
Abstract
Objectives:
More than 1.5 million patients worldwide are affected by bone metastases. Patients with bone metastases frequently develop skeletal-related events (SREs, including radiation to bone, non-vertebral fracture, vertebral fracture, surgery to bone, and spinal cord compression) that are associated with high healthcare costs. This study aims to provide an estimate of the cost per SRE in both the inpatient and outpatient settings in Belgian patients with bone metastases secondary to solid tumors (breast, prostate, and lung cancers).
Methods:
Patients were retrieved from the IMS Hospital Disease database from 2005–2007. Inclusion was based on the International Classification of Diseases and Related Health Problems Version 9 (ICD-9) diagnosis and/or procedure codes covering patients with breast, prostate, or lung cancer with bone metastases who were hospitalized for one or more SREs. All costs were extrapolated to 2010 using progression in hospitalization costs since 2001. Additional outpatient costs resulting from radiation to bone and diagnostic tests performed in ambulatory settings were estimated by combining published unit costs with resource use data obtained from a Delphi panel.
Results:
The average cost per SRE across solid tumor types based on the weighted average of inpatient and outpatient costs was €2653 for radiation to bone, €5015 for a vertebral fracture, and €7087 for a non-vertebral fracture. Costs were €12,885 and €15,267 for surgery to bone and spinal cord compression, respectively.
Limitations:
No patient follow-up across calendar years could be done. Also, details regarding the exact anatomic sites of SREs were not always available.
Conclusions:
SREs add a substantial cost to the management of patients with bone metastases. Avoiding SREs can lead to important cost-savings for the healthcare payer.
Introduction
Bone metastases occur when cancer cells separate from the initial tumor and migrate to bone tissue where they settle and grow. More than 1.5 million patients worldwide are affected by bone metastasesCitation1.
While any type of cancer is theoretically capable of forming metastatic tumors within the bone, the incidence of bone metastases is highly cancer-specific. In particular, breast, prostate, and lung cancers show a predilection to metastasize to the bone. Cumulative incidence rates of bone metastases as high as 75% have been observed in patients with advanced breast and prostate cancerCitation2,Citation3, while incidence rates between 15–40% are reported in lung cancer patientsCitation4,Citation5.
Bone metastases are usually associated with severe bone pain and frequently result in skeletal-related events (SREs), which include pathologic fracture, radiation, or surgery to bone to treat or prevent a fracture, and spinal cord compressionCitation6–9.
In the placebo arms of four clinical trialsCitation10–13, 46–64% of untreated subjects with advanced solid tumors or multiple myeloma and bone disease experienced at least one on-study SRE. The follow-up period was 21–24 monthsCitation10–13. Across all primary cancers, the most common SRE types were radiation to bone (34–43%) and pathologic fracture (22–52%). Surgery to bone and spinal cord compression occurred less frequentlyCitation10–13.
Recently published results of an international prospective study showed that SREs are associated with high healthcare use, since their management often requires prolonged inpatient stays and the use of expensive procedures on top of intense use of outpatient resourcesCitation14. Recent publications described the economic burden associated with SREs in EuropeCitation15,Citation16, but health resource utilization (HRU) or costs associated with SREs in a Belgian healthcare setting have not been reported. This study aims to provide an estimate of the average cost associated with each SRE type in Belgian patients with bone metastases secondary to female breast, prostate, or lung cancer using the Belgian Hospital Disease Database. This database, validated by numerous publicationsCitation17–20, constitutes a unique source of information since it provides complete data on diagnoses, treatments, and inpatient costs in 34% of all hospital beds in Belgium (comparable databases are currently available only in Sweden and the UK). Costs are estimated from the total health care payer’s perspective, i.e., the cost covered by the Belgian National Health Insurance (INAMI/RIZIV) and the patient co-payment.
