
Abstract
Background:
Several studies have demonstrated that the use of single tablet regimens (STRs) in hypertension is associated with improved outcomes and reduced healthcare costs compared with individual component regimens. The objective was to carry out a retrospective analysis of a UK general practice population to test these conclusions in a UK context.
Method:
A retrospective cohort study was carried out using a primary care database (The Health Improvement Network; THIN), comparing 9929 hypertensive patients on STRs with 18,665 patients on individual component therapy. Data were collected for prescriptions, significant cardiovascular events, and out-patient referrals over a minimum follow-up period of 5 years after initiation of therapy. Current NHS costings were applied to the data, to arrive at an estimate of comparative resource use.
Results:
There were significantly more cardiovascular events in the individual component group than those treated with a single tablet regimen. Five year event rates: 8.3% vs 13.6%; Absolute Risk Reduction (ARR) = 5.3%; Number needed to treat (NNT) = 18.9. After correction for potential confounders, the hazard ratio was 0.74 (95%CI = 0.70–0.77), p < 0.0001. Hospital admission costs were lower in the STR group, but drug costs were higher. Overall, the mean annual management cost per patient was similar in the two groups (£191.49 vs £189.35).
Key limitations:
The study was based on a retrospective cohort and the result may therefore be influenced by unidentified confounders. It was not possible to identify the reasons for individual prescriptions, some of which may have been issued for reasons other than hypertension. Costings for some components of the outcome could not be assessed from the dataset and are therefore omitted from the analysis. Finally, no attempt was made to distinguish outcomes associated with individual classes of anti-hypertensives.
Conclusions:
This study confirms the association observed by other authors that patients treated with STRs are less likely to experience serious cardiovascular events than those on individual component therapy. In a UK context this analysis has shown that potential hospital savings broadly offset the additional drug acquisition costs associated with STRs. These agents can therefore be considered cost neutral.
Introduction
The identification and effective treatment of hypertension has formed a key health outcome for UK primary care for the past 20 years. However, despite the introduction of incentivized target systems (Quality Outcomes Framework: QoF), achievement of blood pressure control is still sub-optimal. In 2010–11, 20% of patients with hypertension failed to achieve the QoF blood pressure audit standard of 150/90Citation1. Whilst up-to-date information on the number of patients failing to meet the more challenging clinical target of 140/90 used by the National Institute for Health and Clinical Excellence (NICE) and the British Hypertension Society (BHS) are not available, comparisons of data from previous yearsCitation2,Citation3 would suggest that the current level of QoF audit target achievement corresponds to ∼40% of patients with hypertension failing to reach clinically relevant targets.
Published QoF data are presented as a binary response—either a patient has achieved the target or they have not—and there is no indication as to how far individuals fall short of the objective. However, even if these patients may be relatively close to their treatment target, the clinical consequences of the shortfall can be significant. Even a 2–3 mmHg difference in systolic BP, if sustained for 5 years or more, can result in a 15% higher risk of an adverse cardiovascular outcomeCitation4.
Whilst there are a number of possible explanations for the under-achievement of clinical targets, a key factor is likely to be poor adherence and persistence amongst patients who would otherwise have been adequately treatedCitation5. A recently published study assessed the impact of supervised tablet administration in 37 patients who had been referred to secondary care with apparently treatment-resistant hypertensionCitation6. Despite a mean starting blood pressure of 179/98, in 78% of cases the QoF target was achieved simply by ensuring treatment was taken as prescribed, while in 60% of cases the clinical target of 140/90 was reached. Given the strong link between blood pressure reduction and clinical outcomes, strategies aimed at improving adherence clearly have a powerful potential for reducing cardiovascular events.
