment groups in the randomized clinical trialsCitation16–18, therefore the generalized gamma functions were fitted using mortality data pooled across both treatment groups for each tumor type, to avoid random survival differences. The generalized gamma function was selected based on a comparison against other parametric models including: Weibull, log-logistic, log-normal, exponential, normal, logistic, and extreme value according to log likelihood or the Akaike Information Criterion (AIC).
Probability of drug discontinuation
Due to a lack of data from clinical practice, discontinuation of therapy was incorporated into the model based on the discontinuation rate from each clinical trial (excluding discontinuation due to death, which was already accounted for in the model by the mortality inputs)Citation16,Citation17 (). The model assumed that SRE rates increased after discontinuation of therapy. The placebo rates from other trials were used as a proxy for the effects of discontinuation on outcomes in the absence of published data. The SRE rate for patients who discontinued either treatment was assumed to be 1.75-times higher than the SRE rate in the zoledronic acid-treated patientsCitation36,Citation37. Drug discontinuations were not considered in the base case analyses, but were included in a separate scenario analysis.
Probability of adverse events
It is generally not feasible to include all possible AEs in cost-effectiveness models as the models would become too complex. Since most AEs are infrequent, not related to drug administration, and many have little to no effect on the results of economic models, only clinically and economically important AEs, including osteonecrosis of the jaw (ONJ), acute phase reactions, hypocalcemia, and renal toxicity, were included in the model. The rates of these four AEs were estimated for denosumab and for zoledronic acid based on the integrated safety results across all three Phase 3 clinical studies to help provide more stable rates. Rates of AEs were calculated by using the total number of patients with each AE, and dividing by the person-time on study over which patients were followed for AEs. Adverse events were not included in the base case analyses, but were included in a separate scenario analysis.
Model utilities
Utility refers to the preference of a patient for a particular health outcome or health stateCitation32. In this cost-effectiveness analysis, the baseline utility for patients with advanced solid tumors and bone metastases was estimated using the EuroQoL 5-Dimensions (EQ-5D) data from the three Phase 3 trials pooled across all patients who did not have any on-study SREs ().
Table 2. Baseline utilities and skeletal-related event QALY decrements.
The QALY is a measure of health outcome, which includes both the quality and the quantity of life lived. It assigns to each period of time a weight, ranging from 0 (equivalent to death) to 1 (optimal health), corresponding to the HRQoL during that periodCitation32.The QALY decrements associated with SREs in the model were derived from a time trade-off (TTO) study conducted in 126 participants from the UK general population, who completed TTO interviews to assess the utility of hypothetical health state vignettes describing patients with cancer with bone metastases and SREsCitation38 (). Changes in QALYs were computed to estimate the decrement associated with each year in which an SRE occurred. The model calculates the expected average QALY decrement of an SRE based on the proportion distribution of each type of SRE (see ‘SRE type distribution’ section of the Methods).
The QALY decrements associated with administration of drugs for SRE prevention were estimated from another TTO study conducted in 121 participants from the UK general population, who were interviewed using hypothetical vignettes describing the health states of patients with cancer with bone metastases not receiving bone metastases treatments, receiving bone metastases treatments involving a less than 10 second SC injection, or receiving bone metastases treatments involving an IV infusion of at least 30 minutes. The mean disutility for receiving monthly SC injections for 1 year was 0.015 and the mean disutility for receiving monthly IV infusions for 1 year was 0.027, resulting in an annual QALY difference of 0.012. This was divided by 13 and applied in each cycle for patients who were on treatment.
The QALY decrements associated with AEs were estimated from EQ-5D data using a generalized estimating equations (GEE) regression approach. Due to the small number of these AEs, the QALY decrements were developed by pooling EQ-5D data from patients across the three trials and both treatment groups. No QALY decrement was assumed for acute phase reactions.
An annual discount rate of 3% was applied to the QALYsCitation32.
Costs
The cost inputs included SRE costs by type, drug costs, administration costs, and AE costs.
SRE costs by type of event and by tumor type were estimated using the reimbursed amount from a large representative US commercial claims databaseCitation9, weighting the inpatient and outpatient costs, and were inflated from 2009 to 2011 costs using the medical component of the Consumer Price Index (CPI)Citation40 (). The model calculates the expected average costs of an SRE based on the proportion distribution of each type of SRE.