Methods
SRE definition and type of costs included
Five categories of SREs were defined in the context of this study: pathologic vertebral fractures, pathologic non-vertebral fractures, radiation to bone, surgery to bone, and spinal cord compression. Radiation to bone encompassed both radiation to bone administered for pain control (including use of radioisotopes) and radiation to bone to prevent a fracture. Surgery to bone included procedures performed to stabilize the bone and those to prevent an imminent fracture or spinal cord compression. The estimation of the average total cost is based on the inpatient hospitalization cost and the costs related to the consumption of outpatient resources.
Inpatient hospital costs: retrospective database study
Inpatient costs were obtained from a single country (Belgium), retrospective database study of adult patients (>20 years old) with bone metastases secondary to breast, prostate, or lung cancer. Patients were hospitalized in 2005–2007 with a diagnosis of bone fracture or spinal cord compression or were hospitalized to undergo radiation to bone or surgery to bone. The source of information was the Hospital Disease Database, a database owned by IMS Health. Since 1991, Belgian hospitals have to register case mix data for each admission in a minimum basic data set (MBDS) to receive reimbursement from the authorities. The MBDS contains data on patients’ basic demographics as well as on diagnosed conditions and medical procedures (International Statistical Classification of Diseases and Related Health Problems Version 9 [ICD-9] diagnosis and/or procedure codes). The MBDS are captured via a trusted third party, which standardizes and streamlines the data. Then, a sub-set of the national database, consisting of the hospitals that have given written authorization to do so, is anonymized (on both hospital and patient level) and transmitted to IMS Health. Thus, the database comprises data for ∼34% of all Belgian hospital beds for 2005–2007. The panel of hospitals is representative for Belgium in terms of geographical dispersion, hospital size, and type of centres (general hospital vs academic hospitals).
Data are recorded at the level of the hospital stay, either in a day clinic setting (no overnight stay) or full hospitalized setting. For each stay a unique identification number is assigned. These data comprise the length of stay, the ICD-9 diagnoses and procedure codes, the type of admission, the length of stay in the different service provider settings, and the type of discharge. A list of all drugs invoiced to the patient’s sickness fund or health insurance over the course of the stay (number of units, dose, and cost) is available as well. The database also comprises demographic data at the patient level (age range, gender).
All inpatient stays related to the same patient can be tracked by a unique patient identification number attributed at the beginning of each calendar year.
The hospitalization costs consist of three components: drug cost, room/bed cost, and procedure costs. Drug costs were extracted directly from the database. Room/bed costs and procedure costs were obtained by merging resource use (number of stays with eligible diagnosis codes) from the database with average costs per APR-DRG (All Patient Refined-Diagnosis Related Groups) and severity as calculated from the financial data files that all the Belgian hospitals are legally required to send twice a year to the Belgian authorities and are published on their websiteCitation21. All costs, except for drug costs, were extrapolated to 2010 using progression in hospitalization costs since 2001.
The search criterion to identify eligible patients from the database was the combination of the ICD-9 diagnosis code corresponding to bone metastasis and the code corresponding respectively to breast, prostate, or lung cancer. Hospital stays related to SREs were identified based on specific ICD-9 diagnosis and/or procedure codes listed in .
Table 1. List of ICD-9 diagnosis and procedure codes.
The scope of this analysis was to estimate the average cost per SRE type. As SREs frequently occur as a sequence of multiple events, the following methodology was chosen to ensure that the average cost per single type of SRE would reflect the complexity of all possible real-life combinations.
