Abstract
Objectives:
The purpose was to quantify patient and parent preferences for administration attributes of immunoglobulin (IG) treatments; and determine which administration attributes were most important to users of IG treatment and whether patients and parents have similar preferences for administration attributes.
Methods:
US adult patients and parents of children with a self-reported physician diagnosis of a primary immunodeficiency disorder completed a best-practice web-enabled choice-format conjoint survey that presented a series of 12 choice questions, each including a pair of hypothetical IG-treatment profiles. After reviewing current therapies, each profile was defined by mode of administration, frequency, location, number of needle sticks, and treatment duration. Before answering the choice questions, respondents were told to assume all treatments worked equally well. Choice questions were based on a D-efficient experimental design. Preference weights for attribute levels were estimated using random-parameters logit for each sample (adult patients and parents). Tests were performed to determine potential interactions among the administration attributes. All respondents provided online informed consent.
Results:
In total, 252 patients and 66 parents completed the choice questions appropriately. Overall, both groups preferred a home setting, monthly frequency, fewer needle sticks, and shorter treatment durations of IG treatment relative to alternative choices (p < 0.05). Mode of administration was the least important attribute to both samples; however, parents strongly preferred self-administration to an appointment with a healthcare professional (p < 0.05), whereas patients slightly preferred self-administration but were indifferent to the two modes.
Limitations:
Respondents evaluate hypothetical treatments and differences can arise between stated and actual choices.
Conclusions:
Considering the hypothetical treatments evaluated, IG treatments that provide the option of a home setting, monthly frequency, fewer needle sticks, and shorter treatment durations may address the needs of both patients and parents. Patients and parents have different preferences for administration attributes of IG treatments.
Introduction
Primary immunodeficiency (PI) constitutes a group of disorders involving a primary defect in the immune system. PIs are often described as rare disorders; although, due to the lack of worldwide screening for these diseases, the true incidence or population prevalence, either individually or in the aggregate, is not knownCitation1. A survey of 10,000 American households estimated the prevalence of diagnosed primary immunodeficiency to be 1 in 1200, or ∼250,000 people in the USCitation1. More than half of PIs are associated with inadequate or defective antibody production, caused by a lack of antibody-producing B-cells, B-cells that do not function properly, T-cell defects, or combined T-cell and B-cell defectsCitation2,Citation3. The four principal categories of therapy for different types of PIsCitation4 include Immunoglobulin G (IgG) replacement therapy, antimicrobial prophylaxis, bone marrow transplant, and gene therapy. However, the standard of care for many PI patients is IgG replacement therapyCitation4,Citation5 with the goal to protect the patient from life-threatening infections, prevent organ damage and infectious complications, prolong life, and improve health-related quality-of-lifeCitation3–6.
Individuals with antibody deficiency require lifelong treatment with immunoglobulin (IG), which can be administered intravenously or subcutaneously. While all IG products have to meet regulatory authorities’ requirements for preventing serious acute bacterial infections in PI patients, all IG products are not considered biosimilar or interchangeableCitation7. Multiple factors need to be considered in selecting an IG product, such as route of administration, volume load, rate of infusion, frequency of infusion, number of needle sticks, sugar content, stabilizer used, sodium content, osmolality, pH, and immunoglobulin A contentCitation8.
Given the continual progress that has been made in improving clinical outcomes for IG therapy, a recent editorial recommends ‘individualizing IG therapy to achieve freedom from infection in the diverse population of PI disorder patients’Citation9. This statement implies that understanding patient preferences for IG treatment can aid in achieving this goal. Several patient-reported outcome studies have reported that patients and parents of juvenile patients highly value improvements in the administration of IG treatmentsCitation10,Citation11. However, these studies do not provide any quantitative estimates for this statement. For example, Fasth and NyströmCitation10 conducted a quality-of-life assessment of parents who administered IG therapy at home to children with a PI. The study revealed that the most important dimensions of current treatments were features related to administration, not improved clinical outcomes. Moreover, this result may not be unique to PI and may apply to other chronic, immunological conditions that require frequent patient- or parent-administered treatments via an injection or a spray deviceCitation11. Because little is known about the relative importance to patients and parents and their willingness to accept trade-offs among IG treatment administration features or attributes, we designed a web-enabled choice-format conjoint survey to quantify patient and parent preferences for administration attributes of IG treatments. To answer which administration attributes are most important to specific users of IG treatments, we developed the following two null hypotheses: (1) all administration attributes are equal in importance to all users (patients and parents); and (2) patients and parents have similar preferences for administration attributes of IG treatments. The first hypothesis indicates that all attributes are equally important as the base scenario in the absence of quantitative data. The second hypothesis is important as we are eliciting preference information from users of IG treatments, which includes adult patients as well as parents who are responsible for administering the IG treatments to juvenile patients. The study of such preferences for administration attributes of IG treatments can provide important evidence to guide clinical decision-making and to promote patient-centered careCitation12.
