
Abstract
Objective:
The randomized clinical trials, RE-LY, ROCKET-AF, and ARISTOTLE, demonstrate that the novel oral anticoagulants (NOACs) are effective options for stroke prevention among non-valvular atrial fibrillation (AF) patients. This study aimed to evaluate the medical cost reductions associated with the use of individual NOACs instead of warfarin from the US payer perspective.
Methods:
Rates for efficacy and safety clinical events for warfarin were estimated as the weighted averages from the RE-LY, ROCKET-AF and ARISTOTLE trials, and event rates for NOACs were determined by applying trial hazard ratios or relative risk ratios to such weighted averages. Incremental medical costs to a US health payer of an AF patient experiencing a clinical event during 1 year following the event were obtained from published literature and inflation adjusted to 2010 cost levels. Medical costs, excluding drug costs, were evaluated and compared for each NOAC vs warfarin. Sensitivity analyses were conducted to determine the influence of variations in clinical event rates and incremental costs on the medical cost reduction.
Results:
In a patient year, the medical cost reduction associated with NOAC usage instead of warfarin was estimated to be −$179, −$89, and −$485 for dabigatran, rivaroxaban, and apixaban, respectively. When clinical event rates and costs were allowed to vary simultaneously, through a Monte Carlo simulation, the 95% confidence interval of annual medical costs differences ranged between −$424 and +$71 for dabigatran, −$301 and +$135 for rivaroxaban, and −$741 and −$252 for apixaban, with a negative number indicating a cost reduction. Of the 10,000 Monte-Carlo iterations 92.6%, 79.8%, and 100.0% were associated with a medical cost reduction >$0 for dabigatran, rivaroxaban, and apixaban, respectively.
Conclusions:
Usage of the NOACs, dabigatran, rivaroxaban, and apixaban may be associated with lower medical (excluding drug costs) costs relative to warfarin, with apixaban having the most substantial medical cost reduction.
Introduction
Atrial fibrillation (AF) is the most common significant cardiac rhythm disorder, affecting ∼5 million people in the US and independently increasing the risk of ischemic stroke 5-foldCitation1,Citation2. Stroke was the fourth leading cause of death in 2008 in the US and remains a leading cause of serious long-term disabilityCitation3. With AF-related strokes accounting for between 6–24% of ischemic strokesCitation4,Citation5 and a total US healthcare cost of all strokes of $53.9 billion in 2010, AF-related strokes are estimated to have had an economic burden from $3.2 billion to nearly $13 billion in 2010Citation6. Several risk factors contribute to AF-related stroke occurrence with age being a predominant factorCitation7,Citation8. With the growing elderly population in the US, the prevalence of AF is expected to double or possibly triple by 2050Citation2,Citation9. Future projections estimate the US economic burden of AF in 2050 at ∼$30 billionCitation10.
The principal anticoagulant used to manage stroke risk in AF patients for decades has been warfarin. Warfarin is a broad spectrum anticoagulant that inhibits the synthesis of multiple factors in the clotting cascade and is effective in decreasing stroke risk and reducing mortality in AF patients as long as it is kept in a proper therapeutic rangeCitation7,Citation11. The therapeutic range, as monitored by international normalized ratio (INR), however, is narrow, and patients on warfarin must be regularly monitored via blood testing. Additional complications of warfarin arise because of multiple drug–drug interactions and drug–nutrient interactions which result in out of control INRs.
Randomized clinical trials have demonstrated that several new anticoagulant pharmacotherapies, referred to as Novel Oral Anticoagulants (NOACs), are effective alternatives to warfarin for stroke prophylaxis in AF patientsCitation12–14. These include dabigatran, a direct thrombin inhibitor, and rivaroxaban and apixaban, both of which directly inhibit factor Xa in the coagulation cascade without using antithrombin as a mediator.
