
Abstract
Objective:
The safety and efficacy of the GLP-1 receptor agonists exenatide BID (exenatide) and liraglutide for treating type 2 diabetes mellitus (T2DM) have been established in clinical trials. Effective treatments may lower overall treatment costs. This study examined cost offsets and medication adherence for exenatide vs liraglutide in a large, managed care population in the US.
Methods:
This was a retrospective cohort analysis comprising adult patients with T2DM who initiated exenatide or liraglutide between 1/1/2010 and 6/30/2010 and had 6 months pre-index and post-index continuous eligibility. Patients were propensity score-matched to controls for baseline differences. Medication adherence was measured by proportion of days covered (PDC). Paired t-test and McNemar’s test were used to compare outcomes.
Results:
Matched exenatide and liraglutide cohorts (n = 1347 pairs) had similar average total 6-month follow-up costs ($6688 vs $7346). However, exenatide patients had significantly lower mean pharmacy costs ($2925 vs $3272, p < 0.001). Among liraglutide patients, patients receiving the 1.8 mg dose had significantly higher average total costs compared to those receiving the 1.2 mg dose ($8031 vs $6536, p = 0.026), with higher mean pharmacy costs in the 1.8 mg cohort ($3935 vs $3146, p < 0.001). There were no significant differences in inpatient or outpatient costs or medication adherence between groups (mean PDC: exenatide 56% vs liraglutide 57%, p = 0.088).
Limitations:
The study assumed that all information needed for case classification and matching of cohorts was present and not differential across cohorts. The study did not control for covariates that were unavailable, such as HbA1c and duration of diabetes.
Conclusions:
Patients initiating exenatide vs liraglutide for T2DM had similar medication adherence and total healthcare costs; however, exenatide patients had significantly lower total pharmacy costs. Patients prescribed 1.8 mg liraglutide had significantly higher costs compared to those on 1.2 mg.
Introduction
Globally, at least 177 million people are estimated to have diabetes; the figure is likely to more than double by 2030Citation1. In the US, diabetes affects 25.8 million people, or 8.3% of the populationCitation2. The number of deaths attributed annually to diabetes is ∼3.2 million, and diabetes has become one of the major causes of premature illness and death in most countries; it is the seventh leading cause of death in the USCitation1,Citation2. In adults, type 2 diabetes mellitus (T2DM) accounts for 90–95% of all diagnosed casesCitation2. Patients who are overweight, inactive, older, or have a family history of diabetes are at increased risk of developing diabetesCitation3. In 2007, the total cost of diabetes in the US was estimated at $218 billion; of that amount, $153 billion was associated with medical expenditures, while the remaining $65 billion was attributable to indirect costsCitation4.
To maintain glycemic control as diabetes progresses over time, patients with T2DM require systematic, individualized, and gradually intensified interventions involving different oral or systemic therapies alone or in combinationCitation5. Glucagon-like peptide 1 receptor agonists (GLP-1 RA) represent a newer class of anti-diabetic medications that do not share the limitations of earlier-generation medications. They are not associated with edema and have a low incidence of hypoglycemia; in addition to providing glucoregulatory effects, weight loss is common in patients receiving GLP-1 RAsCitation6. As of June 2010, two GLP-1 RAs have been approved for treating T2DM in the US. Exenatide (Byetta®, Amylin Pharmaceuticals, Inc., San Diego, CA, USA), approved in 2005, and liraglutide (Victoza®, Novo Nordisk, Inc., Copenhagen, Denmark), approved in January 2010, both are indicated as adjunctive therapies to diet and exercise to improve glycemic control in adults with T2DM. A recent consensus statement by the American Diabetes Association/European Association for the Study of Diabetes recommended use of GLP-1 agonists in patients where hypoglycemia was particularly undesirable (e.g., in patients with hazardous jobs) or promotion of weight loss was a major considerationCitation7.