Sample and methods
Study sample
Respondents were recruited from the Immune Deficiency Foundation (IDF) member panel. Potential study respondents received an e-mail invitation from IDF asking them to participate in the online survey. IDF did not provide patient contact information, and patient confidentiality was maintained by IDF throughout the study. All participating respondents were required to be a US resident at least 18 years of age with a self-reported physician diagnosis of a PI or the parent of a child with a PI. The 20-min online survey was administered in April 2011. All respondents provided online informed consent to participate in this study. This research was approved by RTI International’s Office of Research Protection and Ethics and has been performed in accordance with the 1964 Declaration on Helsinki and its later amendments.
Choice-format conjoint analysis
Choice-format conjoint analysis is a systematic method of eliciting trade-offs to quantify the relative importance patients assign to various treatment attributes or outcomes. It is based on the premise that treatments are composed of a set of attributes and that the attractiveness of a particular treatment to an individual patient is a function of these attributesCitation13–19.
Survey instrument
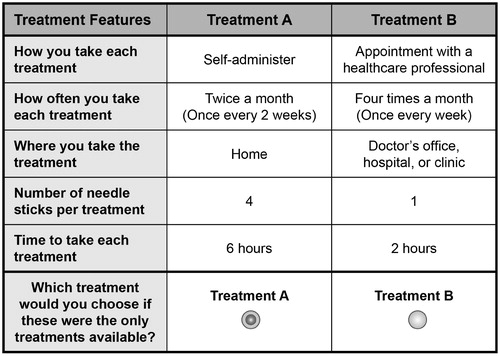
After review of the IG therapies, we identified the following five administration attributes that are common and of importance or relevance to patients and parents: mode of administration (self-administer or administration by a healthcare professional), frequency, location (home, doctor’s office, hospital or clinic), number of needle sticks per treatment and treatment duration (). These five attributes were described in respondent-friendly termsCitation20, and a survey instrument was developed following currently accepted best-practices.
Table 1. Attributes and levels for the choice questions.
Open-ended qualitative interviews (n = 9) were conducted with patients and parents in order to test the clarity of the survey instrument, the appropriateness of the descriptive information, and to confirm that the five administration attributes included in the survey were important to respondents and the respondents’ willingness to accept trade-offs among attributes in evaluating hypothetical treatments. During the interviews, respondents were asked to ‘think aloud’ as they completed a pencil-and-paper version of the draft survey instrument. After completing the survey in this manner, respondents were asked a series of debriefing questions to determine whether they understood the definitions and instructions, accepted the hypothetical context of the survey, and successfully completed the choice questions in the survey instrument as instructedCitation20. Using comments and feedback from the open-ended interviews, text changes were made to the survey to improve comprehension; and a web-enabled choice-format conjoint survey was designed.
Prior to answering the choice questions, respondents were asked to assume that (1) the treatments worked equally well and (2) all of their medical bills, including the cost of treatments and co-pays, were covered by health insurance. For each choice question in the survey, respondents were asked to indicate which of the two hypothetical treatments they would choose. Each hypothetical treatment was defined by varying levels of the five administration attributes (). The underlying experimental design that generated the choice questions utilized the D-efficient main-effects criterion and was constructed using SAS Version 9.2 (SAS Institute, Inc., Cary, NC)Citation21,Citation22, and led to a total of 36 choice pairs. The experimental design allowed for the estimation of main effects as well as interactions between frequency, duration, and number of needle sticks based on the findings from the open-ended qualitative interviews. The final experimental design consisted of three survey versions, each containing 12 choice questions (the order of the choice questions was randomized for each respondent). Each respondent was randomly assigned to one of the three versions.
