
Abstract
Objective:
To perform a comparative long-term analysis of the associated healthcare costs for the therapeutic options in advanced Parkinson’s Disease (PD): deep brain stimulation (DBS), continuous duodenal levodopa-carbidopa infusion (CDLCI), and continuous subcutaneous apomorphine infusion (CSAI).
Methods:
Resource use associated with the pre-treatment period, procedure, and follow-up was assessed for the three therapies from the perspective of the Spanish national healthcare system. Resources consumption was measured with a Healthcare Resources Questionnaire (at nine advanced PD centres). Unit costs (Euro-Spain 2010) were applied to measure resource use to obtain the average total cost for each therapy over 5 years.
Results:
Mean cumulative 5-year cost per patient was significantly lower with DBS (€88,014) vs CSAI (€141,393) and CDLCI (€233,986) (p < 0.0001). DBS was associated with the lowest cumulative costs from year 2, with a yearly average cost of €17,603 vs €46,797 for CDLCI (p = 0.001) and €28,279 for CSAI (p = 0.008). For every patient treated annually with CDLCI, two could be treated with DBS (or €29,194 could be saved) and for every patient treated with CSAI, €10,676 could be saved with DBS. The initial DBS investment (32.2% of the total 5-year costs) was offset by decreases in anti-Parkinsonian drugs and follow-up costs. CDLCI and CSAI required constant drug use (i.e., levodopa and carbidopa for CDLCI, apomorphine for CSAI), representing ∼95% of their total 5-year cost.
Limitations:
All costs were based on a questionnaire, not on actual clinical data. The study is not a cost-effectiveness analysis as there is a lack of comparable outcomes data. An expert panel was used due to the complexity and variability in the treatment of advanced PD. The sample size was relatively small.
Conclusions:
Overall, DBS requires less use of health resources than CDLCI or CSAI in advanced PD patients, mostly pharmacological. The initial DBS investment was offset at year 2 by reductions in the ongoing consumption of anti-Parkinsonian medication. For every patient treated annually with CDLCI or CSAI, substantial cost savings could be made with DBS.
Introduction
Parkinson’s disease (PD) is a progressive neurodegenerative disorder of the central nervous system with motor, cognitive, behavioural, and autonomic symptoms. The number of individuals with PD over the age of 50 years in the world’s 10 most populous nations in 2005 was between 4.1–4.6 million and will double to between 8.7–9.3 million by 2030Citation1. In Spain, with a population of ∼47 million peopleCitation2 and considering the different incidence and prevalence rates publishedCitation3–6, the average incidence of PD has been estimated at ∼6400 new cases/year, and the average prevalence at 150,000 peopleCitation1. It is estimated that 30% of patients are in an advanced stage of the diseaseCitation7.
After the first 5 years from PD diagnosis, 40% of patients experience fluctuations and dyskinesias (difficulties with movement) despite best medical treatment, which increase in severity and frequency over timeCitation8. Additional treatment options to maintain symptom control are needed, but it can be challenging to achieve a medication regimen that keeps the patient mobile but does not create side-effects that impact the patient’s quality-of-life and outweigh the benefits of treatmentCitation9. In these advanced PD patients who are refractory to pharmacological treatment, the following three treatments are recommended: deep brain stimulation (DBS), continuous duodenal levodopa–carbidopa infusion (CDLCI), and continuous subcutaneous apomorphine infusion (CSAI)Citation10.