One approach to improving adherence that has proved effective is the use of single tablet regimens (STRs), which may contain two or three individual components in a range of dose combinations. The use of STRs has been shown to improve treatment adherence vs the individual components prescribed separatelyCitation7,Citation8 with improvements of 20–25% typically being demonstrated. In line with the expected impact of improved adherence, there is also good evidence that the use of STRs results in a reduced risk of admission for cardiovascular eventsCitation9 with consequent cost savings to the healthcare commissionerCitation9,Citation10, across a wide range of organizations.
Despite this evidence, and the endorsement of the approach by professional bodiesCitation11, there is a long clinical tradition in the UK that the use of STRs should be avoided, due principally to a fear that fixed dose combinations may limit dose titration flexibilityCitation12. As a consequence, only ∼1.5% of prescriptions for anti-hypertensives in the UK are for STRsCitation13, compared with, for instance, more than 50% in the USCitation9. Given that most of the studies showing the benefit of STRs have been carried out in the US and GermanyCitation9,Citation10, it is uncertain whether the clinical and budgetary benefits identified in studies carried out elsewhere are also applicable in the UK.
The objective of this study, therefore, is to test two distinct but related hypotheses that have already been demonstrated elsewhere, within a UK healthcare context:
That hypertensive patients treated with regimens containing STRs experience fewer serious cardiovascular events than those treated with regimens containing exclusively individual components; and
That the additional drug acquisition cost incurred by the use of STRs is offset by savings in the secondary care budget.
Methods
Study design
The chosen method is a retrospective cohort study, with sample matching for age, sex, and GP practice, using patient records drawn from the THIN dataset. The Health Improvement Network (THIN) provides regularly updated anonymized primary care data from 479 UK general practices using the INPS VISION computer system. The database includes 3.4 million active patients and a historical data from a further 5.8 million patients. Records available for these patients include full prescribing data, diagnoses from GP and practice nurse contacts, secondary care referrals, and discharge diagnoses from hospitals.
Ethics approval for the study was granted by the THIN Scientific Review Committee (Protocol number 11-053).
Population
Data for this study were drawn from a sub-set of 320 practices within THIN containing validated data up to 1/1/2011. The parent population was selected according to the following criteria:
Diagnosis of hypertension recorded;
Age 18+;
On any treatment licensed for use in hypertension:
Thiazide type diuretic (BNF 2.2.1),
Beta-blocker (BNF 2.4),
Calcium channel blocker (CCB) (BNF 2.6.2),
ACE inhibitor (BNF 2.5.5.1),
Angiotensin receptor blocker (ARB) (BNF 2.5.5.2),
Alpha-blocker (BNF 2.5.4),
Renin inhibitor (BNF 2.5.5.3),
Vasoldilating antihypertensives (BNF 2.5.1),
Centrally acting antihypertensives (BNF 2.5.2), or
Any combination of these agents; and
Minimum 5 years follow-up after first record of anti-hypertensive treatment, unless follow-up was terminated by death.
In order to qualify under the final criterion, no patient who had initiated anti-hypertensive treatment after 1/1/2006 was admitted to the dataset. There was no prior cut-off date specified.
From this parent population, two datasets were selected:
Group A: Any patient who had received a single tablet regimen ± additional anti-hypertensive agents. STRs were defined as any combination tablet that incorporated two or more agents from different treatment classes, as listed above.
Group B: An age-, sex-, and practice-matched control group taking two or more individual component anti-hypertensive medications who had not received a prescription for any STR over a 5-year minimum follow-up period after the first recorded prescription. For every patient in group A, two matched controls were selected for group B.
Group inclusion was based purely on whether the patient had an STR-component to their treatment—no attempt was made to match patients across classes.