Figure 1. Example choice question (patient version).
Statistical analysis
The responses to the choice questions were analyzed using random-parameters logit models for each sample (adult patients and parents), which controls for the panel structure of the data set and accounts for differences among individual preferences by estimating a normal distribution of heterogeneity for each preference parameterCitation23,Citation24. The dependent variable was respondents’ preferred treatment choice, and the explanatory variables included the levels of the attributes shown in . The choice models were estimated using NLOGIT 4.0 (Econometric Software, Inc., Plainview, NY). Statistical tests indicated that the two samples (adult patients and parents) could not be pooledCitation25,Citation26.
Specification tests determined that frequency, treatment duration, and number of needle sticks were linear, continuous variables. Mode of administration and location were modeled as effects-coded categorical variables, so that the parameter for the omitted category was the negative coefficient of the included categoryCitation25,Citation27. During the open-ended interviews, some respondents indicated that treatment duration or number of needle sticks per treatment did not matter to them as much as the total time spent or the total needles used in a given time period. We also hypothesized that preferences for treatment duration and number of needle sticks per treatment were affected by frequency. Thus, treatment duration and number of needle sticks were interacted separately with frequency in the choice models.
The resulting parameter estimates in quantify the relative preference weight of each attribute levelCitation20,Citation27. The vertical bars around each preference weight indicate the 95% confidence interval for that estimate. If the confidence intervals do not overlap for adjacent levels in a particular attribute, the mean estimates are statistically different from each other at the 5% level of significance.
Figure 2. Preference weights: Patients (n = 252) and parents (n = 66). The vertical bars surrounding each mean importance estimate denote the 95% confidence interval about the point estimate. If the confidence intervals do not overlap for adjacent levels in a particular attribute, the mean estimates are statistically different from each other at the 5% level of significance. Preference weights for the five attributes for patients and parents. Only relative differences matter when interpreting preference weights. The differences between adjacent weights indicate the relative importance of moving from one level of an attribute to an adjacent level of that attribute. The vertical distance between the best and worst level (that is, difference in the model coefficients) of each attribute is a measure of the overall mean relative importance of that attribute (over the ranges presented in the survey) to respondents.
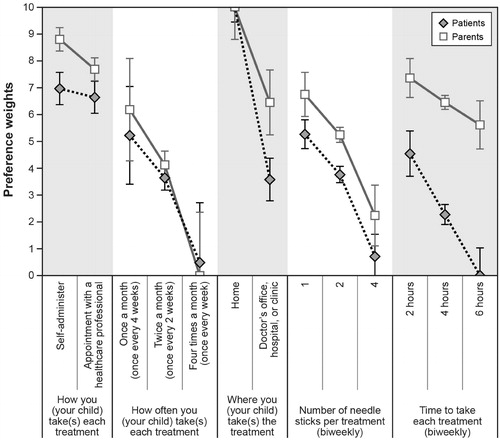
To facilitate the interpretation of the results and compare the two samples, we scaled the preference weights for each sample between 0–10, where the highest parameter (the best treatment attribute level, which was administration at home for both samples) was assigned a 10 and the lowest parameter (the worst treatment attribute level, which was a weekly treatment for parents and a 6-h treatment duration for patients) was assigned a 0. All other parameters were scaled between these two parameters. The vertical distance between the best and worst level (that is, difference in the model coefficients) of each attribute is a measure of the overall mean relative importance of that attribute (over the ranges presented in the survey) to respondentsCitation15,Citation18,Citation19.
Results
Sample characteristics
Email invitations were sent to 3000 existing IDF panel members to screen potential respondents to participate in the online survey. Of these, 470 panel members responded by clicking on the link to the survey (response rate = 16%), and 319 met the inclusion criteria (i.e., were eligible) and consented to participate in the survey. One patient had no variation in her responses to the choice questions (that is, she always chose Treatment A or Treatment B in each choice question) and therefore was excluded. The number of respondents in the final analysis was 252 patients and 66 parents.