The hospital stay where the SRE occurred was defined as the stay related to the index SRE. SRE-related stays registered during the same month were assumed to be related to the index SRE. Consequently, their costs were assigned to the index SRE. Multiple events occurring during the same stay or during the same month as the index SRE were considered to be clustered events. The definition of a clustered event was based on medical relevance. For instance, the event radiation to bone consists of radiation to bone followed by a fracture (vertebral vs non-vertebral) and other radiation to bone. Similarly, surgery to bone events encompass surgery applied to vertebrae, surgery applied to non-vertebrae, and surgery to unknown site (when no fracture codes were found that allowed identifying the fracture site; in most of the cases, these corresponded to preventive surgery, i.e., surgery without a pre-existing fracture). Equally, bone fractures were split between fractures leading to surgery and fractures not leading to surgery, depending on the occurrence of surgery to bone within the month of the fracture. Spinal cord compression was assumed to be a single event, superseding any other SRE occurring within the same calendar month. In case an event qualified for more than one type of clustered SRE, the most cost-driving SRE was assumed to be the index. For instance, if multiple clustered SREs within one calendar month included a spinal cord compression, the event was labelled spinal cord compression. If multiple clustered events included both surgery to bone (with or without fracture) and radiation to bone, the event was labelled as surgery to bone, and radiation to bone was assumed to be part of the event surgery to bone. Based on this algorithm, the following set of nine mutually exclusive clustered events were defined:
Vertebral fracture without surgery to bone (and without radiation to bone);
Non-vertebral fracture without surgery to bone (and without radiation to bone);
Vertebral fracture followed by surgery to bone (with or without radiation to bone);
Non-vertebral fracture followed by surgery to bone (with or without radiation to bone);
Surgery to bone to unspecified site/preventive surgery to bone (with or without radiation to bone);
Radiation to bone without fracture (without surgery to bone);
Radiation to bone with vertebral fracture (without surgery to bone);
Radiation to bone with non-vertebral fracture (without surgery to bone); and
Spinal cord compression (with or without radiation to bone or surgery to bone).
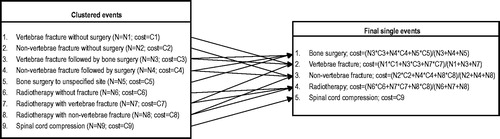
First, the average inpatient cost was calculated for each of the nine clustered events. Second, these clustered events were divided into their single event components (vertebral fracture, non-vertebral fracture, radiation to bone, surgery to bone, and spinal cord compression) using the algorithm depicted in . For example, the cost of the SRE, ‘bone surgery’, was the result of the weighted average of the costs of the clustered events vertebral fracture followed by bone surgery, non-vertebral fracture followed by bone surgery, and bone surgery to unspecified site.
Figure 1. Algorithm used to distribute clustered events into single-label SREs.
Outpatient costs: Delphi panel
Some SREs, e.g., radiation to bone and pathologic fracture, may not always require hospitalization. Some patients may receive outpatient radiation to bone as the sole interventional treatment for their fracture.
A Delphi panel was conducted consisting of seven oncologists and radiotherapists with expertise in the management of patients with bone metastases. The objective of the panel was to derive the proportion of patients receiving radiation to bone in the outpatient setting. Additionally, the panel derived the proportion of patients undergoing ambulatory diagnostic tests. Information from the Delphi panel was essential since the hospital disease database does not contain data on the outpatient setting.
SRE costs based on inpatient hospital costs and outpatient costs
The average costs for the SREs, ‘radiation to bone’ and ‘pathologic fracture’ were the result of the weighted average of inpatient costs (as calculated from the hospital disease database) and outpatient costs (as calculated from information provided by the expert panel). For patients undergoing surgery to bone or those with spinal cord compression, it was assumed that radiation to bone was performed during their hospitalization and, thus, in an inpatient setting. The cost of radiation to bone, if occurring, would therefore already be included in the observed inpatient costs. The costs of outpatient diagnostic tests were considered an additional cost for all categories of SREs.
Results
Inpatient SRE cost
A total of 1268 clustered SREs requiring hospitalization were found in the database (443 in breast cancer patients, 265 in prostate cancer patients, and 560 in lung cancer patients). The most common clustered SRE was pathologic fracture without surgery (47.2% and 23.3%, respectively, for vertebral and non-vertebral fractures). Lowest sample sizes were observed for spinal cord compression (1.7%; n = 21) and radiation to bone with fracture (0.4%; n = 5 for both radiation to bone with vertebral fracture and radiation to bone with non-vertebral fracture).
