
Abstract
Objectives:
To describe the changes in resource utilization in seven European countries (Germany, Greece, Portugal, Romania, Sweden, Spain, and Turkey) and direct costs in four European countries (Germany, Spain, Sweden, and Greece) over the first 12 months of insulin treatment in patients with type 2 diabetes mellitus (T2DM).
Methods:
INSTIGATE and TREAT (2005–2010) were non-interventional, prospective, observational studies in patients with T2DM and initiating insulin for the first time. A 6-month retrospective data capture was conducted at baseline (insulin initiation) followed by prospective data collections at ∼3, 6, and 12 months. Statistical analyses were descriptive; estimated costs are presented as nominal values.
Results:
This study presents data for 1450 patients. Overall, in the first 6 months after insulin initiation, the use and cost of blood glucose monitoring and insulin increased, while the cost of oral diabetic medication decreased. Contributors to total direct costs differed between countries. Ranges of total mean direct costs over the 6-month period before insulin initiation were €489.10–€658.50 (Greece–Spain); 0–6 months after insulin initiation, €573.40–€1084.70 (Greece–Spain); and 6–12 months after insulin initiation, €495.80–€859.30 (Greece–Germany). Thus, the mean cost of treatment increased in all countries in the first 6 months after insulin initiation and then returned to baseline except in Germany.
Limitations:
Overall, 15% of patients were lost to follow-up over 12 months. Costs were not pro-rated to account for variation of visits. Participating centres may not have been fully representative of all levels of care.
Conclusions:
Contributors to total cost differed between countries, potentially reflecting local clinical practice patterns and insulin regimens. In each country, mean direct total costs of T2DM care increased during the first 6 months after insulin initiation and decreased thereafter.
Introduction
Type 2 diabetes mellitus (T2DM) is a leading cause of morbidity and mortalityCitation1. Many patients with diabetes will develop diabetes-related macrovascular or microvascular complicationsCitation2. Consequently, healthcare expenditures may be as much as 5 times higher for patients with diabetes than for patients without diabetesCitation3,Citation4. Diabetes-related complications account for the majority of the cost of diabetes careCitation5, and thus reducing the incidence of complications likely would reduce individual and overall costs of careCitation6–8.
Treatment to control hyperglycemia in T2DM routinely begins with lifestyle changes, such as diet and exercise, and metformin. If glycemic control remains sub-optimal, other oral anti-diabetes (OAD) medications, GLP-1 receptor agonists, or insulin therapy are addedCitation9–11. Due to the progressive nature of T2DM, many patients will eventually require insulin therapyCitation12–14. Despite common use of insulin for the treatment of T2DM in EuropeCitation15, there are limited published data on the cost of insulin initiation and associated utilization of resourcesCitation16,Citation17. Such an assessment is important to plan effectively for diabetes-related resources in healthcare settingsCitation18,Citation19.
The Insulin Titration—Gaining an Understanding of the Burden of Type 2 Diabetes in Europe (INSTIGATE) study and the Treatment Factors and Costs Associated with Insulin Therapy in Patients with Type 2 Diabetes (TREAT) study were observational studies of patients with T2DM initiating any insulin therapy during routine clinical careCitation20–26. INSTIGATE was initially conducted for 6 months and extended to up to 2 years in Germany, Greece, and Spain, while TREAT was conducted for 2 years in Greece, Portugal, Romania, Sweden, and Turkey. The primary objectives of INSTIGATE and TREAT were to assess the direct costs associated with T2DM treatment following initiation of insulin therapy, and secondary objectives included the evaluation of clinical outcomes. Costs and resource use have already been described in the first 6 months following insulin initiation in INSTIGATECitation24. Here, we further report the direct costs and resource use associated with 12 months of insulin therapy in both observational studies.