Study variables
For each patient, the following items were extracted from the record:
Practice ID;
Patient year of birth;
Patient gender;
List of all anti-hypertensive prescriptions prescribed (drug name, formulation, strength, quantity, date prescribed);
Date of first recorded anti-hypertensive prescription;
List of all blood pressure readings both pre- and post-anti-hypertensive prescription;
Full list of all recorded consultations and documented referrals and admissions;
In order to identify those patients with pre-existing ischemic heart disease or diabetes, any of the following diagnoses recorded prior to the first recorded anti-hypertensive prescription were extracted:
Myocardial infarction,
Acute coronary syndrome,
Unstable angina,
Stable angina,
Coronary revascularization,
Ischaemic heart disease (Not otherwise specified), or
Diabetes (any type);
In order to identify cardiovascular outcomes, any of the following relevant diagnoses recorded after the first recorded anti-hypertensive prescription were extracted, with the date of the first recorded diagnosis:
Death,
Stroke,
TIA,
Myocardial infarction,
Acute coronary syndrome,
Unstable angina,
Coronary revascularization, or
Heart failure; and
All records of referral to a hypertension, cardiology, or general medical clinic were extracted.
Analysis
Sample size was calculated in order to power the study sufficiently to demonstrate a 20% reduction in cardiovascular outcomes in year 1. The following assumptions were used:
Event rate in control group: 4%;
Event rate in STR group: 3.2%;
Ratio controls:STR: 2:1;
Power: 90%; and
Alpha: 0.05.
This yielded a required sample size of 8851 in the STR group and 17,702 in the control group. In order to allow for losses following data cleaning in the test population, an initial sample of 10,000 in the STR group and 20,000 in the control group was chosen.
Preliminary analysis of the original dataset revealed a degree of cross-contamination—principally patients in the control group who had received prescriptions for STRs at some stage since their initial anti-hypertensive prescription. These individuals were therefore excluded, yielding final cleaned populations of 9929 in the STR group and 18,665 in the control group. This fell well within the calculated sample size requirements. The potential loss of matching of controls due to unequal patient loss during the cleaning process was taken into account in the analysis (see below).
Objective 1: To identify the relative risk of any CV outcomes in the two groups
From the global set of diagnoses and consultations, any Read codes associated with an adverse cardiovascular outcome was extracted and limited to those events occurring after the first prescription date. These diagnoses were then sorted by date of occurrence and, for each patient, the first recorded such event following the prescription date recorded.
Survival analysis
In order to allow for differences in baseline characteristics, a Cox proportional hazards survival approach was adopted. Potential covariates were tested using the Cox function, in order to ascertain whether they exerted an independent effect on event risk. Only those characteristics that exerted a significant independent effect were included in the survival model. Although the original dataset had been matched for age, sex, and general practice, the loss of nearly 7% of the control group in the data cleaning process may have compromised this matching: for this reason it was planned to include these factors as covariates in the analysis.
Cox proportional hazards survival curves were constructed for both the crude data and data corrected for confounding characteristics. Events were censored at 10 years. Hazard ratios with 95% confidence intervals were estimated for the comparison between the two groups.
Objective 2: To assign costs to both prescriptions and events to allow comparison of the two groups
In all cases, costs incurred were assessed over the 5-year period following treatment initiation, with results being divided into ‘current year’ and ‘years 2–5’.
Hospital admissions
All unique qualifying events occurring in the 5 years post-treatment initiation were recorded as part of objective 1. Those events likely to require hospital admission (myocardial infarction, acute coronary syndrome, revascularization, stroke, TIA) were assigned costings based on the 2011–12 Payment by Results tariff for England (see ). The quality of the data recording for admission events was insufficient to allow accurate HRG mapping, so broad categories were used instead.
Table 1. Payment by results tariff prices used in this analysisCitation14.
Events included in objective 1, but for which primary care records were insufficient to determine whether hospital admission had also occurred (principally congestive heart failure, impaired ventricular function, and death), were excluded from the costing exercise.
Out-patient referrals
From the global set of diagnoses and consultations, any record of a new referral to a cardiology, general medical, or hypertension clinic were extracted and limited to those referrals occurring after the first prescription date. Referrals were costed at £214 per first attendance, in accordance with the PbR tariff (). Attendance at follow-up appointments is rarely recorded in primary care records and, therefore, cannot be captured in the costing process.