DBS is a medical device therapy in which a neurostimulator is connected to two leads inserted into the brain to provide electrical stimulation (i.e., bilateral stimulation of the subthalamic nucleus [STN], globus pallidus, or ventral intermediate thalamic nucleus). The stimulation modulates the signals responsible for the symptoms of PD, and can be non-invasively adjusted to meet patients’ needs. Unlike the other two therapies, DBS is supported by level I evidence. Overall, data have demonstrated a good long-term safety profile, significant improvement of motor symptoms and quality-of-life, and a reduction of daily ‘off’ time and dyskinesias when implanted in the STN in well-selected patientsCitation11–24. A reduction in oral drug treatment has also been foundCitation18,Citation23. CDLCI is a pharmacological/medical device combination therapy in which an external pump continuously delivers levodopa/carbidopa via a catheter inserted directly into the duodenum during the day (oral medication may be taken at night if required). This results in less variability in levodopa concentrations and is associated with fewer motor fluctuations and dyskinesias than oral levodopa administrationCitation24–26. CSAI is a pharmacological/medical device combination therapy that uses an external pump to subcutaneously administer apomorphine via intermittent bolus injection or continuous pump infusion, usually during the waking day hours (but sometimes at night if patients suffer from poor quality sleep or painCitation27). CSAI has shown efficacy in the reduction of ‘off’ episodesCitation24,Citation28–30. It is important to note that these three therapies are not necessarily equivalent treatments and therefore not recommended for all patients with advanced PD; one option may be preferable over another in specific clinical situations. Adequate patient selection allows the optimization of results obtained with the three therapeutic options. The three therapies have no clear positioning in the treatment pathway of advanced PD patients, leaving neurologists with the decision about each therapy’s suitability for their advanced PD patients. Beyond the patient’s clinical status, criteria supporting treatment decision-making include patients’ and physicians’ preferences, previous hospital experience, availability of the treatments, and treatment costs.
No comparative economic evaluation of the three treatment options exists. Cost-effectiveness analyses of these therapies are hindered by the lack of comparable outcomes data. Thus, this study was designed to address the gap in comparative economic data on the three treatment options to support payers and physicians in making treatment decisions for this patient population. The SCOPE (eStudio COstes Parkinson Enfermedad) study is a quantitative evaluation of the long-term (5 years) healthcare costs associated with the use of DBS, CDLCI, and CSAI in patients in advanced PD, from the perspective of the Spanish National Health System (NHS).
Methods
A comparative costing study was undertaken to assess the healthcare costs associated with the use of DBS, CDLCI, and CSAI in patients in advanced PD over a time horizon of 5 years, from the perspective of the Spanish NHS. Costs for the whole treatment period were considered, including: (1) costs of the pre-treatment/pre-operative period; (2) costs of the procedure/treatment administration; and (3) costs of follow-up (separately for up to month 6, and from 6 months onwards to 5 years). To measure the healthcare resources associated with therapies used in advanced PD, a protocol and a detailed Healthcare Resources Questionnaire (HRQ) (see below) were designed with input from a panel of Spanish advanced PD experts. A micro-costing approach was used to estimate the quantity of each health resource consumed.
In the management of chronic diseases such as PD, all the medium- and long-term costs should be considered along with the initial acquisition costs. In addition, the existing literature for DBS states that the average battery life of a non-rechargeable neurostimulator is 4–5 yearsCitation12,Citation31, at which point a new intervention to replace the neurostimulator is required. This time period was confirmed by the expert panel. Consequently, the time period of the study was set at 5 years, to take into account all of the medium- and long-term costs and a replacement cycle. According to recommendations for economic evaluations in SpainCitation32, both social and NHS perspectives are recommended. In the present case, considering the use of resources was taken from an expert panel of NHS clinicians and indirect costs cannot be assumed, it was decided that the perspective of the Spanish NHS was the most appropriate. Therefore, unit costs from the Spanish health resources database (Spanish Cost Database, e-saludCitation33) were assigned to the resource use identified to obtain the total cost for each of the three therapies for the 5-year period.
The SCOPE Study was evaluated and approved by the Ethics Committee of Clinical Research of the Hospital Clinic i Provincial, Barcelona.
Healthcare resources estimates
The main investigators, together with a panel of 11 experts from nine centres in five Spanish regions (Andalucía, Canarias, Cataluña, Comunidad de Madrid and Comunidad Valenciana) developed a research protocol and a detailed Healthcare Resources Questionnaire (HRQ). A panel of experts was included as there is an absence of advanced PD practice guidelines in Spain, and a panel is representative of the clinical judgements and practice variability in situations where no clinical guidelines existCitation34. Centres reported a minimum of 3-years’ experience in each technique. (It should be noted, however, that the length of experience varied between centres and also between treatments; two of the centres had more than 10 years of experience in DBS.) All experts also were specialists in the treatment of advanced PD patients with experience in at least two of the three therapies evaluated. Based on 2009 information, 217 advanced PD patients were estimated to be treated annually with these three therapies in the nine centres.