The efficacy and safety of dabigatran was demonstrated in the Randomized Evaluation of Long-Term Anticoagulation Therapy (RE-LY) trialCitation12. In this open-labeled trial, dabigatran, at a dose of 110 mg twice daily, was shown to be comparable to warfarin in efficacy for reducing stroke risk, and demonstrated a reduction in major bleeding events. At a dose of 150 mg twice daily, dabigatran was associated with lower rates of stroke and systemic embolism, but similar rates of major hemorrhage in comparison to warfarin. In the US, currently, dabigatran is approved for stroke prophylaxis in AF patients at a dose of 150 mg twice daily and for those with severe renal impairment at a dose of 75 mg twice daily.
The efficacy and safety of rivaroxaban was demonstrated in the randomized, double-blind Rivaroxaban Once Daily Oral Direct Factor Xa Inhibition Compared with Vitamin K Antagonism for Prevention of Stroke and Embolism Trial in Atrial Fibrillation (ROCKET-AF)Citation13. In patients with AF, rivaroxaban, at a dose of 20 mg once daily, was similar in efficacy relative to warfarin for the prevention of stroke or systemic embolism, and there was no significant difference in the risk of major bleeding. In the US, currently, rivaroxaban is approved for stroke prophylaxis in AF patients at a dose of 20 mg once daily.
The efficacy and safety of apixaban was demonstrated in the Apixaban for Reduction in Stroke and Other Thromboembolic Events in Atrial Fibrillation (ARISTOTLE) trialCitation14. In this randomized, double-blind trial, apixaban, at a dose of 5 mg twice daily, was shown to be superior to warfarin in preventing stroke or systemic embolism in patients with AF. Additionally, patients treated with apixaban had a significantly reduced risk for major bleeding events in comparison to patients treated with warfarin.
The reduction in clinical events associated with NOACs may impact the medical costs of AF patients, although it is unclear whether there will be differences among the NOACs in this regard. Alongside improving healthcare access and quality, the reduction of medical costs is a priority of healthcare reform and evaluation of whether certain therapeutic interventions are associated with reductions in medical costs are important to consider, as those that do demonstrate a relative medical cost reduction have the potential to improve healthcare delivery while controlling cost. This study aimed to evaluate from a US payer perspective the medical cost reductions associated with the use of individual NOACs instead of warfarin based on data from clinical trials.
Methods
Estimation of clinical event rates
The relative risks of clinical events, expressed as either hazard ratios or relative risk ratios, associated with NOACs were taken directly from each original trial publication. The clinical events evaluated included ischemic or uncertain type of stroke (IS), hemorrhagic stroke (HS), systemic embolism (SE), myocardial infarction (MI), pulmonary embolism (PE) or deep vein thrombosis (DVT), major bleedings excluding hemorrhagic stroke (MBEHS), clinically relevant non-major bleeding, and other minor bleeding events. HS was considered both as an efficacy end-point and a safety end-point in the NOAC vs warfarin clinical trials. In order to avoid double counting, HS events in this cost analysis were excluded from major bleeding, but kept as a component of efficacy end-points. When the relative risk of a particular clinical event was not reported in a clinical trial, the relative risk of an end-point containing this clinical event was used. For example, the relative risk of SE was not reported in the RE-LY trial, and for the purpose of this study it was assumed to be equal to the reported relative risk of stroke and/or SECitation12.
For warfarin, the rates of clinical events were estimated as the averages, weighted by patient sample size from the RE-LY, ROCKET-AF, and ARISTOTLE trialsCitation12–14. This approach reflects that, from a US drug indication perspective, all three NOACs are likely to be used in the same real-world AF population despite different clinical trial designs and risk profiles of clinical trial populations. For example, dabigatran and rivaroxaban are both approved for stroke prophylaxis in AF patients in the US despite differences in their corresponding trial designsCitation15,Citation16. The absolute risk of events, i.e., the clinical event rate, associated with each NOAC, was derived by applying the estimated relative risks to the weighted averages of warfarin event rates. In this study, we did not evaluate the medical cost avoidance related to dabigatran 75 mg dose once daily since the clinical event rates for such dosage were not reported in the RE-LY trialCitation12.