Prescriptions
Prescription records for anti-hypertensive drugs were aggregated for each patient over a 5-year period following the first recorded prescription, with the number of individual doses prescribed for each agent over the period being recorded. Current net ingredient cost per dose, based on the September 2011 edition of the BNF were applied to these dose records, in order to arrive at a total NHS cost of drugs used, expressed at 2011 prices. Although some anti-hypertensive drugs have more than one indication for use (e.g., calcium channel blockers for angina), it was not possible to link each prescription with the clinical justification for its use and so the cost of all prescription events was logged.
An additional costing was added to each prescription issued, in respect of the dispensing fee paid to the pharmacist, which is payable per item dispensed. The formula by which this is calculated is complex, and there is insufficient information within GP prescribing data to make an accurate estimate for each prescription. The estimate was therefore based on published aggregated returns from the NHS Business Services Agency which showed that, in the first half of 2010 the average fee paid to community pharmacists was £2.07 per item dispensedCitation15. Although not often included in NHS cost analyses, the dispensing fee is non-negligible and will often exceed the cost of drugs in the case of generic prescriptions. It is particularly important for this analysis, as STRs incur only a single fee, regardless of the number of component drugs in the tablet, while individually prescribed components will incur one fee per agent prescribed.
Total costs
The three cost variables were then aggregated to arrive at an estimate of total direct costs incurred per patient per year.
Results
After cleaning and checking of supplied datasets, there were 9929 qualifying patients in group A and 18,665 qualifying patients in group B. Baseline characteristics are described in .
Table 2. Baseline characteristics.
Therapy
In the 5 years following the first prescription in the STR group, 2122 patients (21.4%) had exclusively STRs prescribed; 4501 patients (45.3%) had STR + additional component anti-hypertensives prescribed; 3306 patients (33.3%) were switched from STR to individual components at some point during follow-up, but did not have the two regimens prescribed simultaneously.
No patient in the individual component group had an STR prescription at any stage in the 5 years following the first anti-hypertensive prescription.
In the STR group, primary prescriptions were for:
Beta blocker + thiazide: 41.0%;
ACE inhibitor + thiazide: 29.2%;
ARB + thiazide: 19.8%;
Beta blocker + CCB: 9.5%;
ACE inhibitor + CCB: 0.5%; and
ARB + CCB: <0.1%.
In the individual component group, prescriptions were for:
CCB: 24.3%;
ACE inhibitor: 23.8%;
Beta blocker: 21.9%;
Thiazide: 17.5%;
ARB: 6.8%;
Alpha blocker: 5.1%; and
Others: 0.5%.
Cardiovascular events
Overall, there were 2173 first events recorded in group A (21.9%) and 6285 in group B (33.7%) (see and ). The difference in event rates was seen at all time points. A Cox proportional hazards analysis on the crude data, without correction for confounding variables, yielded a hazard ratio of 0.73 (95% CI = 0.70–0.76); p < 0.0001 (see ).
Figure 1. Cox proportional hazards survival analysis (corrected). Censored at 10 years.
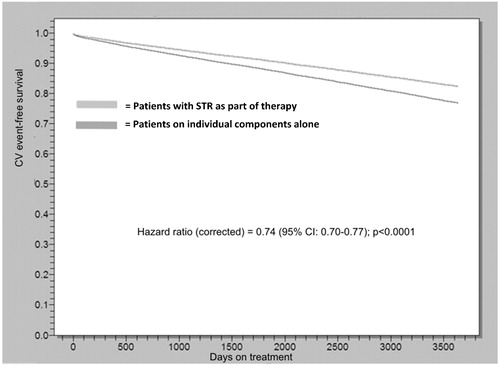
Table 3. First cardiovascular events.
Table 4. Breakdown of first event by sub-type.
