
Abstract
Objectives:
To identify risk factors for initial treatment failure in patients with community-acquired pneumonia (CAP) in non-intensive care unit (non-ICU) settings, and to characterize the association between initial treatment failure and length of stay, total hospital charges, and mortality.
Methods:
Retrospective cohort study. Using data from >100 US hospitals, this study identified all adults (age ≥18 years) hospitalized for pneumonia between January 1, 2000 and June 30, 2009 who began antibiotic therapy within 24 h of admission and were treated for at least 48 h if alive; patients admitted to intensive care within the first 24 h in hospital were excluded. Initial therapy was defined as all parenteral antibiotics administered within the first 24 h in hospital. Treatment failure was assessed based on subsequent receipt of new antibiotic(s), excluding agents of similar/narrower spectrum and those begun at discharge. Multivariate logistic regression was used to identify risk factors for treatment failure, and multivariate linear and logistic regression to compare length of stay, total hospital charges, and in-hospital mortality between patients experiencing initial treatment failure and those who did not.
Results:
Among 32,324 patients with non-ICU CAP, 4695 (14.6%) experienced initial treatment failure, most often within 72 h of hospital admission. Significant predictors of initial treatment failure included malnourishment (OR = 1.87; 95% CI = 1.60–2.18), receipt of vasoactive medications within 24 h of admission (1.51 [1.17–1.94]), and renal failure (1.45 [1.32–1.59]). Treatment failure was associated with higher case fatality (8.5% vs 3.3%), longer hospital stays (mean [SD] = 10.1 [8.1] days vs 4.9 [3.3] days), and higher total hospital charges ($37,602 [$71,876] vs $14,371 [$21,633]) (all comparisons, p < 0.01). Study limitations include possible inclusion of patients with healthcare-associated pneumonia (HCAP) in the study sample, our focus on the 40 most commonly used antibiotic regimens, and indirect measurement of treatment failure.
Conclusions:
Approximately one in seven non-ICU CAP patients experience failure of initial antibiotic therapy. Risk of failure is higher for patients with significant comorbidities and/or severe infections. Non-ICU patients who experience initial treatment failure have significantly longer hospital stays, higher total hospital charges, and higher rates of mortality.
Introduction
Community-acquired pneumonia (CAP) accounts for more than 1 million admissions annually to US hospitalsCitation1. Most (80–90%) patients hospitalized for CAP are treated in non-intensive care unit (ICU) settingsCitation2. While Streptococcus pneumoniae, Haemophilus influenza, and Staphylococcus aureus are common casual pathogens in these patientsCitation3, etiology is typically unknown at initial presentation; in most cases, in fact, it is never determinedCitation4. In a large study at four hospitals in the US and Canada, a microbiological cause of pneumonia was established in only 29.6% of patients hospitalized for CAPCitation5.
Antibiotic therapy is the cornerstone of treatment for bacterial pneumonia. Since causative pathogens are generally unknown at presentation, and because delays in treatment are associated with worse clinical outcomesCitation6,Citation7, initial therapy is often begun within hours of hospital arrival and is typically empiric. Guidelines, such as those of the Infectious Diseases Society of America (IDSA) and the American Thoracic Society (ATS)Citation3,Citation8,Citation9, recommend that initial therapy be selected based on the pathogens likely to be encountered, risk factors for antibiotic resistance (e.g., advanced age, immunocompromising conditions), comorbidities, and severity of illness.
Although most CAP patients experience amelioration of symptoms within 2–3 days, 6–33% have been reported to experience failure of initial therapyCitation10–16. Initial treatment failure is therefore a fairly common clinical problem in these patients; recent US guidelines have addressed this problem under the heading ‘non-responding pneumonia’Citation3. The causes of initial treatment failure are myriad, and include receipt of antibiotic therapy that is ineffective against casuative pathogen(s), severity of infection (e.g., multilobar pneumonia, empyema), and compromised host immunity. Because causative pathogens are identified in relatively few patients in typical clinical practice, it is impossible in most instances to measure initial treatment failure in CAP directly. Operational definitions used in many studies, therefore, focus on clinical deterioration or failure to evidence good clinical response within a reasonable period of timeCitation17.