The majority of patients were female (75%), married (68%), white (98%), and not working (53%); had common variable immunodeficiency disorder (87%), had received their IG treatment at home (60%), and had one needle stick per treatment (54%). The mean age of the patients was 50 years (SD = 14 years). The majority of parents were female (83%), married (86%), white (98%), and working (73%). The mean age of the parents was 44 years (SD = 7 years). The majority of juvenile patients had common variable immunodeficiency disorder (59%), self-administered treatment (56%), and received their IG treatment at home (77%). summarizes the demographics and baseline characteristics of the two samples.
Table 2. Demographics and baseline characteristics of the sample.
Preference weights
shows the scaled preference weights for the two samples. We found that the interaction between treatment duration and frequency was statistically significant and negative for both patients and parents (p < 0.05). This indicated that, as frequency of the treatment increased, the treatment duration became less preferred. This effect was more pronounced for adult patients. We also found a similar, statistically significant relationship for frequency and number of needle sticks for parents (p < 0.05), possibly indicating that parents were more concerned with the total number of needle sticks per month, which was a function of increased number of needle sticks per infusion and increased frequency. However, the interaction between frequency and number of needle sticks was not statistically significant for patients (p > 0.05), possibly indicating that patients were more concerned about the number of needle sticks used per treatment rather than about the total number of needle sticks used in a given month. Since preferences for treatment duration and needle sticks depended on a given level of frequency, in we present preference weights for treatment duration and needle sticks for an example case of a biweekly administration.
For both patients and parents, the estimated preference weights for all five administration attributes were consistent with the expected ordering of the categories; that is, better outcomes were preferred to worse outcomes. For example, number of needle sticks for a bi-weekly administration was naturally ordered: one stick had a higher preference weight than two sticks, and two sticks had a higher preference weight than four sticks (p < 0.05). presents five statistically significant results. First, both samples preferred monthly treatments to weekly treatments and bi-weekly to weekly treatments (p < 0.05). Second, both samples preferred home administration to a doctor’s office, hospital, or clinic (p < 0.05). Moreover, patients strongly preferred not to administer the treatment at a healthcare facility when compared with parents (p < 0.05). Third, preferences for adjacent levels for number of needle sticks (one, two, or four per treatment, assuming a bi-weekly administration) were statistically different from each other; as expected, both samples preferred fewer needle sticks (p < 0.05). These results held for weekly or monthly administration. As mentioned earlier, parents also cared about how many needle sticks were used in a total given time period; parents preferred fewer administrations and fewer needle sticks. However, patients were more concerned about the number of needle sticks per treatment.
Fourth, preferences for each treatment duration level per administration (2, 4, or 6 h, assuming a bi-weekly administration) were statistically different from each other; as expected, both samples preferred shorter treatment durations (p < 0.05). These results held for weekly or monthly administration. Patients were more averse to longer and more frequent administrations than parents. Fifth, parents preferred self-administration to administration by a healthcare professional (p < 0.05), whereas patients slightly preferred self-administration but were indifferent to the two modes (p > 0.05).
The vertical distance between adjacent preference weights in indicates the relative importance of moving from one level of an attribute to an adjacent level of that attribute. For example, the relative importance of a change for patients from administration at a healthcare facility to home administration was 6.5 (10 – 3.5). Similarly, the relative importance of a change from a weekly administration to a monthly administration was 4.5 (5 – 0.5). Therefore, the importance of a change from administration at a healthcare facility to home administration was 1.4-times as important (6.5 ÷ 4.5) for patients as a change from a weekly administration to a monthly administration. In contrast, the relative importance of a change for parents from administration at a healthcare facility to home administration was 3.6 (10 – 6.4). Similarly, the relative importance of a change from a weekly administration to a monthly administration was 6.2 (6.2 – 0.0). Therefore, the importance of a change from administration at a healthcare facility to home administration was 0.6-times as important (3.6 ÷ 6.2) for parents as a change from a weekly administration to a monthly administration. In terms of trade-offs, these results demonstrate how patients and parents have different preferences for administration attributes of IG treatments.