The HRQ was designed to collect healthcare resources associated with DBS, CDLCI and CSAI. Costs tend to be higher in the first 6 months after administration of the therapy, when patients consume more healthcare resources (extra visits, hospitalization, dose adjustments, etc.)Citation35–37. Consequently, it was decided to divide the HRQ into four sections: (1) pre-treatment/preoperative period; (2) procedure/treatment administration; (3) follow-up period from patient’s discharge to month 6; and (4) follow-up period from month 6 to year 5 (). For example, in the pre-treatment period, the HRQ contained questions on what type of specialist visits the patients underwent, need for hospitalization, and length of stay.
Table 1. Healthcare resources identified for every phase and for each therapy used to treat advanced Parkinson’s disease.
The experts were asked to answer the HRQ, on paper or via face-to-face interview, based on their experience and knowledge regarding the therapies, such that the quantitative information obtained would describe real clinical experience for the most frequent patient profile in the selected centres.
Due to the fact that treatment regimens in this patient population are characterized by high variability and complexity, making it difficult to capture drug use, the HRQ did not include direct questions regarding the baseline doses and details of consumption by patients of classical anti-Parkinsonian drugs (selegiline, rasigiline or amantadine, dopaminergic agonists, levodopa, and others). The changes in anti-Parkinsonian drug treatments and associated potential cost reductions or increases with the evaluated therapies were assessed in the HRQ. For each of the treatment phases, it was asked whether anti-Parkinsonian medication was reduced or increased and, if so, by what percentage. This information was then linked to the average drug cost per year for advanced PD patients for conservative (medical) treatment in Spain, as estimated in a published economic evaluationCitation38 for calculation of average drug costs over 5 years for each of the treatment options. The cost did not include that for apomorphine or levodopa/carbidopa.
Unit costs
Once all health resources associated with the therapies were identified and quantified, their cost per unit was obtained from the Spanish health resources database (Spanish Cost Database, e-saludCitation33). When more than one cost was found for a certain resource, the average value was used. In cases where no specific cost was found, experts were consulted in order to choose the cost of a similar resource. All the costs were expressed in Euro-Spain 2010Citation33.
The costs of the DBS neurostimulator and all of its components were included, provided by Medtronic (2010 costs). The costs of the devices and components for CDLCI and CSAI (infusion pump, catheters, etc.) were not included as their unit costs were not publicly available; thus it was assumed that they were provided free of charge by the supplier, and therefore their cost to the healthcare system was zero.
Following health economic evaluation guidelines and considering the duration of the analysis, which was longer than 1 year in this study, an annual discount rate of 3% was appliedCitation32 to convert the future expected costs into a present value amount.
Analyses
The data analysis was performed with the SPSS 15.0 software package for Windows. The non-parametric Kruskal–Wallis one-way analysis of variance by ranks was applied in order to test the statistical differences of mean costs among the three therapies (multiple comparisons)Citation39. The Mann–Whitney U-test was used in order to determine the statistical differences of mean costs among the two therapies with lower costsCitation39; for this reason, only statistical differences of average costs of DBS vs CSAI were obtained. A two-tailed probability level of 5% (p < 0.05) was considered significant. The analysis results are presented as mean ± standard error of the mean (95% confidence interval [CI]).
In order to obtain a more robust estimation of the costs, a bootstrap analysis was also performed using a sample size of 50 and a re-sample of 1000, calculating the main statistics expressed as median (mean; 2.5 percentile; 97.5 percentile).
Additionally to the main analysis, six different alternative scenarios were proposed to test the sensitivity of the results to the changes in some parametersCitation32 (). In scenarios 2, 3, and 5, the sensitivity of the results of the analysis was tested based on two values (min, max).
Table 2. Sensitivity analysis.