The safety and efficacy of exenatide and liraglutide for the treatment of T2DM have been well established in clinical trials. However, there is limited information on comparative economic benefits of these therapies for the management of T2DM. Several studies have examined the cost offsets of exenatide compared to insulin glargine and sitagliptinCitation8–10, but to our knowledge, this is the first study comparing cost offsets and medication adherence of exenatide and liraglutide; this economic information may be helpful in determining resource allocations. The primary objective of this study was to compare total healthcare resource utilization and costs, including component costs (inpatient, outpatient, pharmacy), between T2DM patients in the US treated with exenatide vs liraglutide therapy. The secondary objective was to examine medication adherence to these therapies in the real world.
Patients and methods
Data source
Anonymous patient-level data for this retrospective analysis were obtained from the IMS PharMetrics Database (Watertown, MA), comprising adjudicated medical and pharmaceutical claims for over 100 health plans across the US. The database includes inpatient and outpatient diagnoses (International Classification of Diseases – 9th Revision – Clinical Modification [ICD-9-CM] format) and procedures (Current Procedural Terminology – 4th Edition [CPT-4] and Healthcare Common Procedure Coding System [HCPCS] formats), as well as both retail and mail-order prescription records (National Drug Code [NDC] format). Demographic variables; product and payer types; provider specialty; charged, allowed, and paid amounts; and dates inclusive of plan enrollment are available. The data are longitudinal, with average enrollment duration of 2–3 years. In compliance with the Health Insurance Portability and Accountability Act (HIPAA)Citation11, patient data used in these analyses were de-identified; therefore, this study was exempt from Institutional Review Board approval.
Patient selection
Health insurance claims were screened to identify all patients ≥18 years of age with evidence of a pharmacy claim for a GLP-1 RA (exenatide or liraglutide) during the index window from January 1, 2010 to June 30, 2010; the date of the first observed GLP-1 RA claim was considered the index date, and the corresponding therapy was considered the index medication. Patients were included in the study only if they had evidence of T2DM prior to or on the index date; T2DM was defined as at least one claim with an ICD-9-CM code of 250.x0 or 250.x2 or at least one claim for an oral anti-diabetic medication (sulfonylurea, biguanides, alpha-glucosidase inhibitor, dipeptidyl peptidase-4 [DPP-4] inhibitor, dopamine receptor agonist, thiazolidinedione [TZD], any oral combination anti-diabetic therapy, any other oral anti-diabetic therapy). All patients were required to have continuous health plan enrollment for a minimum of 6 months both prior to and following the index date. Patients were excluded from the study if they were aged 65 years or older and not in a Medicare Risk plan (due to the potential for incomplete claims histories), had evidence of type 1 diabetes (ICD-9-CM codes 250.x1, 250.x3) at any time in the study pre-index or post-index periods, had evidence of any GLP-1 RA use in the 6-month pre-index period or evidence of both GLP-1 RA therapies on the index date, or met any of the following conditions in the 6-month pre-index period or on the index date: (1) evidence of pramlintide; (2) evidence of insulin in any form; (3) evidence of gestational diabetes (ICD-9-CM code 648.8x); or (4) evidence of pregnancy with no evidence of delivery or pregnancy termination.
Following the initial identification, liraglutide patients were randomly matched (1:1) to exenatide patients by propensity score methodology. The dependent variable in the multiple logistic regression model was the use of liraglutide therapy; independent variables entered in a stepwise fashion into the propensity model included: (1) age group (18–34, 35–44, 45–54, 55–64, ≥65); (2) gender (male, female); (3) geographic region (Northeast, Midwest, South, West); (4) health plan type (HMO, point-of-service [POS], PPO, consumer-directed/indemnity/unknown); (4) prescribing physician specialty; (5) prior use of oral anti-diabetic medications; (5) diabetes-related macrovascular complications (myocardial infarction [MI], ischemic heart disease, congestive heart failure [CHF], peripheral vascular disease [PVD], cerebrovascular disease [CVD]); (6) diabetes-related microvascular complications (diabetic retinopathy, macular edema, diabetic neuropathy, amputation and ulceration, renal disease); (7) diabetes-related comorbid conditions (hypertension, dyslipidemia, depression, obesity, hypoglycemia); (8) the Charlson Comorbidity Index (CCI) score; (9) pre-index utilization (total inpatient admissions, total emergency room visits, total physician office visits); and (10) pre-index total healthcare costs. Macrovascular and microvascular complications and the five comorbid conditions were identified using ICD-9-CM codes. Comorbidity burden was estimated using the Dartmouth-Manitoba adaptation of the CCI.
