
Abstract
Objectives:
Patients with bone metastases often experience skeletal-related events (SREs: radiation or surgery to bone, pathologic fracture, and spinal cord compression). This study examined health resource utilization and costs associated with SREs.
Methods:
Data presented are from the European cohort (Germany, Italy, Spain, and the UK) of patients with solid tumours enrolled in a multi-national, prospective, observational study in patients with solid tumours or multiple myeloma. Patients with Eastern Cooperative Oncology Group score 0–2 and life expectancy ≥6 months, who experienced an SRE up to 97 days before enrolment, were eligible. Health resource utilization associated with SREs (including number/length of inpatient stays, numbers of procedures and outpatient visits) were collected through chart review for up to 97 days before enrolment and prospectively during follow-up. Country-specific cost calculations were performed.
Results:
In total, 478 eligible patients contributed 893 SREs to this analysis. Radiation to bone occurred most frequently (66% of total). Spinal cord compression (7%) and surgery to bone (10%) were the least common events, but most likely to require inpatient stays. The most costly SREs were also spinal cord compression (mean per SRE across countries, €4884–€12,082) and surgery to bone (€3348–€9407). Inpatient stays were the main cost drivers.
Limitations:
Health resource utilization used to calculate the costs associated with SREs may have been under-estimated as a result of exclusion of patients with low performance status or life expectancy; unavailable information and exclusion of resource consumption associated with pain. Thus, the estimate of associated costs is likely to be conservative.
Conclusions:
SREs result in considerable health resource utilization, imposing a substantial financial burden driven by inpatient stays. Treatments that prevent/delay SREs may help ease this burden, thereby providing cost savings across European healthcare systems.
Introduction
Patients with breast, lung, or prostate cancers often develop bone metastases as their disease progresses to the metastatic stage. Of patients with breast and prostate cancer, 65–75% typically develop bone metastases, while up to 40% of patients with lung cancer develop the conditionCitation1. Patients who develop bone metastases often experience skeletal-related events (SREs), defined as radiation to bone, pathologic fracture, spinal cord compression, or surgery to bone; all of which are associated with large impacts on both patient well-being and health resources. For example, pathologic fractures not only cause pain, but can substantially affect patients’ quality-of-life. Rib fractures can be associated with sharp chest pains, and may ultimately lead to impaired respiratory functionCitation2. Vertebral fractures may lead to spinal instability, and hip and long-bone fractures reduce load-bearing capacity, which can lead to restriction of movement, disability, and loss of functional independenceCitation3. Spinal cord compression due to vertebral collapse or pressure exerted by the metastasized tumour often presents as a medical emergency and the resultant damage to nerve tissues can cause pain and motor weakness that may lead to paresis or paralysisCitation3. For spinal cord compression, treatments include surgery or radiation and/or high-dose steroids. Surgical intervention is also typically used to treat pathologic fracture or as a preventative measure against such complicationsCitation4. Surgery for stabilizing an established, rather than impending, fracture is generally more difficult, contributing to greater perioperative morbidity for the patientCitation2. Bone surgery can involve inpatient stays of 2 weeks, particularly if there are local post-operative complications, and frequently does not lead to reductions in use of pain-relief medicationCitation4. Radiation to bone may be used to help achieve symptom control. Following radiation therapy, there is the potential for ‘pain flare’Citation5, or for myelosuppression when irradiation is given at pelvic or long-bone sites. Unsurprisingly, SREs such as pathologic fracture or spinal cord compression are often associated with intense pain for the patient, resulting in the requirement for strong analgesics and/or surgery to manage the pain. Studies show that SREs are associated with clinically meaningful reductions in physical, functional, and emotional well-being, as measured by the Functional Assessment of Cancer Therapy–General toolCitation6. Collectively, it is clear that SREs impose a substantial clinical burden and have a significant impact on patients’ quality-of-life.