When patients fail to respond adequately to initial treatment, antibiotic therapy may be modified and/or the level of supportive care may be increased (e.g., mechanical ventilation, thoracentesis, pressors). In the minority of cases in which etiology can be established and culture results indicate that the identified pathogen may not have been susceptible to initial treatment, targeted antibiotic therapy can be initiated. In the great majority of patients in whom causative pathogens remain unknown, however, inadequate clinical response often results in the decision to move to a second-line therapy, usually characterized by a broader spectrum.
In our study, we examine initial treatment failure in hospitalized patients with CAP who are not admitted to ICU in the first 24 h (‘non-ICU CAP’), as well as risk factors for this outcome. We also examine the association between initial treatment failure and length of stay, total in-hospital charges, and inpatient mortality. Since it is impossible to examine antibiotic failure per se in the vast majority of patients with non-ICU CAP, for whom etiology is never established, we use changes in antibiotic therapy as a marker for initial treatment failure.
Patients and methods
Data source
Data were obtained from the Cerner Health Facts Database®, a large electronic data warehouse containing clinical information (described below) from ∼38 million inpatient admissions, emergency department encounters, and outpatient/clinic visits at more than 100 general, acute-care, hospitals in the US.
Information available for each admission includes patient demographics (e.g., age, sex, race), hospital characteristics (e.g., geographic region, number of beds, teaching status), admitting diagnoses (in free text), discharge diagnoses (principal and all secondary) (in International Classification of Diseases, Ninth Revision, Clinical Modification [ICD-9-CM] format), procedures performed (in ICD-9-CM format), all medications administered (including but not limited to antibiotics) (with date and time of administration), results of laboratory tests, discharge status (i.e., alive vs dead) and destination (e.g., home, skilled nursing facility), and total in-hospital charges.
All patient-identifying information was either encrypted or removed from the database, rendering it compliant with the Health Insurance Portability and Accountability Act of 1996 (HIPAA) and federal guidance on Public Welfare and the Protection of Human Subjects. Accordingly, Institutional Review Board (IRB) review and approval was not needed for this study.
Source population
We identified all adults (age ≥18 years) hospitalized for pneumonia (ICD-9-CM diagnosis codes 481, 482.XX, 483.X, 484.3, 484.5, 485, 486, 487.0) between January 1, 2000 and June 30, 2009 (‘study period’) who began antibiotic therapy within 24 h of admission and were treated for at least 48 h if alive. We excluded from our study sample: (1) patients who were admitted to intensive care within the first 24 h in hospital or who died within this period (early deaths are unlikely to depend on antibiotic therapy received); (2) patients with secondary diagnoses of other infections, with the exceptions of empyema (ICD-9-CM 510.XX), septicemia/bacteremia (003.1, 038.XX), and systemic inflammatory response syndrome (SIRS) (995.9X); and (3) patients with probable healthcare-associated pneumonia (HCAP), based on evidence of transfer from another healthcare facility, prior hospitalization within 30 days, receipt of hemodialysis, cancer chemotherapy, or intravenous antibiotics, wound care in the last 30 days, or solid organ or bone marrow transplant.
Among patients meeting study entry criteria, we designated all parenterally administered antibiotics received within the first 24 h following hospital admission as ‘initial antibiotic therapy’. We limited our attention to patients who received initial antibiotic therapy with a regimen that was among the 40 most commonly used regimens in calendar year (CY) 2009 (across all study subjects, a total of ∼1200 unique regimens were identified). The 40 most common initial antibiotic regimens accounted for 81% of all non-ICU CAP admissions in our study sample. Attention was focused on 40 regimens only, as a unique ‘failure algorithm’ had to be developed for each regimen, as described below.
Measures
The demographic and clinical characteristics of study subjects were characterized in terms of patient age, sex, and presence (as secondary discharge diagnoses) of selected comorbidities (Appendix). We also examined the results of all labs drawn within 24 h of initial clinical presentation for findings (e.g., leukopenia, uremia) that might be predictive of treatment outcome; where multiple lab values were available, we used the earliest one.