Among the index liraglutide patients, follow-up prescription claims for liraglutide were examined to determine the appropriate dosing category for each patient. Patients were required to have a minimum of two consecutive liraglutide claims with the same dose, and preference was given to the consecutive dosing sequence with the maximum number of claims; if each dose had an equal number of claims, preference was given to the higher dose. Once a stable dose was verified, the liraglutide patients were classified into one of two sub-cohorts, 1.2 mg or 1.8 mg; patients who were unable to be accurately classified into one of the two dosing sub-cohorts were excluded from the dosing sub-analyses.
Baseline measures
Outcomes evaluated included resource utilization, direct medical costs, and adherence to index therapy. Demographic characteristics (age, gender, geographic region, health plan and payer types) and clinical characteristics (prescriber specialty associated with the index GLP-1 RA therapy, use of oral anti-diabetic medications, diabetes-related macrovascular and microvascular complications, five selected comorbid conditions, CCI score, HbA1c testing, and total inpatient admissions, emergency room visits, physician office visits, and healthcare costs) were evaluated based on data obtained on the index date or during the pre-index period.
Follow-up outcomes
Healthcare resource utilization and medical costs
Resource utilization and direct medical costs were provided for all services over the 6-month post-index period. The measures evaluated included medications identified by NDC code (oral anti-diabetic agents, insulin, all other pharmacy claims), outpatient care (emergency room visits, physician office visits, laboratory and pathology, radiology examinations, surgical services, ancillary services), and inpatient care (hospital admissions). Costs were defined from the perspective of the health plan, and the allowed amount on the claim was used as a proxy for costs; the allowed amount is the dollar amount a health plan allows for a particular service, and includes the amount paid by the health plan plus any member liability such as co-payments, co-insurance, and deductibles.
Medication adherence
Adherence was calculated for the matched index exenatide and index liraglutide cohorts. It was computed using the proportion of days covered (PDC) over the fixed 6-month post-index period and was capped at 100%. The PDC was used for this study as it incorporates both persistence and adherence as well as avoids double-counting days of medication coverage. The numerator was the total number of days supplied for a patient’s index therapy prescriptions, while the denominator was 180 days, the total number of days in the required follow-up period. Claims extending beyond day 179 were pro-rated to include only the portion of days’ supply captured within the 6-month follow-up window; if a patient refilled a prescription early, any days with “double counting”, or overlapping, from the early refill were counted only once. PDC was presented as both a continuous variable as well as by PDC intervals (<20%, 20–39%, 40–59%, 60–79%, ≥80%); data were provided for all patients and for patients with a minimum of two prescriptions for the index therapy. Patients were considered adherent if PDC was ≥80%.
Statistical analyses
All results were reported for the matched exenatide and liraglutide cohorts as well as for the unmatched index liraglutide dosing sub-cohorts. Descriptive statistics were used to describe differences in patient characteristics, resource utilization and medical costs, and adherence. Summary statistics were presented as total patients (n) with percentages (%) for categorical variables and as mean and standard deviation (SD) for continuous variables. Comparisons within the matched exenatide and liraglutide cohorts used McNemar’s or Bowker’s test for categorical variables and the paired t-test for continuous variables; for comparisons between the unmatched index liraglutide dosing sub-cohorts, statistical testing included the Pearson chi-square test and the independent samples t-test for categorical and continuous variables, respectively. A p-value < 0.05 was considered statistically significant. For analyses among the matched cohorts of patients, p-values were produced only for the matched patients in both cohorts who had data for the measure under evaluation.
Adherence with index therapy among the unmatched cohort of exenatide and liraglutide patients with a minimum of two prescriptions was assessed using logistic regression (the model was performed using the unmatched cohorts because the modeling allowed us to adjust for the effects of the baseline characteristics, again ensuring that the differences observed were not due to the considered baseline measures). The dependent variable in the model was adherence to the index therapy (PDC < 80% vs PDC ≥ 80%); additional independent covariates added to the model included the baseline demographic and clinical characteristics. Results for the model were presented in terms of the odds ratio (OR) along with corresponding 95% confidence intervals (CIs).