Estimation of medical cost reductions
Values for incremental medical costs, defined as the incremental costs to a US health payer of an AF patient experiencing a clinical event during 1 year following the event were obtained from published literature or based on input from clinical experts when such literature was not available. The cost of a clinically relevant non-major bleeding event was assumed to be the cost of four office visits and the cost of a minor bleeding event was assumed to be the cost of one office visitCitation17. The medical costs of clinical events were inflation adjusted to 2010 cost levels via the CPI Medical Care IndexCitation18. Based on the absolute risks determined for each of the clinical events, the reduction in total medical costs associated with each NOAC vs warfarin was determined. Our study focuses on the medical cost reduction driven by clinical outcomes, with drug costs and other additional monitoring-related expenses not included in this analysis.
Sensitivity analyses
Univariate sensitivity analyses were conducted to determine the effects of varying a single clinical event rate or the corresponding incremental cost on the medical cost reductions associated with NOAC vs warfarin usage. Clinical event rates were varied between the ranges of their respective 95% confidence intervals and the incremental cost estimates were varied ±30%. Since these variables are often interdependent, a Monte Carlo analysis was also performed as multivariate sensitivity analysis with Gaussian distributions assumed for the estimates of clinical event rates and the corresponding cost estimates. For each cycle of the Monte Carlo analysis, the value of the clinical event rates was taken randomly from a Gaussian distribution of the mean and standard deviation of the corresponding variables, and the value of the corresponding incremental cost taken randomly from a Gaussian distribution of the corresponding mean with a coefficient of variation of 0.30. Ten thousand such iterations were conducted for each NOAC vs warfarin comparison. Descriptive statistics of the total cost reductions were measured from the results of 10,000 random Monte-Carlo cycles. The 95% confidence intervals of the mean medical cost reduction were evaluated as the range between the 2.5 and 97.5 percentile of medical costs evaluated from the 10,000 random cycles of Monte-Carlo simulation for each NOAC vs warfarin comparison.
Results
Relative risks for efficacy and safety end-points
Based on the published results of clinical trials for each NOAC, the estimated relative risks (95% confidence interval) for key study end-points were 0.76 (0.60 –0.98), 0.94 (0.75–1.17), and 0.92 (0.74–1.13) for IS, and 0.93 (0.81–1.07), 1.04 (0.90–1.20), and 0.69 (0.60–0.80) for MBEHS for dabigatran, rivaroxaban, and apixaban, respectively, relative to warfarin (). The relative risks for the other evaluated clinical events are reported in .
Table 1. Relative risks for efficacy and safety end-points associated with warfarin and novel oral anticoagulants (NOACs).
Absolute risks for efficacy and safety end-points
Based on the combined results of the three clinical trials, the per patient year event rates of key clinical events for warfarin treatment were estimated at 1.24% for IS, and 2.88% for MBEHS (). When the NOAC relative risks were applied to these estimated warfarin rates, the estimated event rates were 0.94%, 1.17%, and 1.14% for IS, and 2.97%, 3.20%, and 2.07% for MBEHS for dabigatran, rivaroxaban and apixaban, respectively (). The estimated event rates for the other evaluated clinical events are reported in .
Table 2. Estimated absolute risks for efficacy and safety end-points associated with warfarin and novel oral anticoagulants (NOACs).
Medical cost reductions
Based on previously published literature, the incremental 1-year medical costs of patients with clinical end-points relative to patients who did not have a clinical event in 2010 dollars were estimated as the following: IS = $39,511, HS = $51,659, SE = $19,756, MI = $37,446, PE/DVT = $19,532, and MBEHS = $34,617 (). In a year, the total medical cost reductions associated with NOAC usage instead of warfarin were estimated to be −$179, −$89, and −$485 for dabigatran, rivaroxaban, and apixaban, respectively ().
Table 3. Incremental 1-year healthcare costs of patients with clinical end-points.
Table 4. Medical costs and differences associated with usage of novel oral anticoagulants (NOACs) in comparison to warfarin*.
For dabigatran, cost avoidance was mainly associated with reductions in the cost of HS (−$167) and IS (−$118), but dabigatran usage was associated with increased costs of MI (+$79) and MBEHS (+$31). For rivaroxaban, cost avoidance was mainly associated with reductions in the cost of HS (−$92) and MI (−$56), but rivaroxaban usage was associated with increased costs of MBEHS (+$108). For apixaban, cost avoidance was mainly associated with reductions in the cost of MBEHS (−$282) and HS (−$110), with smaller contributions from the cost of IS (−$39) and MI (−$35).