Overall relative importance of administration attributes
Given the range of levels of each attribute in the study, location was the most important attribute to patients. Frequency, number of needle sticks, and treatment duration were all almost equally important to patients. Number of needle sticks and treatment duration became more important as frequency increased. For parents, frequency was the most important attribute. Number of needle sticks and location were the next most important attributes, followed by treatment duration. Lastly, mode of administration was the least important attribute for both samples.
Discussion
To our knowledge, this is the first quantitative study using best practices for conjoint analysisCitation20 of patient and parent preferences for administration attributes of IG treatments in the US. The modeling of respondents’ answers to the choice questions yielded several important findings. Overall, both patient and parent samples indicated statistically significant preferences (p < 0.05) for monthly vs weekly administration, home setting vs doctor’s office/hospital/clinic, shorter vs longer treatment durations, and fewer needle sticks of IG treatment relative to alternative choices. The findings of this study suggest that administration attributes of IG treatment are relevant and important to patients and parents since IG treatment is a life-long therapy once initiated. Patients and parents may prefer to use an IG therapy that not only provides the clinical benefits they need but also provides the convenience to fit into their daily routine. Convenience attributes of IG therapy such as monthly frequency, ability to self-administer, and ability to schedule infusion at home could result in better adherence as these attributes may provide privacy, comfort, and the flexibility to schedule infusions around their work/school schedules. It has been reported that better medication adherence can have a positive impact on the clinical, economic, and humanistic outcomes. Findings in various therapeutic areas demonstrate increased medication adherence, resulting in reduced hospitalizations, nursing home admissions, physician visits, and avoidable healthcare costsCitation28–33.Therefore, any option in the IG therapy that could improve adherence can potentially impact these outcomes.
This study also sought to determine if patients and parents have similar preferences for administration attributes of IG treatments. For patients, location was the most important attribute of an IG treatment, whereas frequency was the most important attribute to parents. In addition, there were some significant differences between the patient and parent samples for treatment preferences (p < 0.05). The difference arose from respondents in each sample placing different values on the administration attributes, such as frequency, as well as from other, unobserved influences. Also, the importance of the administration attributes differed between the two samples. For example, for both samples, the value of treatment duration depended on frequency, implying that respondents cared about how many total hours in a month were spent administering the treatments, rather than just the duration of each treatment. Specifically, an increase (or decrease) in the frequency diminished (or increased) the value respondents placed on treatment duration. This effect was more prominent for patients. Interestingly, a comparative study between adult patients and parents involving device treatments for allergic rhinitis also found that changes in treatment duration were a significantly greater detriment to patients, who presumably placed a higher value on their timeCitation34. However, mode of administration was the least important attribute for both samples. Patients were almost indifferent to the levels for mode of administration. Parents valued self-administration, rather than administration by a healthcare professional (p < 0.05), but less than they valued improvements in any other treatment attribute. This indifference to the mode of administration in patients is consistent with results by Kittner et al.Citation35, which showed that some patients were not motivated to switch to self-administration of IG therapy for different reasons, despite its potential benefits. These findings generally reflect a difference in patients’ or parents’ willingness to allocate the total time of each month’s treatments among different frequencies and locations for administration. Adult patients, despite being more sensitive to the total time of each administration, have more autonomy in treating their conditions and are better able to substitute frequent administrations in exchange for a more preferable location. Parents have similar concerns, but are required to balance their child’s treatment requirements with other needs.
The results of this study are best interpreted with several issues and qualifications in mind. First, although choice-format conjoint methods are widely used in health economics to elicit preferences, assess health-related quality-of-life, and evaluate marketing strategies, the methods have limitations. One inherent limitation is that respondents evaluate hypothetical treatments. These constructed choice questions are intended to simulate possible clinical decisions but do not have the same clinical, financial, and emotional consequences of actual decisions. For example, we do not know whether real-world considerations such as insurance status or out-of-pocket costs will influence treatment decisions among these respondents. Thus, differences can arise between stated and actual choices. We have attempted to minimize such potential differences by offering alternatives that directly address our research question and mimic real-world trade-offs as closely as possible.