All data management and analyses were conducted using Statistical Analysis Software (SAS®), versions 8.2 and 9.1.
Results
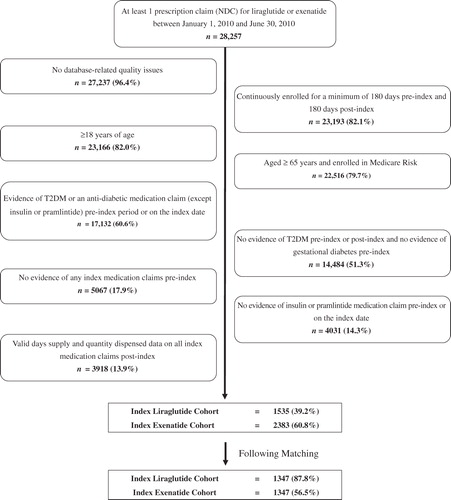
Approximately 28,000 patients with a NDC medication claim for either exenatide or liraglutide between January 1, 2010 and June 30, 2010 were identified; after applying the study inclusion and exclusion criteria, a total of 3918 (13.9%) treated T2DM patients were identified (). Of these patients, 1535 (39.2%) were classified into the index liraglutide cohort and the remaining 2383 (60.8%) were classified into the index exenatide cohort; following matching, 1347 patients were included in each cohort. Index liraglutide patients were further classified into dosing sub-cohorts, with 384 (28.5%) considered recipients of the 1.2 mg dose, and 555 (41.2%) considered recipients of the 1.8 mg dose; 408 (30.3%) index liraglutide patients were unable to be classified by dose and were excluded from sub-cohort analyses.
Figure 1. Identification of the final T2DM study population treated with a GLP-1 receptor agonist.
Matched index exenatide vs index liraglutide cohorts
Baseline patient characteristics
After propensity score matching, the average age was 54.0 (SD = 9.8) years for index exenatide patients and 53.0 (SD = 9.4) years for index liraglutide patients, with similar proportions of males and females in each cohort; the majority of patients were in a PPO plan and covered by a commercial payer (). There was no significant difference in the majority of clinical measures evaluated (). Slightly more index liraglutide patients had a history of oral anti-diabetic use in the pre-index period (97.6% vs 96.4%; p = 0.022), while index exenatide patients were slightly more likely to have a history of hypertension (69.0% vs 68.4%; p = 0.005). The mean (SD) CCI score was 1.5 (0.9) in the exenatide cohort and 1.5 (1.0) in the liraglutide cohort, with two-thirds of patients in each cohort having a CCI score of 1.
Table 1. Baseline characteristics of the matched index therapy cohorts.
Table 2. Clinical characteristics of the matched index therapy cohorts.
All-cause direct medical costs over 6 months
Although there was no significant difference in the mean total overall healthcare costs over the 6-month post-index period between index exenatide patients and index liraglutide patients (mean $6688 vs $7346) (), average total pharmacy costs were significantly higher in the index liraglutide cohort ($3272 vs $2925; p < 0.001). This 12% difference in pharmacy costs was due primarily to the higher costs for the index therapy. Liraglutide prescriptions averaged $1359 among all index liraglutide patients, while the average cost for exenatide among all index exenatide patients was $946. The average cost for sulfonylureas was significantly higher among index exenatide patients, although the overall cost was low ($23 vs $16; p < 0.001). Index liraglutide patients had significantly higher average costs for surgical services ($462 vs $322; p = 0.012) and ancillary services ($1386 vs $966; p = 0.050); there was no difference in inpatient hospitalization costs between the matched index therapy cohorts.
Table 3. All-cause direct medical care costs over 6 months post-index for the matched index therapy cohorts.