Table 3. Costs of skeletal-related events (2011 USD)Citation9.
The 2011 wholesale acquisition cost (WAC) was used for drug costs, with costs of denosumab of $1650 per 120 mg administration and zoledronic acid of $895.61 per administrationCitation41. A $35.42 administration fee for an SC injection of denosumab and a $154.64 administration fee for an IV infusion of zoledronic acid were included for each administration. In addition, a $21.43 renal monitoring fee was also included for each zoledronic acid administrationCitation42.
Due to a lack of data from clinical practice, compliance was assumed to be balanced between the two treatments (10% of doses would be missed for both drugs), consistent with the trial data. In the base case, patients were assumed to continue treatment for their lifetime. Adverse event costs were based on published data, where available (the cost of pyrexia was used for acute phase reactions)Citation30,Citation43. An annual discount rate of 3% was applied to the costsCitation32.
SRE type distribution
The SRE type distributions by tumor type as occur in clinical practice were estimated from published studies of a SEER-Medicare database of patients with prostate, breast, or lung cancer and bone metastasesCitation44,Citation45 ().
Table 4. Real-world skeletal-related event type distributionCitation44,Citation45.
Cost-effectiveness analyses
The outcome measures for the cost-effectiveness analyses included QALY and number of SREs. The ICERs included cost per QALY gained and cost per SRE avoided. The ICER is the ratio of the difference in costs between two alternatives to the difference in effectiveness between the same two alternativesCitation32. Cost per QALY gained is one of the most frequently used ICERs to compare the economic interventions across disease areas. It is also a standard and internationally recognized method to assess the value for money of a medical interventionCitation46.
In this cost-effectiveness analysis, ICERs were obtained by calculating the difference in total cost (ΔC) between denosumab (Cdmab) and zoledronic acid (Czol) and dividing that value by the difference in outcomes (ΔE) between denosumab (Edmab) and zoledronic acid (Ezol)Citation32, where the outcomes are cumulative lifetime QALYs and number of SREs.
The base case analysis used a lifetime time horizon, a 3% per year discount rate for costs and QALYs, and did not incorporate drug discontinuation or AEs. For all three tumor types, two additional scenarios with drug discontinuation and AEs were analyzed.
One-way deterministic and probabilistic sensitivity analyses (PSA) were conducted for key model probability-related, utility-related, and cost-related inputs to test the robustness of the results. In the one-way deterministic sensitivity analyses, plausible values of parameter inputs in the model were varied one at a time and ICERs were re-calculated accordingly. In PSA, probability distributions were specified for each uncertain parameter, and a simulation was performed whereby values of each parameter were randomly drawn from the corresponding distribution, and the resulting probability distribution of expected outcomes was displayedCitation32.
In this cost-effectiveness analysis, individual model variables were intentionally ranged ±50% in one-way deterministic sensitivity analyses to test the robustness of the individual values to large variations. The results are presented in tornado diagrams, where the bars represent the value of ICERs as results of varying the model variables by ±50%. The variable with the largest impact on ICERs appears at the top of the chart, the second largest appears second from the top, and so on. To incorporate the cumulative effect of uncertainty across multiple model inputs, a multivariate PSA was conducted using a Monte Carlo simulation of 1000 iterations for each tumor type. Where possible, the PSA input uncertainties were derived from the confidence intervals, or other measures of uncertainty, available for each parameter (Appendix). The cost-effectiveness acceptability curves (CEACs) for each tumor type were derived to present the probability of denosumab being cost-effective compared with zoledronic acid based on different willingness-to-pay (WTP) thresholds for cost per QALY gained.
Results
Base case
Denosumab was associated with a reduction in the number of SREs compared with zoledronic acid and an improvement in patients’ quality-of-life (thereby increasing QALYs) compared with zoledronic acid across all three tumor types (). Over a patient’s lifetime, the number of SREs avoided per patient taking denosumab was 0.81 for CRPC (median survival = 1.7 years, 56% death in 2 years), 0.99 for breast cancer (median survival = 3.1 years, 34% death in 2 years), and 0.39 for NSCLC (median survival = 9 months, 83% death in 2 years). The lifetime QALYs gained were 0.14 for CRPC, 0.17 for breast cancer, and 0.06 for NSCLC.