We defined initial treatment failure based on initiation of a new antibiotic not previously received within the first 24 h in hospital, excluding substitution of agents of similar or narrower spectrum (i.e., de-escalation/streamlining), switches from parenteral to oral therapy, and regimen changes on the day of (live) hospital discharge or the preceding day, all of which are unlikely to occur as a result of treatment failure. Our definition of treatment failure, therefore, required that we develop a unique ‘failure algorithm’ for each included regimen so we could identify all instances where antibiotic coverage either had been changed or broadened. For instance, in patients treated initially with levofloxacin, receipt of any new antibiotic other than another fluoroquinolone, ampicillin, a first-generation or second-generation cephalosporin, penicillin, penicillin G, or a macrolide was deemed to have constituted a change or broadening of therapy (and hence evidence of treatment failure). Similar algorithms were developed for the other 39 regimens of interest (). Administration of the first dose of a qualifying new antibiotic was designated as time of treatment failure.
Table 1. Failure algorithms for the 40 most commonly initial antibiotic regimens in non-ICU CAP.
Analyses
We examined the demographic and clinical characteristics of study subjects, as well as selected characteristics (e.g., number of licensed beds, teaching status) of admitting hospitals. We also examined the distribution of study subjects across the 40 initial regimens of interest.
We estimated the rate of initial treatment failure, and examined predictors of failure using multivariate logistic regression. Covariates in the regression model included patient and hospital characteristics (as described above), hospitalization for pneumonia in the prior year, time to initial receipt of antibiotics, and selected comorbidities and other proxies for case severity and/or poor prognosis that could be assessed at initial presentation (e.g., liver disease, renal disease, alcohol/drug abuse, obstructive/structural lung disease, uremia, leukopenia, receipt of vasoactive medications <24 h prior to hospital admission)Citation3,Citation17–19. Comorbidities were ascertained based on relevant diagnosis codes (e.g., liver disease), procedure codes on the day of admission (e.g., parenteral nutrition), medication receipt (e.g., vasopressors), or combinations thereof (e.g., diagnosis code for end-stage renal disease and/or procedure code for hemodialysis).
We also compared length of stay in hospital, total inpatient charges, and inpatient mortality (excluding deaths within the first 24 h, as this was an exclusionary criterion) between patients with evidence of initial treatment failure and those without such evidence. Multivariate multiple regression models were used in comparisons of length of stay and total inpatient charges. Explanatory variables that were entered into these models included all covariates used in analyses of predictors of treatment failure as well as initial treatment outcome (i.e., success vs failure). Multivariate logistic regression also was used in comparisons of inpatient mortality in relation to outcome of initial antibiotic therapy. The above-described analyses were undertaken alternatively for patients who experienced treatment failure any time during their hospitalization and for the sub-group of these patients who experienced failure within 72 h of admission. The latter analyses were undertaken because inclusion of patients who experienced failure >72 h could conflate cause and effect (e.g., patients with long hospital stays may be more likely to develop nosocomial infections that necessitate changes to their initial treatment regimen). In the latter analyses, patients who did not experience treatment failure within 72 h were designated ‘not failed’ whether or not they experienced treatment failure subsequently. All analyses were conducted using PC-SAS v9.1 (SAS).
Results
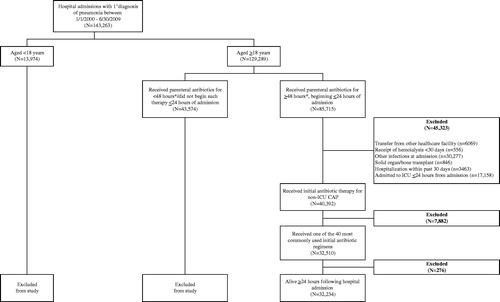
We identified 129,289 patients aged ≥18 years who were admitted to hospital with a principal diagnosis of pneumonia between January 1, 2000 and June 30, 2009 (). Among these patients, 32,234 began antibiotic therapy within 24 h of hospital admission, were not admitted to ICU during this period, were treated for at least 48 h if alive, and met all other study entry criteria.