Results
Over 5 years, DBS required the greatest use of surgical and anaesthesia resources (as expected), but necessitated fewer medical visits than CDLCI or CSAI (). Fewer diagnostic tests were needed with CSAI compared with DBS or CDLCI. The unit costs of the healthcare resources included in the HRQ are shown in . shows the average cost per patient associated with the three alternative therapies in the baseline scenario for the four different phases. As expected, during the pre-treatment phase costs were similar for the three therapies. During phase 2 (procedure/treatment administration), DBS was associated with higher costs due to device acquisition and implant procedure cost. However, from discharge to 5 years follow-up, DBS was associated with significantly lower costs compared to CDLCI and CSAI (p < 0.0001). The costs for DBS were also significantly lower than CSAI for phases 3 (discharge from hospital to 6 months) (p = 0.023) and 4 (month 6 to year 5) (p < 0.0001). This suggests that, in the long-term, DBS is a less costly therapy vs CDLCI and CSAI. The yearly average cost of DBS was €17,603 compared to €46,797 for CDLCI (p = 0.001) and €28,279 for CSAI (p = 0.008). In fact, for every patient treated annually with CDLCI, two patients could be treated with DBS (or €29,194 could be saved) and for every patient treated with CSAI, €10,676 could be saved if DBS was chosen.
Table 3. Cumulative use of resources during the 5-year follow-up period (average values).
Table 4. Unit costs of healthcare resources included in the HRQ (€, 2010).
Table 5. Results of the baseline scenario expressed as mean ± standard error. Costs per patient (€, 2010).
DBS was associated with lower cumulative costs compared with CDLCI over the whole 5-year period (p < 0.0001) (). In addition, from year 2 there was a significant difference in costs between DBS and CSAI, in favour of DBS (p = 0.008). At year 5, the mean cumulative costs per patient for DBS amounted to €88,014 ± 2580, significantly lower than for CSAI (€141,393 ± 9945) and CDLCI (€233,986 ± 10,552) (p < 0.0001) (). For DBS, the high initial investment required during the first two phases (pre-treatment period to discharge; 32.2% of the total 5-year cost) was offset at the end of the first year when compared to CDLCI (p = 0.001) and from year 2 for CSAI comparison (p = 0.008), by decreases in anti-Parkinsonian pharmacological treatment and follow-up costs. The majority of the DBS costs were incurred within the initial 6 months. Around 95% of the total 5-year cost of CDLCI and CSAI was related to constant pharmacological costs, mainly acquisition costs for the levodopa-carbidopa intestinal gel cartridges (84.4%) and apomorphine ampoules (65.7%). In contrast, for DBS anti-Parkinsonian drugs represented only 43% of the total (). Results from the bootstrap analysis were very similar to the deterministic analysis ().
Figure 1. Cumulative annual costs for deep brain stimulation (DBS), continuous duodenal levodopa-carbidopa infusion (CDLCI), and continuous subcutaneous infusion of apomorphine (CSAI) (€, 2010). * All differences were statistically significant (p < 0.05) for multiple comparisons (among the three therapies) and for the DBS vs CSAI comparison (p < 0.05).
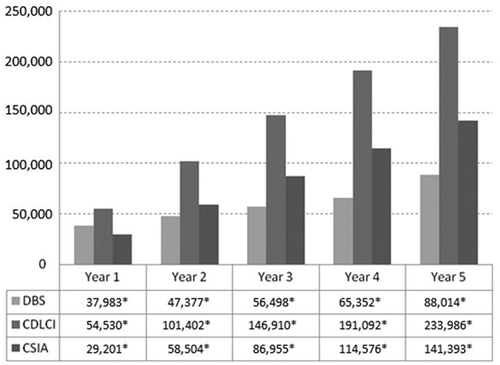
Figure 2. Costs distribution of deep brain stimulation (DBS), continuous duodenal levodopa-carbidopa infusion (CDLCI), and continuous subcutaneous infusion of apomorphine (CSAI) over the 5 year period (€, 2010).
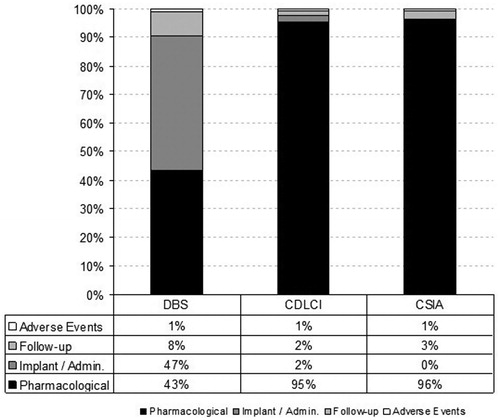
Table 6. Results of the bootstrap analysis.* Results are expressed as median (mean; 2.5 percentile; 97.5 percentile).