At a time when the economic environment is challenging in Europe, it is important to demonstrate the clinical, health resource, and economic burdens of a disease. This helps to evaluate the potential economic value that a new intervention may provide to guide both public and private healthcare sectors. To capture the economic value of a new therapy that targets the prevention of SREs, a comprehensive evaluation of the costs of SREs to healthcare systems is essential. Several studies have examined aspects of the economic burden of bone metastases. Retrospective database analyses in the US estimated that the overall costs associated with SREs in patients with bone metastases secondary to breast, prostate, or lung cancer over ∼1 year were ∼$12,000–$14,000 across the tumour typesCitation7–9. Additionally, Pockett et al.Citation10 assessed the hospital burden in patients over a 3-year period following diagnosis of breast, lung, or prostate cancer in Spain, demonstrating increasing costs as patients progressed to metastatic disease and had subsequent SREs. Hospital admission costs resulting from SREs were in the region of €3500–€4300 across tumour types. However, there is a lack of details on the costs of individual SRE types, and the contributions that different health resource utilizations make to costs associated with SREs in European healthcare systems.
We have reported the health resource utilization associated with SREs in a European cohort of patients with bone metastases arising from solid tumours and multiple myeloma based on data collected in a multi-national, prospective, observational studyCitation11. This study showed that SREs were associated with substantial health resource utilization (lengthy inpatient stays, several outpatient visits, and multiple procedures). In the current paper, the health resource utilization associated with SREs in the sub-group of patients with solid tumours only (excluding multiple myeloma) is presented. We complement these results by presenting data from country-specific cost analyses for each SRE type and a breakdown of the contributions of different components of health resource use to the costs of SREs.
Methods
Patients
Patients eligible for the main study were aged ≥18 years old, with a diagnosis of bone metastases secondary to breast, prostate, or lung cancer, or multiple myeloma, had an Eastern Cooperative Oncology Group (ECOG) performance status of 0, 1, or 2, and experienced at least one SRE in the 97 days prior to enrolment. Informed consent was required before the collection of patient data. Patients with a life expectancy of less than 6 months, or those who were currently enrolled in an investigational drug trial for the treatment of bone metastases or SREs were excluded. The present analysis focuses on the costs associated with SREs in patients with solid tumours.
Study design
Data used in this study were drawn from a multi-centre, prospective, observational study conducted in the US, Canada, Germany, Italy, Spain, and the UK. This report includes cost calculations based on health resource data collected from patients with solid tumours in European sites only. The protocol and informed consent form were approved by the Institutional Review Board at each site. Enrolment began in June 2008 and the cut-off for the final analysis was on 31 May 2010.
The method of data collection on health resource utilization for patients in the study has previously been describedCitation11. Health resource utilization outcome measures included: number, duration, and facility type of inpatient stays; outpatient visits; emergency department visits; number and duration of nursing home/long-term care facility stays; home health visits; and procedures (e.g., imaging, surgery, radiation sessions). Multiple related radiation sessions were counted as a single SRE of radiation to bone, to which multiple procedures of radiation were attributed. Health resource utilization data were collected retrospectively through chart review for all SREs that occurred in the 97-day period before enrolment and prospectively from the patient’s chart at least every 90 days during follow-up, thus ensuring that complications of bone metastases (incident SREs) and related health resource utilization were captured prospectively. The attribution of the health resource utilization types to each SRE was determined by the investigators at the time of data collection.
SRE and health resource utilization statistical methods
A target enrolment for the European cohort of 250 patients for each country was based on the study objective of estimating the number of days of hospitalization per SRE type. The SRE that triggered enrolment (index SRE) and all subsequent SREs were classified as one of the following: radiation to bone, pathologic fracture, spinal cord compression, or surgery to bone. Pathologic fracture was sub-categorized as either vertebral or non-vertebral fracture. Targets for the index SRE types were established for each country based on anticipated enrolment, and the goal of ensuring adequate numbers of each SRE type per tumour type for the analysis.
Descriptive analyses were produced for each SRE type by tumour type and by country. The average length of stay per inpatient stay was computed as the total length of stay (in days) of all inpatient stays attributed to the SRE divided by the total number of inpatient stays. For other outcome measures, average health resource utilization per SRE was computed as the ratio of the total health resource utilization attributed to an SRE to the total number of SREs. Radiation to bone or surgery to bone could be excluded from the health resource utilization analyses if they were determined to be secondary to a primary SRE.
Cost analyses
Cost analyses of individual SREs for each country were devised from the payer perspective.
The health resource types included in the cost analyses include number, duration, and facility type of inpatient stays; outpatient visits; emergency department visits; number and duration of nursing home/long-term care facility stays; home health visits; and procedures.