When calculating the inpatient cost of the clustered events, one case of radiation to bone with a vertebral fracture in a patient with prostate cancer was removed from the analysis as the associated costs were assumed to be an outlier (€105,650). After this correction, the most costly clustered inpatient event remained radiation to bone with vertebral fracture (€18,401). Spinal cord compression (€15,048), and vertebral fracture with surgery to bone (€14,417) were the next most costly SREs. The least costly clustered inpatient events were radiation to bone without a fracture (€5817) and surgery to bone to unspecified site, including preventive surgery to bone (€7794) (). The inpatient cost per SRE type varied between €6393 for radiation to bone (n = 149) and €15,048 for spinal cord compression (n = 21) ().
Table 2. Average inpatient cost per clustered event across solid tumors.
Table 3. Calculation of total average cost per SRE across solid tumors.
Outpatient radiation to bone cost
Based on the information from the Delphi panel, among the patients receiving radiation to bone, the proportion initiating it in the outpatient setting was 72.8%, 72.8%, and 55.4% for patients with breast, prostate, and lung cancer, respectively. Across all solid tumors, this percentage was 64.8%. For the SRE ‘radiation to bone’ we applied the fixed cost of €612.75 corresponding to 1–10 sessions of radiation to bone to these proportions of patients ().
According to the experts, the percentage of patients with fractures (vertebral or non-vertebral) receiving radiation to bone was 65.3%, 86.0%, and 78.2%, respectively, for breast, prostate, and lung cancer. The percentage of patients with fractures was 79.6% across all solid tumors. By multiplying these percentages with the respective proportions of patients receiving radiation to bone in an ambulatory setting, the proportion of patients having a fracture that are only treated with outpatient radiation to bone could be calculated (i.e., 47.6%, 62.6%, and 43.3%, respectively, for breast, prostate, and lung cancer). The proportion across all solid tumors (49.31% for vertebrae fractures and 48.14% for other fractures) was obtained by weighting these proportions per tumor type with the number of events observed in the database. In order to calculate the weighted cost for the SRE, ‘pathologic fracture’, the proportions of patients that receive outpatient radiation to bone were taken into account ().
Additional cost of ambulatory diagnostic tests
The Delphi panel also estimated the percentage of patients per tumor type and SRE type who underwent ambulatory diagnostic tests, i.e., radiography (unit cost = €13.76), computed tomography (CT)-scan (€49.14), magnetic resonance (€49.14), bone scan (€112.2), and positron emission tomography (PET)-CT (€177.76) (). The additional cost per tumor type and SRE type due to outpatient diagnostic tests was obtained by multiplying the unit costs with these proportions (). All costs were considered from the public payer perspective.
Table 4. Estimated percentage of patients undergoing ambulatory diagnostic tests.
Average cost per SRE
The average cost per single SRE type across all solid tumor types was estimated to be €5015 for a vertebral fracture, €7087 for a non-vertebral fracture, €15,267 for spinal cord compression, €12,885 for surgery to bone, and €2653 for radiation to bone ().
Discussion
Patients with bone metastases secondary to advanced malignancies can experience burdensome SREs such as pathologic fracture, spinal cord compression, or the need for surgery or radiation to bone. These skeletal complications can have devastating clinical consequences for the patient. While it is generally known that SREs are associated with high healthcare costs, European-specific data are rather scarce and no specific cost estimates have been made available so far for Belgian patients. Given the prevalence of breast, prostate, and lung cancer, the economic burden associated with SREs is significant. Utilization of treatments to prevent SREs may reduce the associated economic burden. In this study, a hospital disease database comprising of a representative panel of Belgian hospitals was used to estimate inpatient SRE costs. Outpatient costs are not available from the database, and outpatient radiation to bone and ambulatory diagnostic test costs were derived from a Delphi panel and were included in the overall costs. Each SRE type is associated with a considerable cost to the healthcare system. The average cost per SRE type across solid tumor types in Belgium, based on the weighted average of inpatient and outpatient costs, was €2653 for radiation to bone, €5015 for a vertebral fracture, and €7087 for a non-vertebral fracture. Costs for SREs of surgery to bone and spinal cord compression were €12,885 and €15,267, respectively.