Table 5. Cost-effectiveness of denosumab vs zoledronic acid base case results.
The total lifetime incremental costs of denosumab vs zoledronic acid were $6910 for CRPC (incremental drug costs: $18,967; drug administration costs reduction: $3536; SRE costs reduction: $8522), $13,451 for breast cancer (incremental drug costs: $30,431; drug administration costs reduction: $5674; SRE costs reduction: $11,306), and $4076 for NSCLC (incremental drug costs: $10,136; drug administration costs reduction: $1890; SRE costs reduction: $4171). The cost per QALY gained for denosumab compared to zoledronic acid in CRPC, breast cancer, and NSCLC were $49,405, $78,915, and $67,931, respectively. Cost per SRE avoided was $8567, $13,557, and $10,513, respectively ().
Additional scenarios
shows the results for the additional scenarios. When drug discontinuation was considered, the cost per QALY gained for CRPC and NSCLC were reduced to $42,526, and $49,781, respectively, whereas it remained almost constant for breast cancer ().
Table 6. Cost-effectiveness of denosumab vs zoledronic acid scenario analyses results.
The results were not sensitive to the incorporation of ONJ, acute phase reaction, hypocalcemia or renal toxicities (), with the costs per QALY gained and costs per SRE avoided being similar to the base case scenario for each tumor type.
Sensitivity analyses
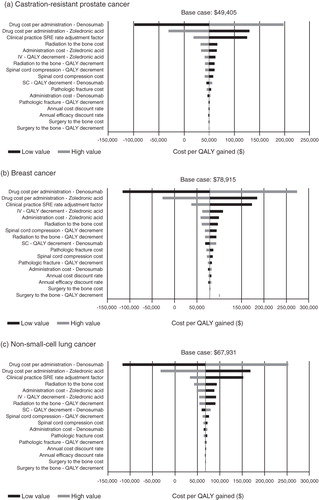
In one-way sensitivity analyses, the most influential variables were drug costs and SRE rates ().
Figure 2. One-way sensitivity analyses of the effect of the input parameters on cost per QALY gained. SRE, skeletal-related events; IV, intravenous; QALY, quality-adjusted life year; SC, subcutaneous.
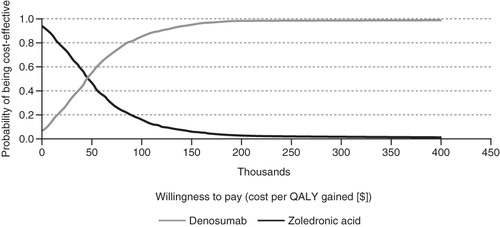
In the multivariate probabilistic sensitivity analysis (PSA), the probabilities of denosumab being cost-effective vs zoledronic acid in patients with CRPC and bone metastases were ∼0.83, 0.94, and 0.98 with ICER thresholds of $100,000, $150,000, and $200,000, respectively (). For patients with breast cancer and bone metastases, the corresponding probabilities were 0.62, 0.79, and 0.91, respectively, and they were 0.60, 0.72, and 0.78 for patients with NSCLC and bone metastases.
Figure 3. Cost-effectiveness acceptability curves (CEACs) of denosumab vs zoledronic acid in the prevention of skeletal-related events in patients with castration-resistant prostate cancer and bone metastases. The curves illustrate the probability of denosumab being cost-effective relative to zoledronic acid and vice-versa based on different thresholds of willingness to pay. The probability of denosumab being cost-effective relative to zoledronic acid increases as the willingness to pay threshold increases. QALY, quality-adjusted life year.
Discussion
Cost-effectiveness analyses help to inform payers and formulary decisions by quantifying the comparative value of treatments. We determined the lifetime cost-effectiveness of denosumab vs zoledronic acid in preventing SREs among patients with CRPC, breast cancer, or NSCLC and bone metastases, from a US managed care perspective.