In the sensitivity analyses (scenarios outlined in ), DBS therapy was the least costly therapy compared to CDLCI and CSAI (p < 0.0001) for the three therapies comparison in both scenarios, even when considering different values for the costs of anti-pPrkinsonian drugs (p = 0.001 for DBS vs CSAI in scenario 1; p = 0.003 and p = 0.008, respectively, for the two DBS vs CSAI comparisons in scenario 2) (). In scenario 3, different discount rates were applied: by varying the discount rate from 0% to 5%, DBS proportionally remained the least costly therapy compared to CDLCI and CSAI (p < 0.0001 for the three therapies comparison; p = 0.008 for DBS vs CSAI). Considering a different battery replacement cycle for DBS, assuming a total of two battery replacements in the 5 year period in scenario 4, DBS remained the least expensive therapy compared to CDLCI and CSAI (p < 0.0001 for the three therapies comparison and for DBS vs CSAI). In scenario 5, the cost of new, differently-priced neurostimulators (either a rechargeable, dual channel implantable neurostimulator for DBS suitable for patients with high energy needs who are willing and able to keep their system recharged, or a smaller non-rechargeable, dual channel implantable neurostimulator for DBS suitable for patients with moderate energy needs) was considered. Even when this cost was taken into account, DBS remained the least expensive therapy (p < 0.0001 for the three therapies comparison and for DBS vs CSAI). In scenario 6, a progressive univariate reduction of CDLCI and CSAI drug acquisition costs was applied in order to achieve the breakeven point. Results showed that the drug acquisition cost of CDLCI must be reduced by 78.5% from its current value to obtain a similar 5-year cost to DBS. Considering CSAI, a 57.2% reduction in the price of apomorphine would bring the mean 5-year cost of CSAI to the same level as DBS (for example, the price of apomorphine ampoules must be ∼€13 instead of the current price of €30.4).
Table 7. Results of the sensitivity analysis (average ± standard error) (€, 2010). The results show 5-year total costs.
Discussion
This study is the first to compare the resource use and costs of DBS vs CDLCI and CSAI, the key three treatment options in advanced PD. It is also the only study in Spain to estimate the resources and costs related to advanced PD management with the three therapies. Results of the current evaluation show that, despite requiring an initial investment of 32.2% of the total cost, DBS was associated with the lowest costs during the whole 5-year period compared to CDLCI (p = 0.001) and from year 2 compared to CSAI (p = 0.008). During the total 5-year period, compared with the amount necessary to treat one patient with CDLCI, at least two patients could be treated if DBS was chosen (or €145,972 could be saved) and €53,379 could be saved vs treatment with CSAI. Comparison of costs over a 5-year period enabled the medium- and long-term costs associated with advanced PD to be captured; results show that the breakeven of the initial DBS investment occurred in the first and second year of treatment, respectively, when compared with CDLCI and CSAI.
The study did not include indirect costs, as the Spanish NHS perspective was selected. Pharmacological costs accounted for ∼95% of the total cost of CDLCI and CSAI, while for DBS they represented 43% of the total. These results were obtained considering one battery replacement in the 5-year period and without including acquisition costs for CDLCI and CSAI devices and components (infusion pump, catheters, etc.; only drug costs). If these costs had been included, results would have been even more favourable for DBS. The bootstrap analysis confirmed that the deterministic cost results were robust. Additionally, DBS showed the lowest costs in all the scenarios considered in the sensitivity analysis, even with the most unfavourable assumptions. Other alternative scenarios were tested in the sensitivity analysis: a second battery replacement during DBS therapy and a reduction of CDLCI and CSAI pharmacological costs. In all of these scenarios, DBS remained the least costly therapy.
Several published international economic evaluations of DBS conducted in other countries have applied different approaches, as presented in the review by Puig-Junoy & Puig Peiró.Citation40 which identified five cost studiesCitation35,Citation36,Citation41–43 and five complete economic evaluations of DBS compared to optimal medical therapyCitation37,Citation38,Citation44–46. As in our study, the evidence shows a reduction in medication costs associated with DBS.