Figure 1. Sample selection. *Or at least 1 dose of such therapy, for those who died within 48 hours of admission. NOTE: ICD-9-CM diagnosis codes 481, 482.XX, 483.X, 484.3, 484.5, 485, 486, and 487.0 used to define pneumonia. ICU: Intensive care unit.
Sixty percent of patients received either fluoroquinolone monotherapy (n = 10,148) or a multi-drug regimen that included a macrolide and a beta-lactam antibiotic (n = 9289).
Mean age of study subjects was 70 years (median = 74 years); there were similar numbers of women and men (). Common comorbidities included congestive heart failure (CHF) (26.9% of all study subjects), chronic obstructive pulmonary disease (COPD) (24.9%), other respiratory diseases (34.1%), and compromised immune status (32.9%). Approximately 23% of patients were hypoxic at admission; a similar proportion were uremic. Four percent of patients had been hospitalized for pneumonia in the prior year.
Table 2. Demographic and clinical characteristics of non-ICU patients admitted for CAP: 2000–2009 (n = 32,234).*†
The most frequently prescribed initial antibiotic regimens were levofloxacin (26.7% of all admissions), azithromycin + ceftriaxone (20.1%), and ceftriaxone (13.3%), which together accounted for ∼60% of all non-ICU CAP admissions (). A total of 4695 patients (14.6%) experienced initial treatment failure, most often (65% of all such cases) within 72 h of hospital admission. Median (interquartile range [IQR]) time to initial treatment failure was 50 h (31 h, 93 h). In multivariate logistic regression, significant predictors of initial treatment failure were malnourishment (odds ratio [OR] = 1.87; 95% confidence interval [CI] = 1.60–2.18), renal failure (1.45 [1.32–1.59]), and immunocompromising conditions (1.43 [1.32–1.56]) as secondary diagnoses, and hypoxemia (1.31 [1.11–1.56]), uremia (1.45 [1.33–1.58]), and acidosis (1.77 [1.38–2.27]) at hospital admission (). The rate of initial treatment failure also was higher in patients who received endotracheal intubation, mechanical ventilation, or central venous catheterization within 24 h of admission (albeit not in the ICU) (2.43 [1.90–3.12]), and in patients who received their first dose of antibiotics more than 8 h following initial clinical presentation (1.22 [1.14–1.30]). The rate of initial treatment failure was lower among patients in teaching hospitals (vs non-teaching hospitals) (0.82 [0.76–0.88]).
Table 3. Frequency distribution of initial antibiotic regimens among non-ICU patients admitted for CAP: 2000–2009 (n = 32,234).*
Table 4. Multivariate logistic regression of factors associated with failure of initial antibiotic therapy in non-ICU CAP.
Initial treatment failure was associated with an additional 5.2 days in hospital (mean [standard deviation] [SD] = 10.1 [8.1] days vs 4.9 [3.3] days, respectively), and $23,231 in additional hospital charges ($37,602 [$71,876] vs $14,371 [$21,633]) (both comparisons, p < 0.01 in multivariate models). Inpatient mortality (excluding deaths within the first 24 h) was ∼2-fold higher in patients who experienced initial treatment failure (8.5% vs 3.3% among those who did not; p < 0.01). Treatment failure within the first 72 h also was associated with longer stays in hospital (7.8 [5.4] days vs 5.6 [4.6] days), higher total inpatient charges ($26,335 [40,964] vs $16,869 [$34,112]), and a higher rate of mortality (6.9% vs 3.7%) (all comparisons, p < 0.01 in multivariate models).