Corrected results
The following variables were identified as having a significant independent impact on the risk of a CV event and were used as variables in a Cox proportional hazards analysis:
Age at start of treatment;
Male sex;
Previous IHD (myocardial infarct, unstable angina, stable angina, revascularization); and
Diabetes.
Post-treatment blood pressure (both absolute values and target achievement) was not a predictor of outcome. The corrected hazard ratio of 0.74 (95%CI = 0.70–0.77) was little different from the result obtained for the uncorrected analysis (see ).
Referrals
Overall, there were 1869 referrals to medical or cardiology clinics recorded in group A (18.8%) and 4429 in group B (23.7%) (). Patients on fixed dose combinations were seen more frequently in the short-term following initiation of treatment and less frequently in the long-term.
Table 5. Referrals to hypertension, cardiology, or general medical OPD.
Costs
lists the overall costs incurred for the two groups, across the three categories: admissions, out-patients, and drug costs. The same data are listed in , expressed as a mean cost per patient. The overall mean annual costs over the 5-year time frame of the analysis were £191.49 (SD = 320.93) in group A and £189.35 (SD = 405.82) in group B, representing virtual equality between the two groups.
Table 6. Total direct costs incurred.
Table 7. Mean costs per patient per year.
Discussion
This analysis has demonstrated that hypertensive adults treated with regimens including single tablet anti-hypertensives have a significantly lower risk of experiencing a serious cardiovascular event than patients treated with separately prescribed anti-hypertensives. The nature of the database meant that adherence to prescribed therapy could not be directly assessed—however, it seems likely that improved compliance on STRs underlies this observed effect.
The cost savings associated with this lower event rate almost offset the additional drug acquisition costs, the net additional cost of STR treatment over a 5-year period being £10.70 (SD = 21.90). The absolute difference in cardiovascular event rate over this period was 5.3%, meaning that 18.9 patients would need to be treated with STR over 5 years to avoid one event, at an additional overall cost of £202.23.
The observed reduction in risk of cardiovascular adverse events (HR = 0.74; 95% CI = 0.70–0.77) is consistent with that seen by other authors. In a recently published analysis of a large US claims databaseCitation9, hospital admissions for cardiovascular reasons were significantly lower in 382,476 hypertensive patients treated with STR (IRR = 0.71; 95% CI = 0.69–0.72) compared with 197,375 patients on individual component therapy. In this study, however, unlike this analysis, the authors noted a net financial saving associated with STR use, a finding that was confirmed in a meta-analysis of 12 other randomized controlled trialsCitation10.
It seems likely that this difference in cost outcomes is driven by national differences. The majority of current literature on the subject is derived from analyses of US practice, where the cost of hospital treatment tends to be significantly higher than tariff prices in the UK. An admission for elective coronary artery bypass grafting, for example, currently carries a tariff of £7318 in the UKCitation14. In contrast, an analysis based on 2005 Medicare claims in the USCitation15 suggested a mean cost for the same procedure of $45,358, equivalent to £24,950 at the mid-2005 exchange rate. Clearly, given that the benefit of STRs is driven by a reduction in hospital admissions, higher prices will tend to draw the two treatment groups apart, such that the difference in secondary care expenditure will tend to overwhelm the relatively small difference in drug acquisition cost.
The relationship between blood pressure changes and the observed outcomes in this analysis is, at first sight, confusing. The STR group had significantly higher mean pre-treatment blood pressure than those on individual component therapy. After treatment, however, mean achieved blood pressure levels were slightly, but significantly lower in the STR group, with significantly more patients achieving both audit and clinical blood pressure targets. These finding are consistent with the hypothesis that the use of STRs reduces blood pressure to a greater extent than individual components, thanks to the beneficial effects on adherence and persistence.
However, regression testing was unable to identify a significant impact of these blood pressure differences on the risk of experiencing a cardiovascular outcome. Indeed, introduction of some of the blood pressure variables prevented the Cox model from converging at all. There are several possible reasons for this unexpected result.