Regarding the other two therapies, only one Swedish study from 2008 estimated the annual cost of CDLCICitation47. Cost estimates oscillated between €40,000 and €80,000 according to the dosage used. These results corroborate the CDLCI results of our study, as we observed an average drug cost of €44,839 per patient per year and the intestinal gel cartridges of CDLCI represented 84.4% of this total drug cost.
There are certain limits to the current study. For example, all costs were based on a questionnaire, not on actual clinical data. In addition, the study is not a cost-effectiveness analysis; however, cost-effectiveness analyses of these therapies are hindered by the lack of comparable outcomes dataCitation24, and the results of this study are the first step towards supporting payers and physicians in making treatment decisions for this patient population. Furthermore, the decision to use an expert panel (due to the complexity and variability in the treatment of advanced PD) may be considered a limitation. However, an expert panel can contribute to mapping complex treatment processes, and provide estimates of healthcare resourcesCitation44. It is worth mentioning that the 11 experts of the panel can be considered representative of the clinical practice of advanced PD in Spain, as both neurologists and neurosurgeons from nine centres located in five different Spanish regions were involved, with experience on at least two of the three therapies evaluated in this analysis. While clinical practice for treating PD might be different for settings outside Spain, it can be assumed to be similar enough for the significant results and large cost savings observed for DBS to be relevant across Europe. A further limitation is the relatively small sample size; nevertheless, all results were checked with non-parametric contrast hypothesis tests. For multiple comparisons, all results became statistically significant, except for the pre-treatment period to hospitalization. When statistical differences of mean costs among the two therapies with lower costs were compared, results showed that DBS became significantly less expensive than CSAI in year 2.
Conclusions
This study showed that DBS is the least costly therapy for advanced PD under the Spanish NHS perspective, compared to CDLCI and CSAI. The initial investment for the DBS implant is offset by a reduction in the consumption of other healthcare resources by patients over the years, resulting in the lowest cumulative costs over a 5-year period. For every patient treated annually with CDLCI or CSAI, substantial cost savings could be made with DBS. In contrast, CDLCI and CSAI require a more important and constant use of relatively similar health resources, with pharmacological costs being the main source.
Transparency
Declaration of funding
This research was funded by Medtronic International Sarl, Tolochenaz, Switzerland.
Declaration of financial/other relationships
FV received honoraria from Medtronic for this study and has received honoraria for lectures or advice from: Bohringer Ingelheim España, Abbot Laboratories (Manufacture and Commercialization of Duodopa [CDLCI]), Italfarmaco (Commercialization of Apomorphine [CSAI] in Spain), Medtronic Ibérica, UCB Pharmaceuticals and Novartis. JP-J received honoraria for consultancy from Medtronic for this study. RP-P received honoraria for consultancy from Medtronic for this study and participated in the study while working at the Centre for in Health and Economics (CRES), Universitat Pompeu Fabra, prior to joining the Office of Health Economics (OHE), London. OHE receives an annual conditional research grant from the Association of the British Pharmaceutical Industry (ABPI). The ABPI Code of Practice for the pharmaceutical industry regulates marketing of prescription medicines by companies based in the UK. Duodopa is produced and commercialized by Abbott, a member company of the ABPI. Abbott did not have any input in this study. The views expressed in this paper are those of the authors and are not necessarily those of either OHE or ABPI or Abbott. Neither OHE nor ABPI are in a position to endorse the findings of this report, which was funded by Medtronic Ibérica, S.A. Paloma González and Cristina Canal work for Medtronic Ibérica SA.
Acknowledgements
This paper was edited by an English-speaking professional medical writer, Deborah Nock (DPP-Cordell, Saxthorpe, UK), funded by Medtronic International Sarl, Tolochenaz, Switzerland.