SREs are part of complex disease progression and may occur as a sequence of multiple events that partly overlap. This study developed a composite view of each SRE, thus better reflecting what is occurring on a patient level while also maintaining a clear focus on cost estimates per SRE type. This was achieved by analyzing the costs for each clustered event and, in a second step, estimating the costs for the separate SRE types based on the weight of the specific clustered events that are composed of the single SRE types. For example, the cost of surgery to bone is the result of the weighted average of the cost of surgery to bone after a fracture and surgery to bone without a fracture. This may result in more reliable cost estimates.
Most of the published studies on the cost of SREs are observational studies based on limited samples. In contrast, this retrospective study was conducted using a database covering 34% of all the hospital beds in Belgium, potentially providing a more representative sample of the whole population.
Common to all studies using database records, some data that may impact the cost of SREs were not available in the database as, for example, outpatient costs. Due to the lack of observational data, these costs were derived by a Delphi panel. The use of a Delphi panel to collect the outpatient data that were not available elsewhere constitutes a potential weakness in our study. Consensus methods, such as the Delphi technique, are not ranked high within the hierarchy of data sources in evidence-based medicine. The guidelines for pharmaco-economic studies published by the Belgian Health Care Knowledge Centre (Kenniscentrum–KCECitation22) state that expert panels should be used only in cases where insufficient observational data are available; the expert panel should be representative and, in this particular case, representativeness would be based on the quality of the expert panel rather than on the number of expertsCitation23. In our study, seven experts (six oncologists and one radiotherapist) with confirmed expertise in managing patients with bone metastasis consecutive to breast, lung, and prostate cancers replied to a one-round questionnaire, followed by a debriefing phone call. The most important information derived from the Delphi panel was the percentage of patients treated only with radiotherapy and this in the outpatient setting. This percentage was used to calculate the total cost per SRE as a weighted average of inpatient and outpatient costs. Should this percentage have been over-estimated, the true total cost would lie closer to the inpatient cost; in the opposite case, the total cost would be somewhat lower than reported.
A limitation associated with the cost calculations was that some of the hospitalization costs that were identified by ICD codes may not accurately represent an inpatient stay associated with a SRE. To minimize potential bias, we excluded specific and easily identifiable cost elements that were attributable to the underlying cancer from our calculation (e.g., the cost of chemotherapy plus its administration cost). A conservative approach was taken when defining the categories of out-patient costs to be included in the calculation; only the cost of ambulatory radiation to bone and the cost of associated diagnostic tests were taken into account, costs associated with visits to the oncologist were excluded. In the case where an SRE qualified for more than one category of clustered events, the event was attributed to the most cost-driving category of clustered events. After identifying and removing a visible outlier, the mean cost estimates did not change substantially for the majority of the SRE types; however, cost estimates based on only a few cases should be seen with caution.
Although we defined a method to assign a subsequent event to the index SRE, it may not always have been entirely accurate, since details with regards to the exact anatomic sites involved were not always available. Also, since the database uses unique patient identification numbers that may change at the beginning of each calendar year, patients cannot always be easily followed across years. Furthermore, the database does not specify exact dates but only the month of patient’s discharge from the hospital is available; as a consequence, the clustering of events is done per calendar month instead of applying a fixed window period around the index event.
It should be noted that the total number of the SRE type ‘radiation to bone’ reported in this study was lower than that which might be observed in a purely epidemiological study. This was anticipated given the algorithm used to define the clusters. Also the ICD-9 code list used to identify ‘bone surgery’ and ‘spinal cord compression’ was restricted compared with other published studiesCitation24. However, the possible under-estimation of the number of cases for these SREs was not considered an issue since a sensitivity analysis using an extended ICD-9 list demonstrated that it did not significantly impact the cost estimate. Indeed, the extension of the list of codes yielded final average costs per SRE that were comparable (a decrease of ∼10%—from €15,267 to €13,708—in spinal cord compression and an increase of ∼6%—from €12,885 to €13,673—in bone surgery).