Sensitivity analyses
Univariate and multivariate sensitivity analysis demonstrated consistent medical cost reductions associated with NOAC usage relative to warfarin. indicates how variations in clinical event rates influenced the estimated cost reductions of NOACs. The clinical event rates with major impact on the estimated cost reductions associated with dabigatran usage instead of warfarin were MBEHS, MI, and IS, with the corresponding medical cost difference ranges of (−$299, −$53), (−$275, −$50), and (−$257, −$71), with negative numbers indicating a cost reduction. The clinical event rates with major impact on the estimated cost reductions associated with rivaroxaban usage instead of warfarin were MBEHS, IS, HS, and MI, with the corresponding medical cost difference ranges of (−$216, +$44), (−$182, +$24), (−$138, −$12), and (−$16, −$141). The clinical event rates with major impact on the estimated cost reductions associated with apixaban usage instead of warfarin were IS, MBEHS, and MI, with the corresponding medical cost difference ranges of (−$573, −$382), (−$564, −$395), and (−$549, −$400).
Figure 1. Univariate Sensitivity Analyses Examining the Influence of Variations in (a) Clinical Event Rates and (b) Incremental Costs on the Medical Cost Reduction of Novel Oral Anticoagulant (NOAC) Usage Relative to Warfarin. IS: ischemic or uncertain type of stroke, HS: hemorrhagic stroke, SE: systemic embolism, MI: myocardial infarction, MBEHS: major bleedings excluding hemorrhagic stroke CRNB: clinically relevant non-major bleeding and Minor bleeds: other minor bleeding events.
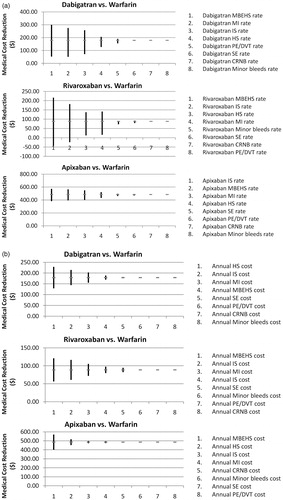
shows how variations in the incremental medical costs of AF patients with events influenced the estimated cost reductions associated with NOACs. The incremental medical costs with major impact on the estimated cost reductions associated with dabigatran usage instead of warfarin were HS (−$229, −$129), IS (−$214, −$144), and MI (−$203, −$155). The incremental medical costs with major impacts on the estimated cost reductions associated with rivaroxaban usage instead of warfarin were MBEHS (−$121, −$56), HS (−$116, −$61), and MI (−$105, −$72). The incremental medical costs with major impacts on the estimated cost reductions associated with apixaban usage instead of warfarin were MBEHS (−$570, −$400) and HS (−$518, −$452).
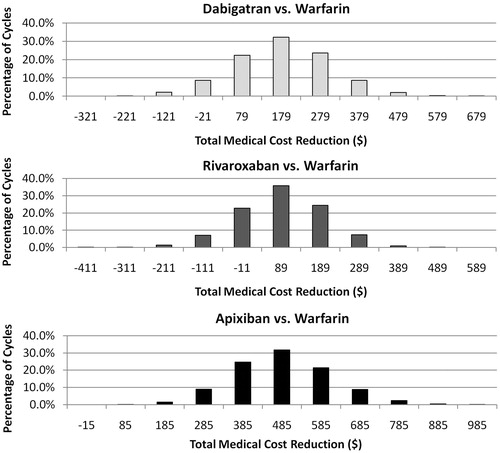
The Monte-Carlo multivariate analysis, in which each variable of the univariate analysis was allowed to vary simultaneously for 10,000 cycles, was used to further test the consistency of the medical cost reduction estimates for NOACs in comparison to warfarin (). The means of medical cost reductions (with 95% confidence interval) associated with NOACs were as follows: dabigatran (−$180); (95% CI, +$71 to − $424), rivaroxaban (−$89); (95% CI, +$135 to −$301), and apixaban (−$485); (95% CI, −$252 to −$741). Of the 10,000 random Monte-Carlo simulation cycles, 92.6%, 79.8%, and 100.0% had a cost reduction >$0 for dabigatran, rivaroxaban, and apixaban, respectively.