All-cause healthcare resource utilization over 6 months
There were few significant differences in 6-month post-index healthcare resource utilization categories among the matched cohort of index exenatide and index liraglutide patients (). A significantly higher proportion of index exenatide patients had evidence of at least one prescription for a sulfonylurea (36.7% vs 29.2%; p < 0.001), oral combination therapy (18.9% vs 15.8%; p = 0.003), and insulin (6.9% vs 4.2%; p = 0.003). Index liraglutide patients averaged 3.4 liraglutide scripts over the follow-up period, while index exenatide patients had an average of 2.8 exenatide scripts over the 6-month post-index period. Index liraglutide patients used slightly more ancillary services post-index (mean 7.7 vs 6.8; p = 0.045), which includes services such as blood venipuncture, electrocardiograms, and vaccine administrations, while there was no significant difference between the matched cohorts in hospital admissions.
Table 4. All-cause healthcare resource utilization over 6 months post-index for the matched index therapy cohorts.
Medication adherence
Adherence to index therapy, as measured using the PDC, was similar between the matched cohorts of index exenatide and index liraglutide patients, averaging ∼ 57% for both (). A similar proportion of index liraglutide patients (31.4% vs 29.3%) were found to be adherent (PDC ≥ 80%); ∼37% of patients in both cohorts were defined as having moderate adherence (PDC 40–79%). When evaluating adherence among the subset of patients with a minimum of two prescriptions for the index therapy (68% of index exenatide patients and 76% of index liraglutide patients; p < 0.001), mean adherence increased as expected in both cohorts (to ∼ 69%), but continued to be non-significantly different.
Table 5. Adherence to the index therapy over 6 months post-index for the matched index therapy cohorts.
Using logistic regression modeling to adjust for baseline patient characteristics in the unmatched cohorts of index exenatide and index liraglutide patients (), there continued to be no significant difference in adherence with index therapy between the two patient cohorts with a minimum of two prescriptions for the index therapy. Examining predictors of adherence, younger patients (aged < 45 years vs 45–54 years), patients with a history of hypertension, and those with a minimum of two emergency room visits in the pre-index period were 24–64% less likely to be adherent to index therapy over 6 months, while older patients (aged > 64 years vs 45–54 years), males, patients with prior use of sulfonylureas or DPP-4 inhibitors or with a history of depression, patients in a POS (vs HMO) plan, those who were prescribed their index therapy by an endocrinologist (vs internal medicine physician), and patients with higher total pre-index healthcare costs were 17–53% more likely to be adherent over the 6-month post-index period.
Table 6. Logistic regression of medication adherence following the index date (adherence ≥ 80% PDC) among the unmatched exenatide (n = 918) and liraglutide (n = 1024) patients with ≥2 prescriptions for the index therapy.
Unmatched index liraglutide dosing: 1.2 mg vs 1.8 mg cohorts
Baseline patient characteristics
In the sub-group analysis, within the unmatched liraglutide dosing cohorts, the average age for the 1.2 mg (n = 384) and 1.8 mg (n = 555) patients was ∼53 years, with a similar distribution of patients by gender, and with the majority of patients in a PPO plan and covered by a commercial payer (). Liraglutide patients in the 1.8 mg cohort were significantly more likely to have had a history of depression (5.9% vs 2.9%; p = 0.028), and these patients also were significantly more likely (p = 0.004) to have had their index therapy prescribed by a specialist (e.g., endocrinologist or cardiologist) vs a generalist (e.g., general practice/family practice or internal medicine physician) ().
Table 7. Baseline characteristics of the unmatched index liraglutide dosing sub-cohorts.
Table 8. Clinical characteristics of the unmatched index liraglutide dosing sub-cohorts.
All-cause direct medical costs over 6 months
Patients defined as part of the 1.8 mg liraglutide cohort had significantly higher overall total costs over the 6-month post-index period compared to those in the 1.2 mg liraglutide cohort, averaging $8031 (SD = $10,699) vs $6536 (SD = $9222) (p = 0.026) (). Total pharmacy costs made up ∼50% of the total overall costs, with average pharmacy costs of $3935 in the 1.8 mg cohort and $3146 in the 1.2 mg cohort (p < 0.001). Patients defined as taking 1.8 mg liraglutide had 37% higher liraglutide prescription costs compared to patients defined as taking 1.2 mg liraglutide (mean $1863 vs $1362; p < 0.001); these liraglutide prescription costs accounted for 43% of the total pharmacy costs among the 1.2 mg cohort and for 47% of the total pharmacy costs among the 1.8 mg cohort. Patients prescribed liraglutide 1.8 mg also had significantly higher costs for TZDs (mean $201 vs $143; p = 0.040).