Other studies estimating SRE costs vary in study design, and the use of country-specific unit costs makes it difficult to directly draw conclusions from a cross-country comparison. In a recent prospective observational study conducted in Canada, Germany, Italy, Spain, the UK, and the USCitation15, in order to estimate the cost of SREs in patients with bone metastasis consecutive to solid tumors, data were collected by chart review in ∼250 patients per country. A comparison with our results shows that cost estimates in Belgium are higher than in other European countries (e.g., for ‘surgery to bone’, the estimate is more than 3-times the highest cost observed in other European countries), except for ‘vertebral fractures’, where the cost lies in the mid-range. A possible explanation lies in the variability of medical practice and costing methods within the different healthcare systems; for instance, a comparison between hospitalization costs per pathology respectively in BelgiumCitation21 and the UK for 2009Citation25 shows that hospitalization costs in Belgium are consistently higher across pathologies, notably due to longer length of stays in Belgian hospitals. This is in line with the figures published by the World Health Organization showing that the average cost per day in hospital (including all pathologies) is higher in Belgium than in Spain (+30%), Italy (+11%) and Germany (+5%)Citation26. However, in line with published dataCitation15,Citation16, this study showed that the SREs ‘surgery to bone’ and ‘spinal cord compression’ are considerably more costly than the SREs ‘radiation to bone’ and ‘pathologic fracture’.
Conclusion
The costs associated with SREs are significant from a payer’s perspective. The present study used a hospital database to estimate cost of SREs in an inpatient setting in Belgium and supplemented it with outpatient costs derived from a Delphi panel. This study provides an estimate of the costs associated with SREs in the Belgian healthcare system that is helpful to payers to quantify the economic burden of SREs in patients with bone metastases secondary to solid tumors. SREs place a substantial burden on patients with advanced tumors and on the healthcare system.
Transparency
Declaration of funding
Funding for this study was provided by Amgen Belgium.
Declaration of financial/other relationships
IMS Health, employer of PC and ML, received honoraria for data management and analyses. J-JB serves as a consultant for Amgen and Novartis, HG and OG are Amgen employees and own stocks in the company.
Acknowledgments
Editorial support was provided by Emma Thomas and Sarah Petrig from Amgen (Europe) GmbH.
References
- Capanna R, Coia LR, Coleman R, et al. editors. Textbook of Bone Metastases. Hoboken, NJ: John Wiley and Sons; 2005. p 105
- Rubens RD, Coleman RE. Bone metastases. In: Abeloff MD, Armitage JO, Lichter AS, et al., editors. Clinical oncology. New York: Churchill Livingstone; 1995. p 643-65
- Crump M, Gluck S, Tu D, et al. Randomized trial of high-dose chemotherapy with autologous peripheral-blood stem-cell support compared with standard-dose chemotherapy in women with metastatic breast cancer: NCIC MA.16. J Clin Oncol 2008;26:37-43
- Coleman RE. Clinical features of metastatic bone disease and risk of skeletal morbidity. Clin Cancer Res 2006;12:6243s-9s.