References
- Dorsey E, Constantinescu R, Thompson J, et al. Projected number of people with Parkinson disease in the most populous nations, 2005 through 2030. Neurology 2007;68:384-6
- Population figures and demographic censuses. National Institute of Statistics, Spain, 2010. http://www.ine.es/inebmenu/mnu_cifraspob.htm. Accessed March 9, 2012
- Claveria L, Duarte J, Sevillano M, et al. Prevalence of Parkinson's disease in Cantalejo, Spain: a door-to-door survey. Mov Disord 2002;17:242-9
- Benito-Leon J, Bermejo-Pareja F, Rodriguez J, et al. Prevalence of PD and other types of parkinsonism in three elderly populations of central Spain. Mov Disord 2003;18:267-74
- Bergareche A, De La Puente E, Lopez de Munain A, et al. Prevalence of Parkinson's disease and other types of Parkinsonism. A door-to-door survey in Bidasoa, Spain. J Neurol 2004;251:340-5
- Abasolo-Osionaga E, Abecia-Inchaurregui L, Fernández-Díaz E, et al. The prevalence and pharmacological cost of Parkinson's disease in Spain. Rev Neurol 2006;43:641-5
- Kulisevsky J. Estimulación cerebral profunda en el tratamiento de la enfermedad de Parkinson: programa de actualización. 2nd edn. Profármaco, Barcelona, 2005
- Ahlskog JE, Muenter MD. Frequency of levodopa-related dyskinesias and motor fluctuations as estimated from the cumulative literature. Mov Disord 2001;16:448-58
- Adler C. Relevance of motor complications in Parkinson's disease. Neurology 2002;58(4 Suppl 1):S51-6
- Oertel W, Berardelli A, Bloem B, et al. Late (complicated) Parkinson's disease. In: Gilhus N, Barnes M, Brainin M, eds. European Handbook of Neurological Management: Volume 1. 2nd edn. Blackwell Publishing Ltd, 2011
- Silberstein P, Bittar R, Boyle R, et al. Deep brain stimulation for Parkinson's disease: Australian referral guidelines. J Clin Neurosci 2009;16:1001-8
- Krack P, Batir A, Van Blercom N, et al. Five-year follow-up of bilateral stimulation of the subthalamic nucleus in advanced Parkinson's disease. N Engl J Med 2003;349:1925-34
- Limousin P, Pollak P, Benazzouz A, et al. Effect on parkinsonian signs and symptoms of bilateral subthalamic nucleus stimulation. Lancet 1995;345:91-5
- Limousin P, Krack P, Pollak P. Electrical stimulation of the subthalamic nucleus in complicated parkinson's disease. N Engl J Med 1998;339:1105-11
- Rodriguez-Oroz M, Obeso J, Lang A, et al. Bilateral deep brain stimulation in Parkinson's disease: a multicentre study with 4 years follow-up. Brain 2005;128:2240-9
- Schüpbach W, Chastan N, Welter M, et al. Stimulation of the subthalamic nucleus in Parkinson's disease: a 5 year follow-up. J Neurol Neurosurg Psychiatry 2005;76:1640-4
- Pahwa R, Factor S, Lyons K, et al. Practice parameter: treatment of Parkinson disease with motor fluctuations and dyskinesia (an evidence-based review): report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology 2006;66:983-5
- Deuschl G, Schade-Brittinger C, Krack P, et al. A randomized trial of deep brain stimulation for Parkinson's disease. N Engl J Med 2006;355:896-908
- Østergaard K, Sunde N. Evolution of Parkinson's disease during 4 years of bilateral deep brain stimulation of the subthalamic nucleus. Mov Disord 2006;21:624-31
- Kleiner-Fisman G, Herzog J, Fisman DN, et al. Subthalamic nucleus deep brain stimulation: summary and meta-analysis of outcomes. Mov Disord 2006;21(14 Suppl):S290-304
- Gan J, Xie-Brustolin J, Mertens P, et al. Bilateral subthalamic nucleus stimulation in complicated parkinson's disease: three years follow-up. J Neurol 2007;254:99-106
- Weaver F, Follett K, Stern M, et al. Bilateral deep brain stimulation vs best medical therapy for patients with advanced Parkinson's disease. JAMA 2009;301:63-73
- Williams A, Gill S, Varma T, et al. Deep brain stimulation plus best medical therapy versus best medical therapy alone for advanced Parkinson's disease (PD SURG trial): a randomised, open-label trial. Lancet Neurol 2010;9(6):581-91