Figure 2. Distribution of Total Medical Cost Reductions from 10,000 Cycles of Monte Carlo Simulation (Novel Oral Anticoagulants - NOACs vs. Warfarin).
Discussion
Based on our economic analysis of the three clinical trials, 1-year medical costs were estimated to be lower for AF patients taking a NOAC vs warfarin. In particular, the medical cost reductions in a patient year associated with dabigatran, rivaroxaban, and apixaban were −$179, −$89, and −$485, respectively. Our cost comparison was done within a 1-year time frame as among the three NOAC vs warfarin trials, the median duration of follow-up ranged between 1.6–2.0 years and an annual perspective is a commonly used time-frame by US payers to assess the cost consequence of new therapies. The estimated medical cost reductions associated with NOAC usage, relative to warfarin, can be helpful in determining the overall cost impacts of the usage of NOACs for the growing population of AF patients in the US.
Our economic analysis was based on clinical trial data and therefore the direct application of the results to the real-world setting, where many factors including local healthcare cost, drug adherence, population risk, and health behaviors may vary, will require further assessment. However, prior to the broad exposure of NOACs to the real world, clinical trial results are considered the best basis for conducting this type of researchCitation19,Citation20. Our study results are consistent under additionally evaluated scenarios, such as when the median costs instead of mean costs of incremental medical costs of AF patients with clinical events were used in the analysis, as well as when the clinical event rates of warfarin were taken separately from each original NOAC trial instead of estimated as the weighted average. These scenarios in addition to the sensitivity analyses were put in place to reflect the variety of the real-world settings and demonstrated the consistency of the study results.
The current American College of Cardiology/American Heart Association/European Society of Cardiology (ACC/AHA/ESC) guidelines recommend oral anticoagulation therapy, with a vitamin K antagonist or dabigatran for AF patients and patients with atrial flutter who have more than one moderate risk factor for stroke, such as age ≥75, hypertension, moderately or severely impaired left ventricular systolic function, heart failure, and diabetesCitation7.This group of patients comprises ∼90% of the AF populationCitation21,Citation22. Although anticoagulation therapy is recommended for the majority of the AF population, it is under-utilized for various reasons, including the frequent monitoring of blood concentrations, wide variation in warfarin pharmacokinetics across the AF population, and increased risk of bleeding associated with warfarin usage. A retrospective database analysis evaluating 171,393 patients in the real world reported that, even among AF patients with high stroke risk, only 42.1% were prescribed warfarinCitation23. The low compliance in clinical practice with the recommended guidelines occurs despite the fact that the net clinical benefit of anticoagulation therapy outweighs the risk for the vast majority of AF patientsCitation24. In clinical trials, NOACs were demonstrated to have comparable or better efficacy and safety than warfarin in AF patients. They also have another clear advantage over warfarin in that they have a predictable pharmacological response with no need for frequent, long-term laboratory testing or dose titration.
In the real-world setting, stroke incidence has been observed to be higher among AF patients than reported in clinical trials, although this requires further study, especially among different racial groups and those at higher risk for stroke, such as patients with type 2 diabetes. For example, Wolf et al.Citation25 reported an incidence of stroke of 4.5% among AF patients, who were not administered anticoagulation therapy. A real-world analysis conducted in the US on 119,764 Medicare patients with AF (mean age = 79.3 years) reported an incidence of ischemic stroke of 3.9% per patient per year and that warfarin usage was associated with a 27% reduction in this incidenceCitation26. The results of the study by Mercaldi et al.Citation26 suggest the incidence of ischemic stroke (2.9%) may be greater among AF patients treated with warfarin in the real world than observed in clinical trial AF patients using warfarin (1.2%)Citation12–14.