In the base case analyses, the costs per QALY gained of denosumab vs zoledronic acid were $49,405 for CRPC, $78,915 for breast cancer, and $67,931 for NSCLC, and the corresponding costs per SRE avoided in patients treated with denosumab vs zoledronic acid were $8567, $13,557, and $10,513, respectively. When the rate of drug discontinuation associated with denosumab or zoledronic acid (as reported in the Phase 3 trials) was included in the analyses, cost per QALY gained in CRPC and NSCLC were reduced substantially (to $42,526 and $49,781, respectively), due to the non-trivial difference in this rate, which was higher for zoledronic acid than for denosumabCitation16,Citation34. The results were robust to the incorporation of ONJ, acute phase reactions, hypocalcemia, and renal toxicity across all three tumor types. By assuming no QALY decrement associated with treatment administration, the cost per QALY gained ranged from ∼$60,000–$105,000, which reflects the non-trivial impact of differences in mode of administration on the cost-effectiveness of denosumab vs zoledronic acid. In fact, previous time and motion studies have demonstrated notably increased time burden associated with zoledronic acid infusionsCitation47,Citation48.
It is worth noting that, among all the important inputs, the model results were most sensitive to drug costs and SRE rates. The Phase 3 trials tended to enroll patients with a better performance status (eligibility criteria required all patients to have an Eastern Cooperative Oncology Group [ECOG] performance status ≤2, with more than 80% of patients randomized having an ECOG of 0 or 1) and longer life expectanciesCitation16–18 than patients in the real world setting, such that the trial-based SRE rates were likely to under-estimate the expected SRE rates in clinical practice. From a payer’s perspective, under-estimating real world SRE rates will under-estimate the economic burden of SREs. A previously reported economic evaluation of denosumab vs zoledronic acid in patients with CRPC and bone metastasesCitation30 used SRE rates from the Phase 3 trial of patients with CRPC, and thus is likely to have under-estimated the economic value of denosumab. Given the importance of SRE rates in the model (), we believe that use of an adjusted rate of SREs that reflects clinical practice (as per our analyses) provides a more accurate assessment of the relative value of these treatments to payers.
In addition, the previously published economic evaluation of denosumab vs zoledronic acid in patients with CRPC and bone metastasesCitation30 made several inappropriate assumptions to derive the transition probabilities between Markov health states, which yield downwardly biased estimates of the incidence of SREsCitation31. This evaluation applied 1-year cumulative costs associated with SREs in aggregateCitation49, which is also not justified and leads to under-estimation of the SRE costsCitation31.
Our Markov model was validated against the clinical trial results by comparing the number of SREs predicted by the model with the number of SREs observed from the trials. By setting the clinical practice SRE rate adjustment factor to one, the model predicted almost the same number of SREs as observed from the trials over the same time duration and for the same number of patients, for both treatment groups in each tumor type.
As noted in the methods, the SRE and drug administration QALY decrement inputs in this cost-effectiveness evaluation were based on TTO studies rather than the EQ-5D data from the Phase 3 clinical trials. Although widely used for the assessment of health state utilities, there are known limitations of the EQ-5D such as ceiling effectsCitation50–53, a limited ability to capture mild burdens of morbidity, and a limited ability to reflect small differences in health states that are particularly important to specific groups of patientsCitation53–55. Therefore, it is unlikely that differences among the SRE types would be captured using the five items of EQ-5D (mobility, self-care, usual activities, pain/discomfort, and anxiety/depression), each with only three response options (no problems, some problems, and severe problems). In addition, due to the clinical characteristics of SREs (i.e., as acute events), it has become very challenging to prospectively capture the accurate impact of SREs on QALY within an observational research design. Regarding the impact on QALY of different modes of administrations, due to the double-blinded, double dummy design of the Phase 3 trials of denosumab vs zoledronic acidCitation16–18, the trial-based quality-of-life measures were not designed to be able to capture the different QALY decrements associated with IV infusions (zoledronic acid) vs SC injections (denosumab). Most reimbursement authorities prefer utilities derived from general population values (e.g., National Institute for Health and Clinical Excellence [NICE], Pharmaceutical Benefits Advisory Committee [PBAC]). The general population approach has the theoretical advantage of ensuring that societal values are represented when making decisions about the levels of public funding for medical treatmentCitation54,Citation56. Thus, we believe the SRE and IV vs SC QALY decrements assessed with a time trade-off approach in the general population are appropriate for application in the CEA model.