Given the protocol requirement for 5 years minimum follow-up, the majority of the pre-treatment data antedated the introduction of QoF and therefore the quality of blood pressure recording prior to initiating treatment was not high; 18% of STR patients and 36% of individual component patients had no blood pressure recorded at all, while, for more than half of the remaining patients, the estimate of pre-treatment blood pressure was based on three or fewer readings. The possibility of selective recording introduces a potential bias into the assessment of this parameter.
There were potential differences between the two groups in terms of blood pressure recording. The median date of first treatment was 11/10/1999 in the STR group and 2/2/1995 in the individual component group. Computerization of UK general practice started with enthusiasts in the late 1980s but was not universal until the late 1990s. In the early stages of computerization, practices did not necessarily make a comprehensive clinical record: this only becoming the norm once incentives such as QoF made it a necessity. Unfortunately there is no way of knowing whether the absence of a blood pressure record for an individual means that no measurement was made or simply that the record was not entered on the computer. However, the fact that treatment was more likely to be initiated early in the evolution of practice computing in the individual component group introduces a further potential bias for the pre-treatment blood pressure metric.
Finally one must consider the reliability of the data actually recorded. Records relating to clinical events, prescriptions issued, and referrals made are reasonably robust, as they are simply records of fact. Blood pressure recording, however, is less clear cut. There is good evidence from the literature that recorded blood pressures are susceptible to recorder bias, with the figure being recorded not necessarily reflecting the true measured blood pressureCitation16.
Overall, the combinations of these potential biases may well have been enough to blur the connection between blood pressure control and the observed reduction in cardiovascular events. Certainly, it is difficult to conceive of any other reason why STRs should exert this effect.
Study limitations
The primary limitation is inherent to the retrospective cohort methodology. Because patients have not been randomized to treatment with STRs or individual components, there may be factors that have not been identified that may have influenced this decision and which will have a bearing on the results. Although the method allowed for many of these potential confounders to be taken into account, it is impossible to be sure that all such factors have been identified.
The second factor relates to the fact that many cardiovascular drugs are used for multiple indications. Thus, beta-blockers and ACE inhibitors may be used for their cardioprotective role in patients who have had a previous MI, while calcium channel blockers may be used for their anti-anginal effect. Where a patient is also hypertensive, it would be reasonable to choose a treatment in the appropriate drug class to cover both indications. In these circumstances, it is unlikely that a STR would be chosen, as the majority of these are combinations of a beta-blocker, ACE inhibitor, or ARB with a thiazide, a class which has no particular cardioprotective properties beyond its ability to lower blood pressure. Although a correction was made for pre-existing ischemic heart disease in the analysis to mitigate this effect, there is no way to directly identify those patients in whom this was the determining factor in treatment choice, given the limitations of a retrospective dataset.
Thirdly, although the events constituting the primary outcome are sufficiently serious to be well recorded in GP clinical records, for some adverse cardiovascular outcomes the spectrum of disease is very wide. For instance the diagnosis of cardiac failure could imply anything from swollen ankles to acute pulmonary edema. The information available to us in this dataset did not allow us to examine any additional free-text notes entered by the GP. In the absence of this fine detail, it is possible that some individuals have been included in the primary outcome who would not clinically have been considered to have serious cardiovascular disease.
A further issue is that the analysis did not control for different drug classes. Although the intention was to compare any STR regimen with individual component therapy, it is possible that differences exist between drug classes. This hypothesis should be explored in a future analysis.
Conclusion
This retrospective cohort study has confirmed the association observed by other authors that patients treated with single tablet regimens are less likely to experience serious cardiovascular events than those on individual component therapy. Although it seems likely that this effect is mediated by improved blood pressure control, it has not been possible to confirm this assumption, due to data limitations. In a UK context the study has shown that the reduction in cardiovascular events results in a reduction in healthcare costs that approximately matches the additional drug acquisition costs associated with STRs. These agents can therefore be considered cost neutral.