The efficacy of warfarin for stroke prophylaxis in the real worldCitation26, which is about half that observed in clinical trials, is likely the result of several factors including a wide range of drug–drug and drug–food interactions, low treatment adherence of warfarin, and fluctuation of time in therapeutic range. As none of these factors, nor the associated costs of warfarin monitoring and dose adjustments were taken into account in our study, the medical cost reductions associated with NOAC usage relative to warfarin treatment may be much more substantial when examined in the real world, although again further study is required in this regard.
The fact that warfarin usage increases the risk for major bleeding events is of great concern, especially among AF patients with a high risk of bleeding in the first place. The average absolute risk for major bleeding events in clinical trial patients using warfarin was ∼2.8%Citation12–14. In the real world major bleeding events can be higher, and exceptionally so in patients with greater comorbidities, and in those not serviced by anticoagulation clinicsCitation27,Citation28. A retrospective database study reported that, of 9186 AF patients with CHADS2 scores of 0–1, 2, and 3–6, annual major bleeding event rates were 2.26%, 3.11%, and 4.42%, respectivelyCitation27. Annual rates of major bleeds have been reported to be substantially greater in routine medical clinics, averaging 10.9% in comparison to anticoagulation clinics, which average 2.8%Citation28. The probable increased risk for major bleeds in the real world may imply that NOACs with lower bleeding risk may fare even better in the real world, where warfarin’s time in therapeutic range is frequently lowerCitation29.
Generic warfarin in comparison to NOACs is less expensive when only drug costs are taken into account. However, to assist clinicians and health policy-makers in determining a cost-effective pharmacotherapy for stroke prevention in AF, apart from drug costs, it is important to consider whether certain medical costs are avoided with new therapies in comparison to the standard therapy. Additionally, when cost-effective analyses consider treatment costs along with outcome costs, the cost and frequency of monitoring and dose adjustment and its relationship to clinical outcomes on warfarin should be appropriately incorporated within the context of the clinical data from the randomized control trials. At the time of completing this analysis, only the cost-effectiveness of dabigatran, which has been on the market for longer than a year, has been evaluated in hypothetical real-world AF populations. The cost-effectiveness analyses of dabigatran, which have been published to dateCitation30–33, consistently reported that dabigatran, despite its higher drug cost, is cost-effective relative to warfarin for stroke prevention in real world AF populations.
Limitations
In this study, costs of delivering stroke risk reduction, including drug costs, office visit, and laboratory monitoring costs for warfarin were not taken into account. While drug costs would be higher for NOACs relative to warfarin, inclusion of costs for dose adjustment and routine monitoring would further increase the medical cost reduction with NOACs relative to warfarin. Due to the relationship between frequency of warfarin monitoring, quality of INR control, and rates of clinical outcomes, further studies are needed to incorporate the costs of treatment, inclusive of drug costs and monitoring, into the medical costs of outcomes. The two NOACs, dabigatran and rivaroxaban, in the US market are priced higher than warfarin. At the time of this analysis, apixaban has not yet been approved by the FDA in the US and the drug price has not been established. Other limitations to this study and warranting further analysis among the AF population are the long-term burden of clinical events, indirect costs, and quality-of-life, all of which may be impacted by more efficacious pharmacotherapies for stroke prophylaxis or reduction of major bleeds. As mentioned above, major bleed rates may be greater in the real world and our cost estimates may have under-estimated the medical cost reductions, especially in the case of apixaban in the real-world setting. Another limitation of this cost analysis is that when the relative risk of a particular clinical event was not reported in a clinical trial, the relative risk of an end-point containing this clinical event was used. For example, the relative risk of SE was not reported in the RE-LY trial, and for the purpose of this study it was assumed to be equal to the reported relative risk of stroke and/or SECitation12. Finally, due to a substantial overlap between patients with clinical events (e.g., stroke, major bleeds) and patient deaths, patient death was not included in our cost analysis. This may have led to an under-estimation of the benefits of NOACs vs warfarin.
Conclusion
Based on the data from three NOAC clinical trials, usage of the NOACs, dabigatran, rivaroxaban, and apixaban may be associated with a reduction in medical costs when used instead of warfarin. Apixaban usage may potentially be associated with the most substantial medical cost reduction, as its cost reduction is mainly driven by significant reductions in the risks for both stroke and major bleeding events.