Discussion
Initial antibiotic therapy for CAP is usually empiric, since causative pathogens are typically unknown at clinical presentation. In selecting an initial regimen, multiple factors must be considered, including risks of treatment failure, antibiotic resistance, side-effect(s) of treatment, and costs of patient care. While broad-spectrum regimens may be more effective than narrow ones, they are more costly and their over-use may hasten the emergence of resistant micro-organisms. On the other hand, while concerns about fostering antibiotic resistance and costs may be lower with narrow-spectrum regimens, they may not be as effective as regimens with a broader spectrum. Knowledge of the predictors of treatment failure, and the association between initial treatment failure and length of stay, total hospital charges, and mortality may be important considerations in therapeutic decision-making.
In our study of more than 32,000 hospitalized patients with non-ICU CAP, 14.6% of subjects had evidence of a substantial change or broadening of antibiotic coverage more than 24 h following hospital admission, usually within the first 72 h. Significant predictors of initial treatment failure included (but were not limited to) malnourishment, receipt of vasoactive medications within 24 h of admission, and renal failure. Delays of more than 8 h between initial presentation and receipt of first dose were also associated with a higher rate of failure, consistent with prior research reporting a reduction in mortality among patients beginning antibiotic therapy within 8 h of admissionCitation6,Citation7,Citation20,Citation21.
Our estimate of the rate of initial treatment failure is similar to what has been reported previouslyCitation10–15. For example, in their study of 260 patients admitted for CAP between July 2000 and June 2003, Hoogewerf et al.Citation13 reported that 31% of study subjects satisfied their criteria for ‘early clinical failure’, which they defined as occurrence ≥3 days following hospital admission of any of the following events: death, mechanical ventilation, respiratory rate >25/min, <90% oxygen saturation, PaO2 <55 mm Hg, hemodynamic instability, altered mental state, or fever. In another study involving 500 consecutive patients admitted to hospital for CAP, Aliberti et al.Citation16 estimated the incidence of clinical failure (defined as need for mechanical ventilation, receipt of aggressive therapy for hemodynamic deterioration, or in-hospital death up to 28 days following admission) to be 13%; they included patients who were admitted directly to the ICU (17% of all study subjects), however, while we excluded all patients admitted to the ICU during the first 24 h in hospital.
Despite these similarities in findings, it is important to point out that our sample selection criteria and definition of initial treatment failure differed from those employed in other studies. Moreover, limitations of our database prevented us from replicating definitions of initial treatment failure employed by others. We note, however, that similar definitions of initial treatment failure (i.e., change in antibiotic therapy) have been used in earlier retrospective studies in patients with complicated intra-abdominal infectionsCitation22,Citation23 and complicated skin and soft-tissue infectionsCitation24.
Our findings suggest that initial treatment failure in non-ICU CAP is associated with an additional 5.2 days in hospital, more than $23,000 in additional inpatient charges, and a greater than 2-fold higher rate of mortality. It is important to note, however, that these comparisons represent an ‘improper’ sub-group analysisCitation25, in that the groups are defined on the basis of an outcome (i.e., success vs failure of initial treatment). Such comparisons can result in conflation of cause and effect (e.g., treatment failure may be associated with longer stays because longer stays increase risk of nosocomial infections). To address this issue, we conducted a sub-group analysis in which we focused exclusively on treatment failure in the first 72 h following admission, thereby partially controlling for this problem (64% of all treatment failures occurred within this timeframe). In this sub-group analysis, the association of initial treatment failure with length of stay, total inpatient charges, and mortality (excluding deaths within the first 24 h in hospital) remained strong. We therefore believe that our findings are not an artifact of an outcomes-based comparison.
Nonetheless, it is important to note that our findings concerning an association between initial treatment failure and the outcomes of interest simply may reflect inherent differences between patients who experience treatment failure vs those who do not, and not necessarily a causal relationship. For example, many of the risk factors for initial treatment failure that we identified (e.g., renal failure, immunocompromising conditions) are also correlated with longer stays in hospital, higher costs of care, and higher rates of mortality, and thus may confound the relationship between failure and outcomes that we observed.