For the cost conversion of each health resource utilization type, cost equations were established and validated with country billing and clinical experts. Country-specific mean health resource utilization was multiplied by the corresponding unit costs for each country for the different SRE types. All unit costs were validated by country billing experts. Country unit costs were collected from 2010 national sources. Costs in Great British Pounds Sterling were converted into Euros (£1 = €1.128,67).
In Germany, Italy, and the UK, where diagnosis-related group (DRG)/healthcare resource group (HRG) costs were available, the cost associated with inpatient stays attributed to each SRE type was estimated based on the mean number of inpatient stays by SRE, the price of DRG/HRG (or weighted average price when several DRGs/HRGs were selected) by SRE, and the excess bed day cost of DRG/HRG (or weighted average excess bed day cost of DRGs/HRGs when several DRGs/HRGs were selected) by SRE (see for Germany, Italy, and the UK, respectively). In Spain, a per diem system was applied as no DRGs/HRGs specific to SREs from bone metastases were available. Thus, the cost associated with each outcome measure was estimated based on mean health resource utilization and unit costs for the resources used ().
Table 1. Cost of inpatient stays per SRE in Germany.
Table 2. Cost of inpatient stays per SRE in Italy.
Table 3. Cost of inpatient stays per SRE in the UK.
Table 4. Cost of inpatient stays per SRE in Spain.
Health resources of procedures performed during an inpatient stay were not taken into account since it was assumed that they were captured in the DRG, HRG, or per diem costs. Additionally, chemotherapy or hormone therapy that occurred in the outpatient setting were not included in the costs per SRE, as insufficient data were captured to estimate these costs precisely. Information about change of systemic bone-targeted therapies (e.g., change of drug, frequency, or discontinuation) was collected, but not information about inpatient/outpatient administration or which type of SRE the change related to. Therefore, health resources on systemic bone-targeted therapies were excluded from cost calculations.
Results
Study population
A total of 631 patients that met the eligibility criteria were enrolled across the four countries; of these, 478 patients (Germany, n = 149; Italy, n = 129; Spain, n = 93; UK, n = 107) had solid tumours (breast cancer, lung cancer, or prostate cancer) and contributed health resource utilization data to this study. Within this set, 46.7% of patients had breast cancer, 28.2% had lung cancer, and 25.1% had prostate cancer. Baseline demographics and disease characteristics were broadly similar to those reported for the full group of 631 patients (including those with multiple myeloma)Citation11.
The median (mean) length of prospective follow-up (across the four countries) was 6.9–10.9 (7.1–10.3) months in patients with breast cancer, 1.5–5.6 (3.2–5.6) months in patients with lung cancer, and 4.6–9.4 (5.9–8.6) months in patients with prostate cancer.
Skeletal-related events
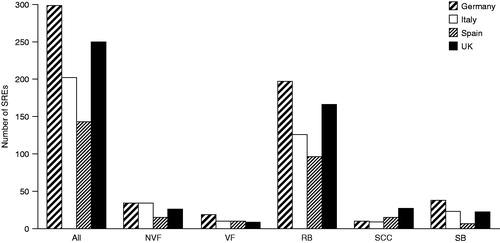
The eligible patients contributed 961 SREs to the study. The patient-year adjusted SRE rates were 2.0–2.8 (across tumour types) for Germany, 1.6–2.1 for Italy, 2.0–3.2 for Spain, and 2.4–3.9 for the UK. Sixty-eight SREs were subsequently excluded (because they were associated with the treatment of another primary SRE), thus leaving a total of 893 SREs in the health resource utilization cost-conversion analysis (109 non-vertebral fractures, 48 vertebral fractures; 585 radiations to bone; 61 spinal cord compressions; 90 surgeries to bone; ). The most frequently reported SRE type was radiation to bone (range = 96–197 occurrences), which accounted for 66% of all SREs across the European countries. The least frequently reported SRE was spinal cord compression (range = 9–27 occurrences), accounting for 7% of all SREs across the European countries. However, these rates of SRE incidence should not be considered representative of real-world distribution because target numbers of SRE types were pre-defined at enrolment. In addition, SREs that may have been linked to a prior SRE were not taken into consideration.
Figure 1. Number of skeletal-related events by country and event type included in the health resource utilization analysis and cost analysis. NVF, non-vertebral fracture; RB, radiation to bone; SB, surgery to bone; SCC, spinal cord compression; SRE, skeletal-related event; VF, vertebral fracture.