Transparency
Declaration of funding
This research was supported by Bristol-Myers Squibb and Pfizer.
Declaration of financial/other relationships
Yonghua Jing, Dinara Makenbaeva, and John Graham are employees of Bristol-Myers Squibb and own stock in the company. Daniel Wiederkehr is an employee of Pfizer and owns stock in the company. Jay Lin is an employee of Novosys Health, which has received research funds from Bristol-Myers Squibb and Pfizer in connection with conducting this study and development of this manuscript. Steve Deitelzweig and Alpesh Amin are paid consultants for Novosys Health in connection with conducting this study.
Acknowledgments
We would like to acknowledge Melissa-Lingohr Smith from Novosys Health for the editorial support and review of this manuscript. This support was funded by Bristol-Myers Squibb and Pfizer.
References
- Miyasaka Y, Barnes ME, Gersh BJ, et al. Secular trends in incidence of atrial fibrillation in Olmsted County, Minnesota, 1980 to 2000, and implications on the projections for future prevalence. Circulation 2006;114:119-25
- Go AS, Hylek EM, Phillips KA, et al. Prevalence of diagnosed atrial fibrillation in adults: national implications for rhythm management and stroke prevention: the AnTicoagulation and Risk Factors in Atrial Fibrillation (ATRIA) Study. JAMA 2001;285:2370-5
- Miniño BAM, Murphy SL, Jiaquan X, et al. Deaths: final data for 2008. Natl Vital Stat Rep 2011;59:1-157
- Miyazaki S, Ito T, Suwa M, et al. Role of transesophageal echocardiography in the prediction of thromboembolism in patients with chronic nonvalvular atrial fibrillation. Jpn Circ J 2001;65:874-8
- CET Force. Cardiogenic brain embolism. The second report of the Cerebral Embolism Task Force. Arch Neurol 1989;46:727-43
- Heidenreich PA, Trogdon JG, Khavjou OA, et al. Forecasting the future of cardiovascular disease in the United States: a policy statement from the American Heart Association. Circulation 2011;123:933-44
- Fuster V, Rydén LE, Cannom DS, et al. ACC/AHA/ESC 2006 Guidelines for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the European Society of Cardiology Committee for Practice. Circ 2006;114:e257-354
- Heeringa J, van der Kuip DAM, Hofman A, et al. Prevalence, incidence and lifetime risk of atrial fibrillation: the Rotterdam study. Eur H J 2006;27:949-53
- Naccarelli GV, Varker H, Lin J, et al. Increasing prevalence of atrial fibrillation and flutter in the United States. Am J Cardiol 2009;104:1534-9
- Kim MH, Lin J, Hussein M, et al. Cost of atrial fibrillation in United States managed care organizations. Adv Ther 2009;26:847-57
- Atrial Fibrillation Investigators. Risk factors for stroke and efficacy of antithrombotic therapy in atrial fibrillation. Analysis of pooled data from five randomized controlled trials. Arch Intern Med 1994;154:1449-57
- Connolly SJ, Ezekowitz MD, Yusuf S, et al. Dabigatran versus warfarin in patients with atrial fibrillation. New Engl J Med 2009;361:1139-51
- Patel MR, Mahaffey KW, Garg J, et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. New Engl J Med 2011;365:883-91
- Granger CB, Alexander JH, McMurray JJV, et al. Apixaban versus warfarin in patients with atrial fibrillation. New Engl J Med 2011;365:981-2
- Boehringer Ingelheim Pharmaceuticals, Inc. Highlights of Prescribing Information. PRADAXA® (dabigatran etexilate mesylate) capsules for oral use. Initial U.S. Approval: 2010. Ridgefield, Connecticut; 2011
- Janssen Pharmaceuticals, Inc. Highlights of Prescribing Information. XARELTO (rivaroxaban) film-coated oral tablets. Initial U.S. Approval: 2011. Titusville, NJ; 2011