As with all cost-effectiveness models, these analyses also have limitations. For example, the model does not capture pain management costs, even though the clinical studies have demonstrated a difference in pain severity and analgesic use between the two treatments in favor of denosumabCitation20–22. The inclusion of pain management costs would therefore be anticipated to provide lower costs per QALY gained for denosumab vs zoledronic acid than the current estimates. A further limitation is that, due to the lack of empirical data, the mortality rate beyond the clinical study durations were extrapolated from the generalized gamma functions, which may or may not accurately reflect actual outcomes. However, given that, overall, there was no significant difference in mortality between the two treatment groupsCitation16–18, it is very unlikely that the cost-effectiveness results are biased because of this. As there are limited data on compliance with denosumab in the oncology setting, the current model assumed the same drug compliance rate for both treatment groups. Since denosumab does not require dose adjustment or dose withholding based on renal status and is associated with fewer acute phase reactions compared with zoledronic acidCitation19, compliance with denosumab is expected to be higher than with zoledronic acid in clinical practice. However, further studies are needed to investigate the compliance rates and usage of these two drugs in clinical practice. The SRE costs in patients with NSCLC were assumed to be the average of SRE costs in breast cancer and CRPC. The direction of bias due to this assumption is not clear; however, the model results were robust to the SRE costs. Finally, costs and QALY decrements associated with the AEs, such as ONJ and hypocalcemia, are not well documented in the literature. Although these inputs in this model are very unlikely to bias the results substantially, this suggests the need for further research in costs and patient utilities in this area.
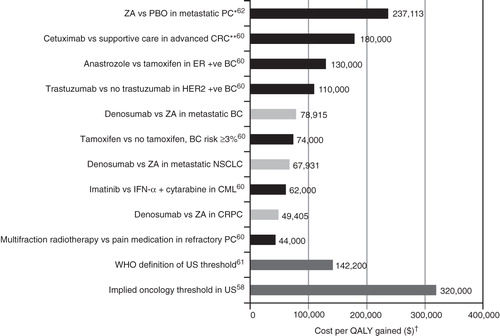
Interpretation of the cost per QALY gained of denosumab vs zoledronic acid leads to the question of what is considered an acceptable ICER threshold in the US healthcare sector, specifically, in US oncology settings. Unlike European countries (UK NICE recommends an ICER threshold of £20,000–£30,000 per QALY gainedCitation46; other European countries generally recommend €50,000), there is no generally accepted cost per QALY gained threshold in the US, and the implied thresholds likely vary by disease area. The recently enacted Patient Protection and Affordable Care Act states: ‘… the Patient Centered Outcomes Research Institute… shall not develop or employ a dollars per quality adjusted life year (or similar measure that discounts the value of a life because of an individual’s disability) as a threshold to establish what type of health care is cost-effective or recommended…’. In addition, although several instances were identified where cost-effectiveness evidence was cited in National Coverage Decisions, no clear evidence was found indicating an implicit threshold from the Centers for Medicare and Medicaid Services (CMS)Citation57. A survey study of US oncologists suggested an average cost per QALY gained threshold of $320,000Citation58. Another simulation model study estimated the value of a statistical year of life implied by dialysis practice at $129,090 per QALYCitation59. However, the costs per QALY gained of denosumab vs zoledronic acid for all the three tumor types from this analysis ($49,405 for CRPC, $78,915 for breast cancer and $67,931 for NSCLC) are within the range of other innovative oncology therapies available on the US market ().
Figure 4. Cost-effectiveness of denosumab vs zoledronic acid relative to other select innovative oncology therapiesCitation58,Citation60–62. *Costs inflated to 2010 using proportional increase in US consumer price index from 2000 to 2010 (http://www.bls.gov/data). **In patients with wild-type KRAS. †Costs in 2010 USD for historical data. ZA, zoledronic acid; PBO, placebo; PC, prostate cancer; CRC, colorectal cancer; ER + ve, estrogen receptor positive; BC, breast cancer; HER2 + ve, HER2-receptor positive; NSCLC, non-small-cell lung cancer; CML, chronic myeloid leukemia; CRPC, castration resistant prostate cancer; WHO, World Health Organization.
Conclusions
In conclusion, from the US managed care perspective, denosumab is cost-effective in preventing SREs in patients with bone metastases secondary to advanced solid tumors compared with zoledronic acid. The overall value of denosumab is based on superior efficacy, a favorable safety profile, and more efficient administration.