Health resource utilization
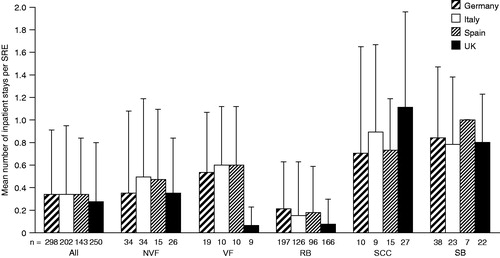
The numbers of inpatient stays associated with the different SRE types and by country are shown in . For all SRE types combined, the numbers of inpatient stays required per SRE were similar across the four countries (range of means = 0.27–0.34). When inpatient stays for the different SRE types were considered individually, the numbers of stays were also consistent across the four countries. Two SRE types were associated with similarly high numbers of inpatient stays per SRE: spinal cord compression (range of means = 0.70–1.11) and surgery to bone (0.78–1.00). Vertebral fractures were associated with a moderate number of inpatients stays in Germany, Italy, and Spain (range of means = 0.53–0.60); however, the number was considerably lower in the UK (mean = 0.06). The SRE associated with the least number of inpatient stays across the four countries was radiation to bone (range of means = 0.07–0.21).
Figure 2. Number of inpatient stays per skeletal-related event type by country. Data are shown as mean + standard deviation. n = total number of SREs of each type included in the health resource utilisation analysis. NVF, non-vertebral fracture; RB, radiation to bone; SB, surgery to bone; SCC, spinal cord compression; SRE, skeletal-related event; VF, vertebral fracture.
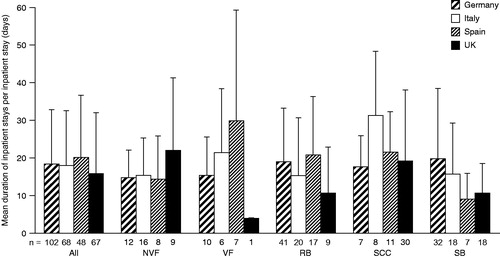
The durations of stays per inpatient stay by type of SRE across the four countries are shown in . For the all SRE types combined, the lengths of stays per inpatient stay were broadly similar across the countries (range of means = 16.0–20.2 days). For individual SREs, the ranges of inpatient stay durations were more variable across the four countries. Spinal cord compression was associated with the longest mean inpatient stays; the mean lengths were 17.6–21.6 days in Germany, Spain, and the UK, but the mean length was much longer in Italy (31.4 days). With the exception of the UK, vertebral fracture was also associated with lengthy inpatient stays: in Germany and Italy, mean lengths were 15.4 and 21.3 days, respectively; in Spain the mean length was 29.9 days, however, in the UK inpatient stays were a mean length of just 4.0 days. The lengths of inpatient stays associated with surgery to bone were comparatively short in Spain and the UK (9.0 and 10.7 days, respectively), and longer in Germany and Italy (19.8 and 15.7 days, respectively).
Figure 3. Duration of stays per inpatient stay by skeletal-related event type and country. Data are shown as mean + standard deviation. n = total number of inpatient stays by SRE type. NVF, non-vertebral fracture; RB, radiation to bone; SB, surgery to bone; SCC, spinal cord compression; SRE, skeletal-related event; VF, vertebral fracture.
Overall, 74.1% of SREs required at least one outpatient attendance (mean ± SD, 4.8 ± 5.8 per SRE). More than 95% of SREs were associated with at least one procedure (mean ± SD, 6.9 ± 6.5 per SRE).
Cost per SRE type
The mean cost associated with each SRE type from breast, prostate and lung cancers pooled together in each of the four countries studied is shown in . The SRE type with the highest associated costs was spinal cord compression (∼€5000–€12,000 across countries) followed by surgery to bone (∼€3000–€9000). Spinal cord compression was approximately twice as costly in the UK relative to the other European countries. Similarly, surgery to bone was approximately twice as expensive in the UK and Germany compared with Italy and Spain. In comparison with spinal cord compression and surgery to bone, the costs of radiation to bone, non-vertebral fracture, and vertebral fracture were generally lower across the different countries (<€3500), with the exception of vertebral fracture in Spain, which cost almost €7000. Cost data generally did not differ by type of solid tumour (data not shown).