Patients and methods
Study design
INSTIGATE and TREAT were prospective, observational, non-interventional, multi-center, open-label studies. Eligible consenting patients with T2DM and initiating insulin for the first time were observed at initiation and over 24 months during the course of usual care. Investigators either initiated insulin therapy or referred patients to specialists for insulin initiation and remained active in usual patient care. In Germany, only diabetologists participated in the study. In other countries, diabetologists, endocrinologists, and general practitioners who treated patients with T2DM participated.
Both studies were performed in accordance with the Declaration of Helsinki (1996). Local requirements for ethical review and regulatory notifications were met for each participating country, and all patients provided written informed consent for the release of information at the time of insulin initiation (baseline).
INSTIGATE patients (n = 1172) were recruited from 121 investigator sites in France, Germany, Greece, Spain, and the UK, beginning in November 2005 with visits through November 2008. These patients were observed for 6 months after insulin initiation (baseline). Consenting patients in Germany, Greece, and Spain participated in an extended observation that lasted for an additional 6–18 months. Further design details and baseline characteristics as well as clinical data and cost and resource use data for the first 6 months have been reported previouslyCitation20–24. This manuscript presents resource use and cost data from the follow-up of INSTIGATE patients participating in the extension phase only (Germany, n = 155; Greece, n = 237; and Spain, n = 172).
TREAT was planned as a 24-month study. Patients (n = 985) were recruited from 79 investigator sites in Greece, Portugal, Romania, Sweden, and Turkey, beginning in June 2007 with visits through August 2010. Of these, 886 patients had sufficient data for assessment at baseline. Local reference costs for resource use were either incomplete or not publicly available for Portugal, Romania, and Turkey. Thus, this manuscript presents resource use data for patients from all five countries (Greece, n = 162; Portugal, n = 148; Romania, n = 207; Sweden, n = 158; and Turkey, n = 211) and cost data for patients from Greece and Sweden only.
We collected 24-month data in both studies. However, due to variable patient dropout, we present only 12-month follow-up data here. The following are the numbers of patients with visits at 24 months in INSTIGATE: 119 patients (46.5% of patients at insulin initiation) in Germany, 227 patients (86.3%) in Greece, and 152 patients (73.4%) in Spain. The following are those with visits at 24 months in TREAT: 145 patients (70.7% of patients at insulin initiation) in Greece, 107 patients (64.8%) in Portugal, 201 patients (97.1%) in Romania, 127 patients (71.3%) in Sweden, and 172 patients (74.8%) in Turkey.
Data collection
At baseline (insulin initiation), demographic, socioeconomic, and clinical characteristics of patients were recorded, including age, gender, education, occupation, duration of diabetes, body mass index (BMI), glycated hemoglobin A1c (HbA1c), insulin initiation as an outpatient or inpatient, and smoking status. Other recorded patient information included macrovascular and microvascular diagnoses and other comorbidities.
At baseline and follow-up visits ( ∼ 3, 6, 12, 18, and 24 months post-baseline), the following data on use of healthcare resources (since the last visit) were collected by the investigator:
incidence and number of outpatient clinic visits and phone calls (primary care physician [PCP], specialist nurse clinic, primary care nurse, and dietitian),
incidence and number of consultations (diabetologist or endocrinologist, ophthalmologist, internal medicine or other specialist, and chiropodist or podiatrist),
incidence and number of hospitalizations due to diabetes (including emergency room visits and overnight hospitalizations),
OAD and insulin medication use (agent and dosage), and
incidence and average number of blood glucose monitoring (BGM) tests.
Diabetes costs were evaluated from the national healthcare system (third-party payer) perspective at 2008 and 2009 prices. For each country, per-patient costs were assessed by applying local unit costs that were derived from published sources to each resource usedCitation24: clinic visit and phone call costs, consultation costs, hospitalization costs, insulin and OAD medication costs, and BGM costs. The following assumptions were employed when calculating costs: all medications were assumed to be branded formulations; when medications with multiple brand names were used, mean costs were taken; and data on the average number of BGM measurements per patient per week over the past month were used to calculate daily costs that were applied to each day over the observation interval. Data on hospitalizations for acute complications, long-term complications, and hypoglycemia were collected. Hospitalization costs were valued on the basis of cost per episode for each type of admission. Direct non-medical costs (e.g., transportation costs) and indirect costs (e.g., productivity losses) were not assessed in this study.