Transparency
Declaration of funding
This study was funded by Amgen Inc.
Declaration of financial/other relationships
KC, ZC, RD, and YQ are employees of Amgen Inc. MD and MH received funding from Amgen Inc in order to perform cost-effectiveness analyses. DH has received research funding from Amgen. DH and MR have received consultancy/speaker fees from Amgen. AS has acted as a paid consultant/advisor to Amgen and Novartis.
Supplementary Material
Download PDF (55 KB)Acknowledgments
Editorial assistance was provided by Dr Sue Laing of ApotheCom ScopeMedical Ltd, UK, which was funded by Amgen Inc.
References
- Coleman RE. Bisphosphonates: clinical experience. Oncologist 2004;9(Suppl 4):14-27
- Mundy GR. Metastasis to bone: causes, consequences and therapeutic opportunities. Nat Rev Cancer 2002;2:584-93
- Roodman GD. Mechanisms of bone metastasis. N Engl J Med 2004;350:1655-64
- Coleman RE. Skeletal complications of malignancy. Cancer 1997;80:1588-94
- Coleman RE. Clinical features of metastatic bone disease and risk of skeletal morbidity. Clin Cancer Res 2006;12:6243s-9s
- Weinfurt KP, Li Y, Castel LD, et al. The significance of skeletal-related events for the health-related quality of life of patients with metastatic prostate cancer. Ann Oncol 2005;16:579-84
- Pockett RD, Castellano D, McEwan P et al. The hospital burden of disease associated with bone metastases and skeletal-related events in patients with breast cancer, lung cancer, or prostate cancer in Spain. Eur J Cancer Care (Engl) 2010;19:755-60
- Delea T, McKiernan J, Brandman J, et al. Retrospective study of the effect of skeletal complications on total medical care costs in patients with bone metastases of breast cancer seen in typical clinical practice. J Support Oncol 2006;4:341-7
- Barlev A, Song X, Ivanov B, et al. Payer costs for inpatient treatment of pathologic fracture, surgery to bone, and spinal cord compression among patients with multiple myeloma or bone metastasis secondary to prostate or breast cancer. J Manag Care Pharm 2010;16:693-702
- Hatoum HT, Lin SJ, Smith MR, et al. Zoledronic acid and skeletal complications in patients with solid tumors and bone metastases: analysis of a national medical claims database. Cancer 2008;113:1438-45
- Kohno N, Aogi K, Minami H, et al. Zoledronic acid significantly reduces skeletal complications compared with placebo in Japanese women with bone metastases from breast cancer: a randomized, placebo-controlled trial. J Clin Oncol 2005;23:3314-21
- Rosen LS, Gordon D, Tchekmedyian NS, et al. Long-term efficacy and safety of zoledronic acid in the treatment of skeletal metastases in patients with nonsmall cell lung carcinoma and other solid tumors: a randomized, Phase III, double-blind, placebo-controlled trial. Cancer 2004;100:2613-21
- Saad F, Gleason DM, Murray R, et al. Long-term efficacy of zoledronic acid for the prevention of skeletal complications in patients with metastatic hormone-refractory prostate cancer. J Natl Cancer Inst 2004;96:879-82
- Novartis. Zometa® US Prescribing Information. Novartis, East Hanover, New Jersey, USA, 2011
- Body JJ, Facon T, Coleman RE, et al. A study of the biological receptor activator of nuclear factor-kappaB ligand inhibitor, denosumab, in patients with multiple myeloma or bone metastases from breast cancer. Clin Cancer Res 2006;12:1221-8
- Fizazi K, Carducci M, Smith M, et al. Denosumab versus zoledronic acid for treatment of bone metastases in men with castration-resistant prostate cancer: a randomised, double-blind study. Lancet 2011;377:813-22
- Stopeck AT, Lipton A, Body JJ, et al. Denosumab compared with zoledronic acid for the treatment of bone metastases in patients with advanced breast cancer: a randomized, double-blind study. J Clin Oncol 2010;28:5132-9
- Henry DH, Costa L, Goldwasser F, et al. Randomized, double-blind study of denosumab versus zoledronic acid in the treatment of bone metastases in patients with advanced cancer (excluding breast and prostate cancer) or multiple myeloma. J Clin Oncol 2011;29:1125-32