- Centers for Medicare and Medicaid Services. Medicare Fee Schedule, Payment and Reimbursement Benefit Guideline, CPT Code Billing. 2010. http://www.medicarepaymentandreimbursement.com/2010/05/medicare-payment-for-e-m-code-99201.html. Accessed January 11, 2012
- Consumer Price Index December 2010. USDL-11-0018. Bureau of Labor Statistics US Department of Labor. http://www.bls.gov/news.release/archives/cpi_01142011.pdf. Accessed January 11, 2012
- Chiong JR, Kim S, Lin J, et al. Evaluation of costs associated with Tolvaptan-mediated length of stay reduction among heart failure patients with Hyponatremia in the US, based on the EVEREST Trial. J Med Econ 2012;15:1-9
- Dasta JF, Chiong JR, Christian R, et al. Evaluation of costs associated with Tolvaptan- mediated hospital length of stay reduction among US patients with the syndrome of inappropriate antidiuretic hormone secretion, based on SALT-1 and SALT-2 Trials. Hospit Pract 2012:40:1-8
- Singer DE, Albers GW, Dalen JE, et al. Antithrombotic therapy in atrial fibrillation: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. 8th edn. Chest 2008;133(6 Suppl):546S-92S
- Wang TJ, Massaro JM, Levy D, et al. A risk score for predicting stroke or death in individuals with new-onset atrial fibrillation in the community: the Framingham Heart Study. JAMA 2003;290:1049-56
- Zimetbaum PJ, Thosani A, Yu H-T, et al. Are atrial fibrillation patients receiving warfarin in accordance with stroke risk? Am J Med 2010;123:446-53
- Wyse DG, Waldo AL, DiMarco JP, et al. A comparison of rate control and rhythm control in patients with atrial fibrillation. New Engl J Med 2002;347:1825-33
- Wolf PA, Abbott RD, Kannel WB. Atrial fibrillation as an independent risk factor for stroke: the Framingham Study. Stroke 1991;22:983-8
- Mercaldi CJ, Ciarametaro M, Hahn B, et al. Cost efficiency of anticoagulation with warfarin to prevent stroke in medicare beneficiaries with nonvalvular atrial fibrillation. Stroke 2011;42:112-8
- Fang MC, Go AS, Chang Y, et al. A new risk scheme to predict warfarin-associated hemorrhage The ATRIA (Anticoagulation and Risk Factors in Atrial Fibrillation) Study. J Am Coll Cardiol 2011;58:395-401
- Ansell JE, Hughes R. Evolving models of warfarin management: anticoagulation clinics, patient self-monitoring, and patient self-management. Am Heart J 1996;132:1095-100
- Melamed OC, Horowitz G, Elhayany A, et al. Quality of anticoagulation control among patients with atrial fibrillation. Am J Manag Care 2011;17:232-7
- Freeman JV, Zhu RP, Owens DK, et al. Cost-effectiveness of dabigatran compared with warfarin for stroke prevention in atrial fibrillation. Ann Intern Med 2011;154:1-11
- Berg AM. Dabigatran compared with warfarin for stroke prevention in atrial fibrillation. Ann Intern Med 2011;154:570, author reply 570-1
- Sorensen SV, Kansal AR, Connolly S, et al. Cost-effectiveness of dabigatran etexilate for the prevention of stroke and systemic embolism in atrial fibrillation: a Canadian payer perspective. Throm Haemost 2011;105:908-19
- Shah SV, Gage BF. Cost-effectiveness of dabigatran for stroke prophylaxis in atrial fibrillation. Circulation 2011;123:2562-70
- Connolly SJ, Ezekowitz MD, Yusuf S, et al. Newly identified events in the RE-LY Trial. New Engl J Med 2010;363:1875-6
- FDA Draft Briefing Document for the Cardiovascular and Renal Drugs Advisory Committee (CRDAC). NDA 202439: XARELTO® (rivaroxaban) Tablets
- Earnshaw SR, Scheiman J, Fendrick AM, et al. Cost-utility of aspirin and proton pump inhibitors for primary prevention. Arch Intern Med 2011;171:218-25
- Spyropoulos AC, Lin J. Direct medical costs of venous thromboembolism and subsequent hospital readmission rates: an administrative claims analysis from 30 managed care organizations. J Manag Care Pharm 2007;13:475-86.