Table 9. All-cause direct medical care costs over 6 months post-index for the unmatched index liraglutide dosing sub-cohorts.
All-cause healthcare resource utilization over 6 months
The only significant differences in healthcare utilization observed between the 1.2 mg and 1.8 mg liraglutide dosing sub-cohorts were the higher proportion of patients prescribed liraglutide 1.8 mg with at least one prescription for a TZD (20.9% vs 14.8%; p = 0.019), and the higher number of laboratory and pathology tests post-index (mean 9.0 vs 7.8; p = 0.033) in the 1.8 mg cohort ().
Table 10. All-cause healthcare resource utilization over 6 months post-index for the unmatched index liraglutide dosing sub-cohorts.
Discussion
This retrospective cohort study examined economic outcomes and medication adherence among T2DM patients treated with exenatide vs liraglutide therapy. Although there was no significant difference in total healthcare costs among patients initiating exenatide compared to liraglutide, patients initiating on exenatide therapy had significantly lower total mean pharmacy costs compared to those initiating on liraglutide therapy. The cost of the index therapy was a key driver of this difference. On average, drug costs for exenatide prescriptions among index exenatide patients were lower than the costs for liraglutide prescriptions among liraglutide patients. The sub-group analysis of liraglutide patients with dosing information found that those treated with 1.8 mg doses had higher mean total and pharmacy costs compared to those treated with 1.2 mg doses. There was no significant difference in average patient adherence between the index therapies; therefore, it is unlikely that adherence to therapy was a major factor in the results reported in the economic analyses.
The data presented here extend recent studies that have provided evidence of the economic benefit of exenatide treatment over other anti-diabetic therapies. A 2011 study by Pawaskar et al.Citation8 found that T2DM patients initiating exenatide therapy had significantly lower resource utilization (including a 19% lower likelihood of all-cause hospitalizations) and total medical costs (inpatient and outpatient costs specifically) compared to insulin glargine-treated patients. Misurski et al.Citation9 showed that T2DM patients initiating therapy with exenatide vs insulin glargine incurred significantly lower total all-cause medical costs ($19,293 vs $23,782; p < 0.001) and total diabetes-related medical costs ($7833 vs $8536; p < 0.001). Exenatide also has been found to have cost savings compared to use of sitagliptin, with lower total 6-month costs ($9340 vs $9995, p < 0.001)Citation10. In all of these studies, any higher pharmacy costs associated with exenatide use were outweighed by significantly lower inpatient and outpatient medical costs. Finally, a comparison of liraglutide to exenatide over a 35-year time horizon using the CORE Diabetes Model estimated that total lifetime treatment costs for liraglutide were $12,956 higherCitation12.
The results presented here must be viewed in light of some limitations associated with this study using claims data. If an incorrect diagnosis was listed in the medical record, or the medical record was incomplete, then patients might have been misclassified, resulting in selection bias. The study also assumes that all information needed for case classification and matching of cohorts is present and not differential across the cohorts of interest. Although propensity score matching was used to control for observed differences between cohorts, this does not control for measured confounding bias. The study also could not control for important covariates such as HbA1c, body mass index, and duration of diabetes, due to the lack of available data in the claims database.
The correspondence between pharmacy submission of claims and patients’ receipt and consumption of the medication is assumed and not directly measured. Although pharmacy claims can be used to analyze medication adherence and are typically the most readily available data, these claims may not always provide an accurate estimate of true medication adherence due to multiple factors, including patients filling prescriptions but not actually taking the medications as prescribed (e.g., stockpiling) or the use of auto-refill programs. However, prior work suggests that medication exposure measures can be accurately derived from pharmacy claimsCitation13, and we are confident that, in this disease area, use of pharmacy claims is an accurate measure of adherence in this patient population. The dosing data for the index liraglutide medication was difficult to interpret due to the nature of claims for injectable therapies; therefore, any data based solely on dosing patterns must be interpreted with caution.