- Lipton A, Siena S, Rader M, et al. Comparison of denosumab versus zoledronic acid (ZA) for treatment of bone metastases in advanced cancer patients: an integrated analysis of 3 pivotal trials. Ann Oncol 2011;21:viii380, Abstract 1249P
- von Moos R, Patrick D, Fallowfield L. Effects of denosumab versus zoledronic acid (ZA) on pain in patients (pts) with advanced cancer (excluding breast and prostate) or multiple myeloma (MM): results from a randomized phase III clinical trial. J Clin Oncol 2010;18(suppl), Abstract 9043
- Stopeck AT, Fallowfield L, Patrick D. Effects of denosumab versus zoledronic acid (ZA) on pain in patients (pts) with metastatic breast cancer: results from a phase III clinical trial. J Clin Oncol 2010;28(suppl), Abstract 1024
- Patrick D, Fallowfield L, Cleeland C. Effects of denosumab versus zoledronic acid on pain in patients with metastatic breast cancer: results from a randomized, double-blind, double-dummy phase 3 trial. Multinational Association of Supportive Care in Cancer Meeting, Vancouver, Canada, 2010. Abstract 274
- Fallowfield L, Patrick D, Body JJ. The effect of treatment with denosumab or zoledronic acid on health-related quality of life in patients with metastatic breast cancer. San Antonio, TX: Breast Cancer Symposium, 2010. Abstract P1-13-05
- Fallowfield L, Patrick D, Body JJ. Effect of denosumab versus zoledronic acid on health-related quality of life in patients with metastatic breast cancer. J Clin Oncol 2011;29(27 Suppl), Abstract 272
- Amgen Inc. Xgeva® US Prescribing Information. Amgen Inc, Thousand Oaks, CA, USA, 2010
- OECD Health Data 2011 Frequently Requested Data. Available at: http://www.oecd.org/document/16/0,3746,en_2649_37407_2085200_1_1_1_37407,00.html. Accessed July 2011
- Annemans L, Cleemput I, Simoens S. The increasing role of health economic evaluations in drug development. Drug Dev Res 2010;71:457-62
- Coleman RE. Prostate cancer: targeted therapy for prostate cancer metastases to bone. Nat Rev Urol 2011;8:296-8
- West H. Denosumab for prevention of skeletal-related events in patients with bone metastases from solid tumors: incremental benefit, debatable value. J Clin Oncol 2011;29:1095-8
- Xie J, Namjoshi M, Wu EQ, et al. Economic evaluation of denosumab compared with zoledronic acid in hormone-refractory prostate cancer patients with bone metastases. J Manag Care Pharm 2011;17:621-43
- Rader M, Goessl C, Cong Z. Economic evaluation of denosumab compared with zoledronic acid in hormone-refractory prostate cancer patients with bone metastases. J Manag Care Pharm 2012;18:74-6
- Gold MR, Siegel JE, Russell LB. Cost-effectiveness in health and medicine. New York: Oxford University Press, 1996
- Botteman M, Barghout V, Stephens J, et al. Cost effectiveness of bisphosphonates in the management of breast cancer patients with bone metastases. Ann Oncol 2006;17:1072-82
- Scagliotti G, Hirsch V, Siena S, et al. Overall survival improvement in patients with lung cancer treated with denosumab versus zoledronic acid: results from a randomized phase 3 study. 14th World Conference on Lung Cancer, Amsterdam, The Netherlands, 2011. Abstract and oral presentation O01.01
- McKeage K, Plosker GL. Zoledronic acid: a pharmacoeconomic review of its use in the management of bone metastases. Pharmacoeconomics 2008;26:251-68
- Pavlakis N, Schmidt R, Stockler M. Bisphosphonates for breast cancer. Cochrane Database Syst Rev 2005;CD003474
- Saad F. Zoledronic acid significantly reduces pathologic fractures in patients with advanced-stage prostate cancer metastatic to bone. Clin Prostate Cancer 2002;1:145-52
- Matza LS, Van Brunt K, Chung K. Health state utilities for skeletal-related events associated with bone metastases. J Clin Oncol 2011;19(suppl), Abstract e16620
- Levack P, Collie D, Gibson A, et al. A prospective audit of the diagnosis, management and outcome of malignant cord compression. CRAG Report 97/08. Edinburgh: CRAG, 2001