Furthermore, diagnosis among respondents in this study was self-reported and not confirmed by physician consultation or chart review. However, we believe the likelihood is small that patients without a PI (or parents of children without a PI) would complete a study such as this because the study is cognitively challenging and requires an investment in time in exchange for little personal gain. Finally, we recruited respondents through a patient group’s online member panel, which means that the sample used in this study is not necessarily representative of the patients in the US on IG therapy. It is possible that members of an advocacy group may be more highly motivated to obtain treatment at any cost.
Conclusion
In conclusion, choosing a lifelong IG therapy is a multi-faceted decision for PI patients and parents. IG treatments that provide the option of a home setting, monthly frequency, fewer needle sticks, and shorter treatment durations may address the needs of patients and parents alike. Factors specifically related to individual needs also should be considered, and this study identified several differences between patient and parent preferences that may provide useful information to guide clinicians in determining the best treatment for a specific patient. Future studies are needed to address how treatment preference can impact treatment compliance and outcomes.
Transparency
Declaration of funding
This study was funded by Baxter Healthcare Corporation. The views expressed herein do not necessarily reflect those of Baxter Healthcare Corporation.
Declaration of financial/other relationships
The authors declare that they have no competing interests. AFM and VK have no conflicts of interest to declare. Drs ML, RI, and JL-M have stock ownership in Baxter. As the supervisor for the study, AFM had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. The peer reviewers of this manuscript have disclosed that they have no relevant financial relationships.
Acknowledgments
The authors would like to thank the Immune Deficiency Foundation for their assistance in locating respondents who were interested in participating in this study, as well as the respondents who chose to participate in either the pilot study or the main study. The authors also would like to thank Paul Shannon and Stuart Yarr for programming the main study and Ryan Ziemiecki for his assistance in analyzing the data.
References
- Boyle JM, Buckley RH. Population prevalence of diagnosed primary immunodeficiency disease in the United States. J Clin Immunol 2007;27:497–502
- Immune Deficiency Foundation (IDF). Diagnostic & clinical care guidelines for primary immunodeficiency diseases. 2009. http://primaryimmune.org/wp-content/uploads/2011/04/IDF-Diagnostic-Clinical-Care-Guidelines-for-Primary-Immunodeficiency-Diseases-2nd-Edition.pdf. Accessed June 29, 2012
- Lindegren ML, Kobrynski L, Rasmussen SA, et al. Applying public health strategies to primary immunodeficiency diseases: a potential approach to genetic disorders. MMWR Recomm Rep 2004;53:1-29
- Bonilla FA, Bernstein IL, Khan DA, et al. Practice parameters for the diagnosis and management of primary immunodeficiency. Ann Allergy Asthma Immunol 2005;94:s1-s61
- Savides C, Shaker M. More than just infections: an update on primary immune deficiencies. Curr Opin Pediatr 2010;22:647-54
- Orange JS, Hossny EM, Weiler CR, et al. Use of intravenous immunoglobulin in human disease: a review of evidence by members of the Primary Immunodeficiency Committee of the American Academy of Allergy, Asthma and Immunology. J Allergy Clin Immunol 2006;117(4 Suppl):S525-53
- Siegel J. The product: all intravenous immunoglobulins are not equivalent. Pharmacotherapy 2005;25:78S-84S
- Gelfand EW. Differences between IGIV products: impact on clinical outcome. Int Immunopharmacol 2006;6:592-9
- Bonilla FA. IgG replacement therapy, no size fits all. J Clin Immunol 2011;2:107-9
- Fasth A, Nyström J. Quality of life and health-care resource utilization among children with primary immunodeficiency receiving home treatment with subcutaneous human immunoglobulin. J Clin Immunol 2008;28:370-8