Table 5. Mean cost per skeletal-related event in solid tumours.
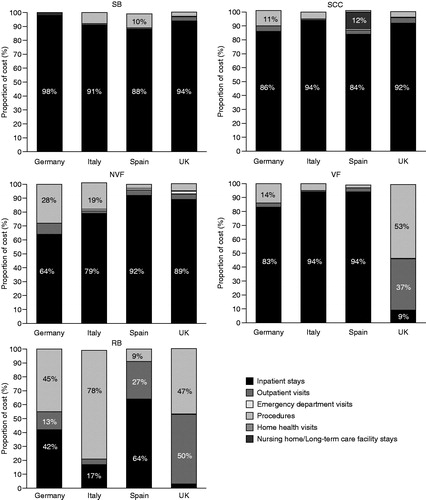
The contributions that the different types of health resource utilization made to overall costs associated with each SRE type in each country are shown in . With the exception of radiation to bone and vertebral fracture, inpatient stays were the main cost drivers for the SRE costs across all countries; inpatient stays typically contributed ∼90% of the overall costs. For radiation to bone, the major associated expenses occurred in the outpatient setting (outpatient visits and procedures), although inpatient stays were still a substantial component in Germany and in Spain. For vertebral fractures, inpatient stays were the major expense in all countries except the UK, where outpatient visits and procedures were the major expense. The other types of health resource utilization generally did not contribute substantially to overall SRE costs.
Figure 4. Mean cost breakdown by skeletal-related event and health resource utilization type by country. NVF, non-vertebral fracture; RB, radiation to bone; SB, surgery to bone; SCC, spinal cord compression; VF, vertebral fracture.
Discussion
To our knowledge, this is the first prospective, observational study to estimate the health resource utilization and associated costs of SREs in patients with bone metastases secondary to solid tumours in European countries, where investigators directly attributed health resource utilization to SREs. This study illustrates that, in addition to the devastating clinical burden that SREs impose on patients with metastatic bone disease, SREs are also associated with a substantial economic burden on European healthcare systems. The vast majority of health resource utilization resulting from SREs in patients with solid tumours arises from inpatient stays, outpatient attendances, and procedures. Of these resources, inpatient stays generally contribute the most to the cost of each SRE type.
This study benefits from a cost-conversion analysis that was based on the local health resources utilized for the different SRE types, where local unit costs, DRG/HRG costs, or per diem costs were validated by country billing experts. In estimating the costs of inpatient stays, country-specific equations were generated, using DRG/HRG costs in all countries except Spain, where no specific DRG/HRG costs for SREs relating to bone metastases were available. The two SRE types that were the most costly were spinal cord compression and surgery to bone, which had costs across the four countries of €4884–€12,082 and €3348–€9407, respectively. These high costs are a reflection of these SRE types almost always requiring lengthy inpatient admissions. The costs of the other types of SREs (non-vertebral fracture, vertebral fracture, and radiation to bone) were generally lower (€1720–€3209, €1015–€6968, and €704–€2461, respectively). Of these three SREs, radiation to bone was the least likely to require an inpatient stay, with the procedure generally performed in an outpatient setting, making this the lowest-cost SRE. In the UK, mean cost per radiation to bone event was ∼3-times lower than in the other countries. This is due to single fraction radiotherapy being usual practice in the UK for palliation of pain from bone metastasesCitation12,Citation13, in contrast to the multiple fraction approach commonly used in other European countries. Although UK guidelines on the management of spinal cord compression indicate multiple fraction radiotherapy should be usedCitation14, these radiation sessions were not attributed to the SRE of radiation to bone in this study and would not impact on its cost. Despite radiation to bone being the lowest-cost SRE, it is often the SRE most frequently reported in patients with bone metastasesCitation15,Citation16, which means its contribution to the overall real-world economic burden of SREs is large. The cost of vertebral fracture in Spain was at least 3-times higher than in the other countries. This is due to the combined effects of a high hospitalization rate and long duration of inpatient stays, especially important when a per diem billing cost conversion is used. Similarly, the cost variation seen in general can be linked to the country-specific health resource utilization and clinical practice (e.g., mean number or length of stay, type of procedures), differences in local unit costs, and billing systems (DRG/HRG vs per diem billing).