- United States Department of Labor. Bureau of Labor Statistics. Consumer Price Index - All Urban Consumers. US City Average, Medical Care, 12-month percent change July 2009 to July 2011. http://www.bls.gov/data. Accessed December 2011
- Analysource. Analysource Online. http://www.analysource.com. Accessed July 2011
- Ingenix. National Fee Analyzer. 50th Percentile data for CPT codes 96365 and 96372. Ingenix, Minnesota, USA, 2011
- Bell JM, Miller JD, Namjoshi M, et al. Comparative budget impact of formulary inclusion of zoledronic acid and densoumab for prevention of skeletal-related events in patients with bone metastases. Value Health 2011;14:A159
- Sathiakumar N, Delzell E, Morrisey MA, et al. Mortality following bone metastasis and skeletal-related events among women with breast cancer: a population-based analysis of U.S. Medicare beneficiaries, 1999-2006. Breast Cancer Res Treat 2012;131:231-8
- Sathiakumar N, Delzell E, Morrisey MA, et al. Mortality following bone metastasis and skeletal-related events among men with prostate cancer: a population-based analysis of US Medicare beneficiaries, 1999-2006. Prostate Cancer Prostatic Dis 2011;14:177-83
- NICE. Measuring effectiveness and cost effectiveness: the QALY. http://www.nice.org.uk/newsroom/features/measuringeffectivenessandcosteffectivenesstheqaly.jsp. Last updated April 2010, Accessed December 2011
- DesHarnais Castel L, Bajwa K, Markle JP, et al. A microcosting analysis of zoledronic acid and pamidronate therapy in patients with metastatic bone disease. Support Care Cancer 2001;9:545-51
- Oglesby A, Sherif B, Odom D. Time and costs associated with preparing and administering zoledronic acid in patients with breast or prostate cancer and metastatic bone disease. Commun Oncol 2009;6:494-505
- Lage MJ, Barber BL, Harrison DJ, et al. The cost of treating skeletal-related events in patients with prostate cancer. Am J Manag Care 2008;14:317-22
- Brazier J, Roberts J, Tsuchiya A, et al. A comparison of the EQ-5D and SF-6D across seven patient groups. Health Econ 2004;13:873-84
- Brazier J, Jones N, Kind P. Testing the validity of the Euroqol and comparing it with the SF-36 health survey questionnaire. Qual Life Res 1993;2:169-80
- Hinz A, Klaiberg A, Brahler E, et al. [The Quality of Life Questionnaire EQ-5D: modelling and norm values for the general population]. Psychother Psychosom Med Psychol 2006;56:42-8
- Kaarlola A, Pettila V, Kekki P. Performance of two measures of general health-related quality of life, the EQ-5D and the RAND-36 among critically ill patients. Intensive Care Med 2004;30:2245-52
- Stein K, Fry A, Round A, et al. What value health?: a review of health state values used in early technology assessments for NICE. Appl Health Econ Health Policy 2005;4:219-28
- Torrance GW, Furlong W, Feeny D. Health utility estimation. Expert Rev Pharmacoecon Outcomes Res 2002;2:99-108
- Brazier J. Valuing health states for its use in cost-effectiveness analysis. Pharmacoeconomics 2008;26:769-79
- Chambers JD, Neumann PJ, Buxton MJ. Does Medicare have an implicit cost-effectiveness threshold? Med Decis Making 2010;30:E14-E27
- Nadler E, Eckert B, Neumann PJ. Do oncologists believe new cancer drugs offer good value? Oncologist 2006;11:90-5
- Lee CP, Chertow GM, Zenios SA. An empiric estimate of the value of life: updating the renal dialysis cost-effectiveness standard. Value Health 2009;12:80-7
- Center for the Evaluation of Risk in Health. The Cost-effectiveness Registry. Institute for Clinical Research and Health Policy Studies, Tufts Medical Center, Boston, MA, USA, 2011
- Edejer T, editor. Making choices in health: WHO guide to cost-effectiveness analysis. Geneva: WHO, 2003
- Reed SD, Radeva JI, Glendenning GA, et al. Cost-effectiveness of zoledronic acid for the prevention of skeletal complications in patients with prostate cancer. J Urol 2004;171:1537–42