- Clarke C, Worth P, Grosset D, et al. Systematic review of apomorphine infusion, levodopa infusion and deep brain stimulation in advanced Parkinson's disease. Parkisonism Rel Disord 2009;15:728-41
- Antonini A, Isaias I, Canesi M, et al. Duodenal levodopa infusion for complicated parkinson's disease: 12-month treatment outcome. Mov Disord 2007;22:1145-9
- Samanta J, Hauser R. Duodenal levodopa infusion for the treatment of Parkinson's disease. Expert Opin Pharmacother 2007;8:657-64
- McGee P. Apomorphine treatment: a nurse's perspective. ACNR 2002;2:23-4
- Manson A, Turner K, Lees A. Apomorphine monotherapy in the treatment of refractory motor complications of Parkinson's disease: long-term follow-up study of 64 patients. Mov Disord 2002;17:1235-41
- Katzenschlager R, Hughes A, Evans A, et al. Continuous subcutaneous apomorphine therapy improves dyskinesias in Parkinson's disease: a prospective study using single-dose challenges. Mov Disord 2005;20:151-7
- Pietz K, Hagell P, Odin P. Subcutaneous apomorphine in late stage Parkinson's disease: a long term follow up. J Neurol Neurosurg Psychiatry 1998;65:709-16
- Bin-Mahfoodh M, Hamani C, Sime E, et al. Longevity of batteries in internal pulse generators used for deep brain stimulation. Stereotact Func Neurosurg 2003;80:56-60
- López Bastida J, Oliva J, Antonanzas F, et al. A proposed guideline for economic evaluation of health technologies. Gac Sanit 2010;24:154-70
- Health Sector Economic Information. Spanish Cost Database, e-salud. Oblikue Consulting, Spain, 2010. http://www.oblikue.com/bddcostes/. Accessed February 2010
- Simoens S. Using the Delphi technique in economic evaluation: time to revisit the oracle? J Clin Pharm Ther 2006;31:519-22
- McIntosh E, Gray A, Aziz T. Estimating the costs of surgical innovations: the case for subthalamic nucleus stimulation in the treatment of complicated Parkinson's Disease. Mov Disord 2003;18:993-9
- D'Ausilio A, Marconi S, Antonini A, et al. Cost analysis in Italy of various strategies for the treatment of Parkinson disease in the advanced phase. Recenti Prog Med 2003;94:484-93
- Tomaszewski K, Holloway R. Deep brain stimulation in the treatment of Parkinson's disease: a cost-effectiveness analysis. Neurology 2001;57:663-71
- Valldeoriola F, Morsi O, Tolosa E, et al. Prospective comparative study on cost-effectiveness of subthalamic stimulation and best medical treatment in advanced Parkinson's disease. Mov Disord 2007;22:2183-91
- Hollander M, Wolfe D. Nonparametric statistical methods. 2nd edn. Wiley Interscience, New York, NY, 1999
- Puig-Junoy J, Puig Peiró R. Review of the economic evidence on the use of deep brain stimulation in late stage Parkinson's disease. Neurologia 2009;24:220-9
- Gerzeli S, Cavallo M, Caprari F, et al. Analysis of deep brain stimulation (DBS) costs: an observational study on Italian patients. Pharmacoeconomics-Italian Research Articles 2002;4:66-79
- Charles P, Padaliya B, Newman A, et al. Deep brain stimulation of the subthalamic nucleus reduces antiparkinsonian medication costs. Parkisonism Relat Disord 2004;10:475-9
- Fraix V, Houeto JL, Lagrange C, et al. Clinical and economic results of bilateral subthalamic nucleus stimulation in Parkinson's disease. J Neurol Neurosurg Psychiatry 2006;77:443-9
- Spottke E, Volkmann J, Lorenz D, et al. Evaluation of healthcare utilization and health status of patients with Parkinson's disease treated with deep brain stimulation of the subthalamic nucleus. J Neurol 2002;249:759-66
- Meissner W, Schreiter D, Volkmann J, et al. Deep brain stimulation in late stage Parkinson's disease: a retrospective cost analysis in Germany. J Neurol 2005;252:218-23
- National Collaborating Centre for Chronic Conditions. Parkinson's Disease: national clinical guideline for diagnosis and management in primary and secondary care. Appendix F: 187–193. London: Royal College of Physicians, 2006
- Sydow O. Parkinson's disease: recent development in therapies for advanced disease with a focus on deep brain stimulation (DBS) and duodenal levodopa infusion. FEBS J 2008;275:1370-6