Analysis of the cost breakdown per SRE shows some variation by country. However, it is clear that inpatient stays accounted for the majority of the SRE-related economic burden across all countries. A notable exception was radiation to bone, where much of the cost was attributed to the outpatient setting, although substantial portions were attributed to inpatient stays in Germany and Spain. The latter may be a consequence of inpatient stays associated with radiation to bone being of longer duration in these countries. Although inpatient stays generally accounted for the majority of the cost associated with vertebral fracture, this was not the case in the UK, where the major expenses were procedures and outpatient visits, likely reflecting a difference in clinical practice. This trend may also help to explain why treatment of vertebral fracture was at least half the cost in the UK as in any other country.
Some limitations of our study should be acknowledged. As discussed in the report on health resource utilization in the full set of European patients with solid tumours or multiple myeloma who contributed to this study, the total health resource utilization may be under-estimatedCitation11. Reasons for this include: exclusion of patients with low performance status or life expectancy; unavailable information in relation to home health visits or unreported emergency department visits; or exclusion of additional health resource utilization associated with patients experiencing pain (not considered an SRE) that may have required strong analgesics or interventional anaesthetic techniques. Collectively, these and other factors may also contribute to an under-estimation of the total costs of SREs. For example, chemotherapy or hormone therapy that occurred in the outpatient setting were not included in the cost calculations because this category of data was not collected in sufficient detail to estimate their contribution to SRE-related HRU accurately. Our analysis assumed that procedures performed during inpatient stays were paid by DRG/HRG or per diem costs. However, this may not always be the case and, consequently, the non-inclusion of such procedures could also contribute to an under-estimation of the costs of inpatient stays. Although information about change of systemic bone-targeted therapies (e.g., change of drug, frequency of administration, or discontinuation) was collected, data on inpatient/outpatient administration of these drugs or which type of SRE the change related to were not collected, and, thus, any related health resource utilization was also excluded from cost calculations.
More generally, slow recruitment resulted in lower numbers of patients than planned from each country. This, in conjunction with a number of early withdrawals due to patient deaths, led to shorter follow-up times than planned and may limit detailed interpretation of some results. Consequently, our data may provide what may be viewed as a fairly brief ‘snapshot’ of limited SRE-related costs.
This study was observational; therefore, all SREs included were detected following routine physician visits and procedures, rather than through systematic imaging. Consequently, all the SREs included in our study reflect clinically apparent events. In addition, if an SRE only required minimal healthcare resources (for example, treatment with oral analgesics) then this was captured in this analysis as well, reducing the mean HRU per SRE accordingly. Therefore, the SRE incidence and associated costs reported here are likely to reflect real-world clinical practice.
Conclusions
This study shows that SREs arising from bone metastases secondary to solid tumours are associated with considerable health resource utilization and significant cost to European healthcare systems. The major health resources utilized as a result of SREs are inpatient stays, outpatient visits and procedures. Of these three resources, inpatient stays are the main cost driver. This study highlights the importance of effective therapies, such as the bone-targeted agents denosumabCitation17 or intravenous bisphosphonatesCitation18–20, that can delay or prevent SREs. Such treatments may provide important cost savings across European healthcare systems, thereby allowing a shift of resources to treating patients’ underlying cancer rather than the potentially debilitating complications of metastatic spread to the bone.
Transparency
Declaration of funding
This work was supported by Amgen Inc.
Declaration of financial/other interests
G. Hechmati is an employee of Amgen (Europe) GmbH and holds stock. S. Cure and A. Gouépo are employees of Optuminsight, UK. H. Hoefeler has served as an advisor to Amgen.
V. Lorusso has no conflicts of interest to declare. D. Lüftner has been a speaker for Amgen and participated in Advisory Boards. I. Duran has participated in advisory boards and lectures for Amgen and Novartis. C. Garzon-Rodriguez has participated in advisory boards for Amgen.
J. Ashcroft has participated in advisory boards for Novartis and Amgen. R. Wei is an employee of Amgen Inc. and holds stock. P. Ghelani is employed by Ovatech Solutions and has undertaken contracts with Amgen Limited. A. Bahl has participated in advisory boards and presented lectures for Amgen and Novartis.
Acknowledgements
The authors thank Dr Steven Inglis (PhD) from Oxford PharmaGenesisTM Ltd (UK) who provided medical writing support. Funding for this support was provided by Amgen Europe (GmbH).