- Crawford B, Dalal AA, Stanford R, et al. Validation of the Experience with Allergic Rhinitis Nasal Spray Questionnaire (EARNS-Q): a patient reported outcomes (PRO) questionnaire to measure experience and preference with nasal sprays. J Allergy Clin Immunol 2008;121(2 Suppl 1):S106
- Bridges J, Jones C. Patient based health technology assessment: a vision of what might one day be possible. Int J Technol Assess Health Care 2007;23:30-5
- Bridges JFP, Kinter ET, Kidane L, et al. Things are looking up since we started listening to patients: trends in the application of conjoint analysis in health 1982-2007. Patient 2008;1:273-82
- Mohamed AF, Epstein JD, Li-McLeod JM. Patient and parent preferences for haemophilia A treatments. Haemophilia 2011;17:209-14
- Mohamed AF, Hauber AB, Neary MP. Patient benefit-risk preferences for targeted agents in the treatment of renal cell carcinoma. Pharmacoeconomics 2011;29:977-88
- Johnson FR, Özdemir S, Mansfield C, et al. Crohn’s disease patients’ risk-benefit preferences: serious adverse event risks versus treatment efficacy. Gastroenterology 2007;133:769-77
- Johnson FR, Hauber AB, Özdemir S, et al. Are gastroenterologists less tolerant of treatment risks than patients? Benefit-risk preferences in Crohn’s disease management. J Manag Care Pharm 2010;16:616-28
- Hauber AB, Mohamed AF, Johnson FR, et al. Quantifying asthma patient preferences for onset of effect of combination inhaled corticosteroids and long-acting beta2-agonist maintenance medications. Allergy Asthma Proc 2009;30:139-47
- Hauber AB, Mohamed AF, Watson ME, et al. Benefits, risks, and uncertainty: preferences of antiretroviral-naïve African Americans for HIV treatments. AIDS Patient Care STDs 2009;23:29-34
- Bridges JFP, Hauber AB, Marshall D, et al. Conjoint analysis applications in health—a checklist: a report of the ISPOR Good Research Practices for Conjoint Analysis Task Force. Value Health 2011;14:403-11
- Kuhfeld W. Marketing research methods in SAS: experimental design, choice, conjoint, and graphical techniques. Cary, NC: SAS Institute Inc, 2010
- Kuhfeld W, Tobias F, Garratt M. Efficient experimental design with marketing research applications. J Mark Res 1994;31:545-57
- Train K. Discrete choice methods with simulation. Cambridge: CUP, 2003. p 138-54
- Train K, Sonnier G. Mixed logit with bounded distributions of correlated partworths. In: Scarpa R, Alberini A, ed. Applications of simulation methods in environmental and resource economics. Dordrecht: Springer Publisher, 2005. p 117-34
- Hensher DA, Rose JM, Greene WH. Applied choice analysis. Cambridge: CUP, 2005
- Louviere JJ, Hensher DA, Rose JM, et al. Stated choice methods: analysis and applications. Cambridge: CUP, 2000
- Bech M, Gyrd-Hansen D. Effects coding in discrete choice experiments. Health Econ 2005;14:1079-83
- American Pharmacists Association/APhA. Medication Compliance-Adherence Persistence (CAP) Digest. Washington, DC: American Pharmacists Association and Pfizer Pharmaceuticals, 2003. www.nhtsa.gov/people/injury/olddrive/druguse. Accessed March 29, 2012
- Balkrishnan R, Rajagopalan R, Camacho FT, et al. Predictors of medication adherence and associated health care costs in an older population with type 2 diabetes mellitus: a longitudinal cohort study. Clin Ther 2003;25:2958-71
- Dragomir A, Cote R, Roy L, et al. Impact of adherence to antihypertensive agents on clinical outcomes and hospitalization costs. Med Care 2010;48:418-25
- Gwadry-Sridhar FH, Manias E, Zhang Y, et al. A framework for planning and critiquing medication compliance and persistence research using prospective study designs. Clin Ther 2009;31:421-35
- Lau DT, Nau DP. Oral antihyperglycemic medication nonadherence and subsequent hospitalization among individuals with type 2 diabetes. Diabetes Care 2004;27:2149-53
- Sokol MC, McGuigan KA, Verbrugge RR, et al. Impact of medication adherence on hospitalization risk and healthcare cost. Med Care 2005;43:521-30
- Sheth K, Derebery J, Mahr T, et al. Ineffective control of allergic rhinitis symptoms reduces patient satisfaction and adherence with treatment. J Allergy Clin Immunol 2008;121:S106
- Kittner, J, Grimbacher B, Wulff W, et al. Patients’ attitude to subcutaneous immunoglobulin substitution as home therapy. J Clin Immunol 2006;26:400-5