Transparency
Declaration of funding
This study was funded by Daiichi Sankyo UK Ltd. Daiichi Sankyo UK had no editorial input into the content of the publication, other than to review for medical accuracy.
Declaration of financial/other relationships
Dr Belsey has disclosed that he has received payment from Daiichi Sankyo UK Ltd for health economic consultancy. He has also carried out other paid consultancy for the pharmaceutical industry, including other companies involved in the management of hypertension.
References
- NHS: The Information Centre. Quality and Outcomes Framework (QoF) 2010--11. England. 2012; http://www.ic.nhs.uk/statistics-and-data-collections/audits-and-performance/the-quality-and-outcomes-framework/the-quality-and-outcomes-framework-2010-11. Accessed 24 January 2012
- NHS: The Information Centre. Time Series Analysis for selected clinical indicators from the Quality and Outcomes Framework 2001-2006. 2007; http://www.ic.nhs.uk/webfiles/QOF/2006-07/QResearch%202006-70%20QOF/Time%20Series%20Analysis%20for%20Selected%20Clinical%20Indicators%20from%20QOF%202001-2006%20Report.pdf. Accessed 24 January 2012
- NHS: The Information Centre. Health Survey for England 2006. 2008; http://www.ic.nhs.uk/statistics-and-data-collections/health-and-lifestyles-related-surveys/health-survey-for-england/health-survey-for-england-2006:-cvd-and-risk-factors-adults-obesity-and-risk-factors-children. Accessed 24 January 2012
- Staessen JA, Wang JG, Thijs L. Cardiovascular protection and blood pressure reduction: a meta-analysis. Lancet 2001;358:1305-15
- Elliott WJ. Improving outcomes in hypertensive patients: focus on adherence and persistence with antihypertensive therapy. J Clin Hypertens 2009;11:376-82
- Bunker J, Callister W, Chang CL, et al. How common is true resistant hypertension? J Hum Hypertens 2011;25:137-40
- Bangalore S, Kamalakkannan G, Parkar S, et al. Fixed-dose combinations improve medication compliance: a meta-analysis. Am J Med 2007;120:713-9
- Gupta AK, Arshad S, Poulter NR. Compliance, safety, and effectiveness of fixed-dose combinations of antihypertensive agents: a meta-analysis. Hypertension 2010;55:399-407
- Yang W, Chang J, Kahler KH, et al. Evaluation of compliance and health care utilization in patients treated with single pill vs. free combination antihypertensives. Curr Med Res Opin 2010;26:2065-76
- Sherrill B, Halpern M, Khan S, et al. Single-pill vs free equivalent combination therapies for hypertension: a meta-analysis of health care costs and adherence. J Clin Hypertens (Greenwich ) 2011; 13:898-909
- Bonny A, Lacombe F, Yitemben M, et al. The 2007 ESH/ESC guidelines for the management of arterial hypertension. J Hypertens 2008;26:825-6
- Audit Commission. A prescription for improvement: towards more rational prescribing in general practice. London: Audit Commission, 1994
- NHS: The Information Centre. Prescription cost analysis: England. 2010. http://www.ic.nhs.uk/pubs/prescostanalysis2010. Accessed 24 January 2012
- Department of Health. 2011-12 Tariff for admitted patient care & outpatient procedures. 2011; http://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/documents/digitalasset/dh_125398.xls. Accessed 24 January 2012
- Birkmeyer JD, Gust C, Baser O, et al. Medicare payments for common inpatient procedures: implications for episode-based payment bundling. Health Serv Res 2010;45:1783-95
- de Lusignan S, Belsey J, Hague N, et al. End-digit preference in blood pressure recordings of patients with ischaemic heart disease in primary care. J Hum Hypertens 2004;18:261-5