References
- Coleman RE. Metastatic bone disease: clinical features, pathophysiology and treatment strategies. Cancer Treat Rev 2001;27:165–76
- Rubens RD. Bone metastases—the clinical problem. Eur J Cancer 1998;34:210–3
- Coleman RE. Clinical features of metastatic bone disease and risk of skeletal morbidity. Clin Cancer Res 2006;12:6243s–9s
- Katzer A, Meenen NM, Grabbe F, et al. Surgery of skeletal metastases. Arch Orthop Trauma Surg 2002;122:251–8
- Loblaw DA, Wu JS, Kirkbride P, et al. Pain flare in patients with bone metastases after palliative radiotherapy—a nested randomized control trial. Support Care Cancer 2007;15:451–5
- Weinfurt KP, Li Y, Castel LD, et al. The significance of skeletal-related events for the health-related quality of life of patients with metastatic prostate cancer. Ann Oncol 2005;16:579–84
- Delea T, Langer C, McKiernan J, et al. The cost of treatment of skeletal-related events in patients with bone metastases from lung cancer. Oncology 2004;67:390–6
- Delea T, McKiernan J, Brandman J, et al. Retrospective study of the effect of skeletal complications on total medical care costs in patients with bone metastases of breast cancer seen in typical clinical practice. J Support Oncol 2006;4:341–7
- Lage MJ, Barber BL, Harrison DJ, et al. The cost of treating skeletal-related events in patients with prostate cancer. Am J Manag Care 2008;14:317–22
- Pockett RD, Castellano D, McEwan P, et al. The hospital burden of disease associated with bone metastases and skeletal-related events in patients with breast cancer, lung cancer, or prostate cancer in Spain. Eur J Cancer Care 2010;19:755–60
- Hechmati G, Hoefeler H, Bahl A, et al. Skeletal-related events in patients with bone metastases lead to considerable health resource utilisation in Europe: analysis of a multinational observational study. Value Health 2011;14:A168
- National Institute of Clinical Excellence (NICE). Advanced breast cancer: diagnosis and treatment. Full Guideline. 2009. London: NICE. http://guidance.nice.org.uk/CG81/Guidance/pdf/English. Accessed July 5, 2012
- National Institute of Clinical Excellence (NICE). The diagnosis and treatment of lung cancer (update). Full Guideline. 2011. London: NICE. http://guidance.nice.org.uk/CG121/Guidance/pdf/English. Accessed July 5, 2012
- National Institute of Clinical Excellence (NICE). Metastatic spincal cord compression: diagnosis and management of patients at risk of or with metastatic spinal cord compression. Full Guideline. 2008. London: NICE. http://guidance.nice.org.uk/CG75/Guidance/pdf/English. Accessed July 5, 2012
- Saad F, McKiernan J, Eastham J. Rationale for zoledronic acid therapy in men with hormone-sensitive prostate cancer with or without bone metastasis. Urol Oncol 2006;24:4–12
- Rosen LS, Gordon D, Tchekmedyian NS, et al. Long-term efficacy and safety of zoledronic acid in the treatment of skeletal metastases in patients with nonsmall cell lung carcinoma and other solid tumors: a randomized, Phase III, double-blind, placebo-controlled trial. Cancer 2004;100:2613–21
- Lipton A, Fizazi K, Stopeck AT, et al. Superiority of denosumab to zoledronic acid for prevention of skeletal-related events: a combined analysis of 3 pivotal, randomised, phase 3 trials. Eur J Cancer 2012;48:3082–92
- Kohno N, Aogi K, Minami H, et al. Zoledronic acid significantly reduces skeletal complications compared with placebo in Japanese women with bone metastases from breast cancer: a randomized, placebo-controlled trial. J Clin Oncol 2005;23:3314–21
- Rosen LS, Gordon D, Tchekmedyian S, et al. Zoledronic acid versus placebo in the treatment of skeletal metastases in patients with lung cancer and other solid tumors: a phase III, double-blind, randomized trial–the Zoledronic Acid Lung Cancer and Other Solid Tumors Study Group. J Clin Oncol 2003;21:3150–7
- Saad F, Gleason DM, Murray R, et al. Long-term efficacy of zoledronic acid for the prevention of skeletal complications in patients with metastatic hormone-refractory prostate cancer. J Natl Cancer Inst 2004;96:879–82