Several additional limitations of our study merit discussion. We limited our attention to patients who received any of the 40 antibiotic regimens most commonly used in CY2009 as initial therapy for non-ICU CAP for convenience (i.e., to limit the number of failure algorithms we had to develop). We note, however, that these patients constituted 81% of all non-ICU CAP admissions in our study population. Furthermore, ∼60% of patients received either fluoroquinolone monotherapy or a regimen comprised of a beta-lactam and a macrolide, consistent with both current treatment guidelinesCitation3 and a ‘core measure’ of The Joint Commission for initial antibiotic therapy in hospitalized patients with CAP. Nevertheless, our findings may not be generalizable to patients who receive other, less frequently used regimens.
In retrospective studies, operational definitions of measures may be less precise than those possible with prospective data collection. For example, the algorithms that we employed to exclude patients with HCAP are less than perfectly sensitive due to inherent limitations in our data (e.g., information on hospital admissions during the prior 30 days is limited to those that occurred at the same hospital [or hospital system]). Some patients with HCAP, therefore, may have ended up in our study sample.
Finally, while our study is one of the largest to date, and reflects the experience of ∼32,000 CAP patients at more than 100 US hospitals over a period of almost 10 years, our sample is not random. Although hospitals in the database appear to be similar to acute-care hospitals generally throughout the US, the former may in fact differ from the latter in a number of unknown respects. The impact that this would have on our findings is unclear.
Conclusion
Approximately one-in-seven non-ICU CAP patients experience failure of initial antibiotic therapy. Risk of failure is higher for patients with significant comorbidities and/or severe infections. Non-ICU patients who experience initial treatment failure have significantly longer hospital stays, higher total hospital charges, and higher rates of mortality. Our study may help guide therapeutic decision-making in this setting.
Transparency
Declaration of funding
This study was supported by Forest Research Institute, Inc. Forest Research Institute, Inc. was involved in the design and decision to present these results. Funding for editorial assistance was provided by Forest Research Institute, Inc. Forest Research Institute, Inc. had no involvement in the collection, analysis, or interpretation of data. Data management, processing, and analyses were conducted by AB, JE, and GO. All authors read and approved the final manuscript.
Declaration of financial/other relationships
AB, JE, and GO are employed by Policy Analysis Inc., which received study funding from Forest Laboratories, Inc. DW was a paid consultant to Policy Analysis Inc. on this study. CMRO peer reviewers may have received honoraria for their review work. The peer reviewers on this manuscript have disclosed that they have no relevant financial relationships.
Acknowledgments
We thank Scientific Therapeutics Information, Inc. (Springfield, New Jersey) for their editorial assistance. Portions of this research were presented previously at the 2010 Annual Meeting of the Interscience Conference on Antimicrobial Agents and Chemotherapy (ICAAC) (‘Real-World’ Failure of Initial Antibiotic Therapy in Non-ICU Community-Acquired Pneumonia [CAP] in US Hospitals, 2000–2009) (September 12–15, 2010; Boston, MA), and the 2010 Mid-Year Clinical Meeting of the American Society of Health System Pharmacists (ASHP) (Consequences of Failure of Initial Antibiotic Therapy in Patients with Non-ICU Community-Acquired Pneumonia [CAP] in US Hospitals, 2000–2009) (December 5–9, 2010; Anaheim, CA).