The claims dataset does not include uninsured patients and those covered only by Medicare (Part D), and the source population consisted primarily of commercially-insured patients in the US; therefore, the results are most generalizable to similar commercially-insured patients and may not be generalizable to other populations if they differ in their accessibility to physician services or prescriptions. The database does not provide information on systemic factors that could affect care, including plan limits on medication use. Due to the large and diverse nature of the plans in the database, however, these factors should not have impacted our study results. Lastly, the observational nature of the study design does not permit causal inferences.
Conclusion
Exenatide treatment was associated with significantly lower pharmacy costs compared to liraglutide treatment over a 6-month follow-up period; there was no significant difference in total healthcare costs.
Transparency
Declaration of funding
This study was funded by Amylin Pharmaceuticals, Inc.
Declaration of financial relationships
MP is a former employee of Eli Lilly and Company; she currently is employed by MedImmune, LLC (Gaithersburg, Maryland). JHB is an employee and stockholder of Amylin Pharmaceuticals, Inc. (San Diego, CA).
Acknowledgments
The authors would like to thank Daniel B. Smith, MA (IMS Health, Inc., Watertown, MA) for his assistance in the statistical programming for the study.
References
- World Health Organization (WHO). Global Strategy on Diet, Physical Activity and Health. Diabetes Facts. http://www.who.int/hpr/gs.fs.diabetes.shtml. Accessed February 16, 2012 (Copyright 2003)
- Centers for Disease Control and Prevention. National diabetes fact sheet: National estimates and general information on diabetes and prediabetes in the United States, 2011. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, 2011. http://www.cdc.gov/diabetes/pubs/pdf/ndfs_2011.pdf. Accessed February 16, 2012
- American Diabetes Association (ADA). Diabetes Basics: Prevention, Risk Factors. http://www.diabetes.org/diabetes-basics/prevention/risk-factors/. Accessed February 16, 2012 (Copyright 1995--2012)
- Dall TM, Zhang Y, Chen YJ, et al. The economic burden of diabetes. Health Aff 2010;29:297-303
- Saydah SH, Fradkin J, Cowie CC. Poor control of risk factors for vascular disease among adults with previously diagnosed diabetes. JAMA 2004;291:335-42
- Gallwitz B. Glucagon-like peptide-1-based therapies for the treatment of type 2 diabetes mellitus. Treat Endocrinol 2005;4:361-70
- Nathan DM, Buse JB, Davidson MB, et al. Medical management of hyperglycemia in type 2 diabetes: a consensus algorithm for the initiation and adjustment of therapy: a consensus statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetes Care 2009;32:193-203
- Pawaskar M, Zagar A, Sugihara T, et al. Healthcare resource utilization and costs assessment of type 2 diabetes patients initiating exenatide BID or glargine: a retrospective database analysis. J Med Econ 2011;14:16-27
- Misurski D, Lage MJ, Fabunmi R, et al. A comparison of costs among patients with type 2 diabetes mellitus who initiated therapy with exenatide or insulin glargine. Appl Health Econ Health Policy 2009;7:245-54
- Lage MJ, Fabunmi R, Boye KS, et al. Comparison of costs among patients with type 2 diabetes treated with exenatide or sitagliptin therapy. Adv Ther 2009;26:217-29
- Health Insurance Portability and Accountability Act (HIPAA), Pub. L. No. 104-191,110 Stat.1936 2006. Washington, DC, USA: US Department of Health and Human Services
- Lee WC, Conner C, Hammer M. Results of a model analysis of the cost-effectiveness of liraglutide versus exenatide added to metformin, glimepiride, or both for the treatment of type 2 diabetes in the United States. Clin Ther 2010;32:1756-67
- Lau HS, de Boer A, Beuning KS, et al. Validation of pharmacy records in drug exposure assessment. J Clin Epidemiol 1997;50:619-25