- Sugiura H, Sugiura T, Mitsudomi T. Predictors of survival in patients with bone metastasis of lung cancer. Clin Orthop Relat Res 2008;466:729-36
- Rosen LS, Gordon D, Kaminski M, et al. Zoledronic acid versus pamidronate in the treatment of skeletal metastases in patients with breast cancer or osteolytic lesions of multiple myeloma: a phase III, double-blind, comparative trial. Cancer J 2001;7:377-87
- Henry D, Costa L, Goldwasser F, et al. Randomized, double-blind study of denosumab versus zoledronic acid in the treatment of bone metastases in patients with advanced cancer (excluding breast and prostate cancer) or multiple myeloma. J Clin Oncol 2011;29:1125-32
- Stopeck AT, Lipton A, Body J-J, et al. Denosumab compared with zoledronic acid for the treatment of bone metastases in patients with advanced breast cancer: a randomized, double-blind study. J Clin Oncol 2010;28:5132-9
- Fizazi K, Carducci M, Smith M, et al. Denosumab versus zoledronic acid for treatment of bone metastases in men with castration-resistant prostate cancer: a randomised, double-blind study. Lancet 2011;377:813-22
- Lipton A, Theriault RL, Hortobagyi GN, et al. Pamidronate prevents skeletal complications and is effective palliative treatment in women with breast carcinoma and osteolytic bone metastases: long term follow-up of two randomized, placebo-controlled trials. Cancer 2000;88:1082-90
- Saad F, Gleason DM, Murray R, et al. Long-term efficacy of zoledronic acid for the prevention of skeletal complications in patients with metastatic hormone-refractory prostate cancer. J Natl Cancer Inst 2004;96:879-82
- Berenson JR, Lichtenstein A, Porter L, et al. Long-term pamidronate treatment of advanced multiple myeloma patients reduces skeletal events. Myeloma Aredia Study Group. J Clin Oncol 1998;16:593-602
- Rosen LS, Gordon D, Tchekmedyian NS, et al. Long-term efficacy and safety of zoledronic acid in the treatment of skeletal metastases in patients with nonsmall cell lung carcinoma and other solid tumors: a randomized, phase III, double-blind, placebo-controlled trial. Cancer 2004;100:2613-21
- Hoefeler H, Duran I, Hechmati G, et al. Health resource utilization associated with skeletal-related events by tumour type in patients with bone metastases/lesions: European analysis of a prospective multinational observational study. Poster presented at European Multidisciplinary Cancer Congress (ECCO); Stockholm, September 2011
- Hechmati G, Cure S, Gouépo A, et al. Cost of skeletal-related events in patients with bone metastases to solid tumours based on the health resource utilization collected in a prospective European multinational observational study. Value in Health 2011;14:455
- Gunther O, Body J-J, Sleeboom H, et al. Cost of skeletal complications from bone metastases: results from a retrospective European study. Support Care Cancer 2012;20(Suppl 1):S372
- Gerlier L, De Vos C, Lamotte M, et al. Epidemiology of idiopathic thrombocytopenic purpura in Belgium assessed using Hospital records. ISPOR 11th Annual European Congress, Athens, 10–12 November 2008
- Spaepen E, Demarteau N, Van Belle S, et al. Health economic evaluation of treating anemia in cancer patients receiving chemotherapy: a study in Belgian hospitals. Oncologist 2008;13:596-607
- Spaepen E, Merchant S, Neslusan C, et al. Costs and outcomes of nosocomial pneumonia in a sample of Belgian hospitals. ISPOR 9th Annual European Congress, Copenhagen, 28–31 October 2006
- Annemans L, Rémy V, Lamure E, et al. Economic burden associated with the management of cervical cancer, cervical dysplasia and genital warts in Belgium. J Med Econ 2008;11:135-50
- SPF Santé Publique. Cellule Technique de traitement de données relatives aux hôpitaux. Banque Nationale de Données Diagnostic médical/soins et coût. 2011. https://tct.fgov.be/webetct/etct-web/html/fr/index.jsp (Accessed 3 July 2012)
- Cleemput I, Van Wilder P, Vrijens F et al. Richtlijnen voor farmacoeconomische evaluaties in België. Health Technology Assessment (HTA). Brussel: Federaal Kenniscentrum voor de Gezondheidszorg (KCE); 2008. KCE Reports 78A (D/2008/10.273/23)
- Powell C. The Delphi technique: myths and realities. J Adv Nursing 2003;41:376-82
- Barlev A, Song X, Ivanov B, et al. Payer costs for inpatient treatment of pathologic fracture, surgery to bone, and spinal cord compression among patients with multiple myeloma or bone metastasis secondary to prostate or breast cancer. J Manag Care Pharm 2010;16:693-702
- UK Government National Archives. Department of Health. Payment by Results (PbR) in 2008–09. http://webarchive.nationalarchives.gov.uk/+/www.dh.gov.uk/en/Managingyourorganisation/Financeandplanning/NHSFinancialReforms/DH_081238 (Accessed 3 July 2012)
- World Health Organization. CHOosing Interventions that are Cost-Effective (WHO-CHOICE). http://www.who.int/choice/country/deu/cost/en/ (Accessed 3 July 2012)