References
- Niederman MS. Community-acquired pneumonia: the U.S. perspective. Semin Respir Crit Care Med 2009;30:179-88
- File TM, Jr Marrie TJ. Burden of community-acquired pneumonia in North American adults. Postgrad Med 2010;122:130-41
- Mandell LA, Wunderink RG, Anzueto A, et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis 2007;44(2 Suppl):S27-S72
- Niederman MS, Bass JB, Jr Campbell GD, et al. Guidelines for the initial management of adults with community-acquired pneumonia: diagnosis, assessment of severity, and initial antimicrobial therapy. American Thoracic Society. Medical Section of the American Lung Association. Am Rev Respir Dis 1993;148:1418-26
- Fine MJ, Stone RA, Singer DE, et al. Processes and outcomes of care for patients with community-acquired pneumonia: results from the Pneumonia Patient Outcomes Research Team (PORT) Cohort Study. Arch Intern Med 1999;159:970-80
- Meehan TP, Fine MJ, Krumholz HM, et al. Quality of care, process, and outcomes in elderly patients with pneumonia. JAMA 1997;278:2080-4
- Houck PM, Bratzler DW, Nsa W, et al. Timing of antibiotic administration and outcomes for Medicare patients hospitalized with community-acquired pneumonia. Arch Intern Med 2004;164:637-44
- Niederman MS, Mandell LA, Anzueto A, et al; for the American Thoracic Society. Guidelines for the management of adults with community-acquired pneumonia. Diagnosis, assessment of severity, antimicrobial therapy, and prevention. Am J Respir Crit Care Med 2001;163:1730-54
- Bartlett JG, Dowell SF, Mandell LA, et al. Practice guidelines for the management of community-acquired pneumonia in adults. Infectious Diseases Society of America. Clin Infect Dis 2000;31:347-82
- Arancibia F, Ewig S, Martinez JA, et al. Antimicrobial treatment failures in patients with community-acquired pneumonia: causes and prognostic implications. Am J Respir Crit Care Med 2000;162:154-60
- Menéndez R, Torres A, Zalacaín R, et al; for Neumofail Group. Risk factors of treatment failure in community acquired pneumonia: implications for disease outcome. Thorax 2004;59:960-5
- Genné D, Sommer R, Kaiser L, et al. Analysis of factors that contribute to treatment failure in patients with community-acquired pneumonia. Eur J Clin Microbiol Infect Dis 2006;25:159-66
- Hoogewerf M, Oosterheert JJ, Hak E, et al. Prognostic factors for early clinical failure in patients with severe community-acquired pneumonia. Clin Microbiol Infect 2006;12:1097-104
- Rosón B, Carratalà J, Fernández-Sabé N, et al. Causes and factors associated with early failure in hospitalized patients with community-acquired pneumonia. Arch Intern Med 2004;164:502-8
- Bruns AH, Oosterheert JJ, Hustinx WN, et al. Time for first antibiotic dose is not predictive for the early clinical failure of moderate-severe community-acquired pneumonia. Eur J Clin Microbiol Infect Dis 2009;28:913-9
- Aliberti S, Amir A, Peyrani P, et al. Incidence, etiology, timing, and risk factors for clinical failure in hospitalized patients with community-acquired pneumonia. Chest 2008;134:955-62
- File TM. Community-acquired pneumonia. Lancet 2003;362:1991-2001
- Escobar GJ, Fireman BH, Palen TE, et al. Risk adjusting community-acquired pneumonia hospital outcomes using automated databases. Am J Manag Care 2008;14:158-66
- Fine MJ, Singer DE, Hanusha BH, et al. Validation of a pneumonia prognostic index using the MedisGroups Comparative Hospital Database. Am J Med 1993;94:153-9
- Mortensen EM, Restrepo M, Anzueto A, et al. Effects of guideline-concordant antimicrobial therapy on mortality among patients with community-acquired pneumonia. Am J Med 2004;117:726-31
- Marrie TJ, Wu L. Factors influencing in-hospital mortality in community-acquired pneumonia: a prospective study of patients not initially admitted to the ICU. Chest 2005;127:1260-70
- Cattan P, Yin DD, Sarfati E, et al. Cost of care for inpatients with community-acquired intra-abdominal infections. Eur J Clin Microbiol Infect Dis 2002;21:787-93
- Edelsberg J, Berger A, Schell S, et al. Economic consequences of failure of initial antibiotic therapy in hospitalized adults with complicated intra-abdominal infections. Surg Infect (Larchmt) 2008;9:335-47
- Edelsberg J, Berger A, Weber DJ, et al. Clinical and economic consequences of failure of initial antibiotic therapy for hospitalized patients with complicated skin and skin-structure infections. Infect Control Hosp Epidemiol 2008;29:160-9
- Yusuf S, Wittes J, Probstfield J, et al. Analysis and interpretation of treatment effects in subgroups of patients in randomized controlled trials. JAMA 1991;266:93-8
Appendix
Definitions for comorbidities of interest.