Statistical analyses
For both studies, sample sizes were pre-planned in the protocol and calculated by country, with the aim of providing adequate precision for the estimation of mean direct costs, assuming that 10% of data collected might be incomplete or inadequate for useCitation24,Citation25.
All statistical analyses were descriptive. Categorical variables were summarized by counts and percentages. Percentages were based on the number of patients available and included missing values. Continuous variables were summarized by standard descriptive statistics, including means and standard deviations (SD) or medians and quartiles as appropriate. Missing values were not imputed. All costs were presented as nominal values.
Results
Patient disposition
In INSTIGATE, there were 256, 263, and 207 patients at insulin initiation (baseline) in Germany, Greece, and Spain, respectively. Of those, 155, 237, and 172 patients (77.7% of those with baseline data) participated in the extension period. Thus, they had visits at 12 months or later and are included in this analysis. All these patients, except two in Germany, had 12-month visits.
In TREAT, there were 162, 148, 207, 158, and 211 patients (89.9% of those recruited) with data available at baseline in Greece, Portugal, Romania, Sweden, and Turkey and 149, 130, 204, 146, and 177 patients, respectively (91.0% of those with baseline data) with 12-month visits. The combined overall dropout rate at 12 months for both studies was 15.0%.
Baseline characteristics
Patient characteristics at baseline are shown in . In INSTIGATE, at insulin initiation, mean age ranged from 61.0 years (Germany) to 66.0 years (Greece). The percentage of male participants was 52.3–56.1%. Mean BMI ranged from 28.2 kg/m2 (Greece) to 30.6 kg/m2 (Germany). Mean duration of T2DM ranged from 6.5 years (Germany) to 11.8 years (Greece). Mean HbA1c was 9.2% for Germany and Spain and 9.6% for Greece. Hypertension was reported in 62.4–69.7% of patients and hyperlipidemia in 29.7–50.6%.
Table 1. Patient characteristics at baseline (insulin initiation).
In TREAT, at insulin initiation, mean age ranged from 56.5 years (Turkey) to 66.9 years (Greece). The percentage of male participants was 41.5–65.2%. Mean BMI ranged from 28.5 kg/m2 (Portugal) to 30.6 kg/m2 (Turkey). Mean duration of T2DM ranged from 7.6 years (Romania) to 13.9 years (Greece). Mean HbA1c ranged from 8.7% (Sweden) to 10.6% (Turkey). Hypertension was present in 66.4–74.3% of patients and hyperlipidemia in 62.0–67.3%.
Evolution of glycemic control over 12 months
Glycemic control improved in INSTIGATE and TREAT following insulin initiation, as described previouslyCitation25,Citation26. Across all countries, the largest mean decrease in HbA1c was observed at 3 months, followed by smaller mean decreases in the subsequent periods. At insulin initiation and at 12 months post-initiation in INSTIGATE, mean (SD) HbA1c was 9.2% (2.0%) and 6.7% (0.8%) in Germany, 9.7% (1.6%) and 7.4% (1.1%) in Greece, and 9.2% (1.5%) and 7.6% (1.3%) in Spain, respectively. Mean (SD) HbA1c levels at insulin initiation and at 12 months post-initiation in TREAT were 9.0% (1.7%) and 7.3% (0.8%) in Greece, 9.7% (1.9%) and 7.9% (1.3%) in Portugal, 9.9% (1.5%) and 8.0% (1.1%) in Romania, 8.7% (1.8%) and 7.3% (0.9%) in Sweden, and 10.6% (2.4%) and 8.0% (1.2%) in Turkey.
Diabetes-related resource use over 12 months
Anti-hyperglycemic medications
and summarize diabetes-related resource utilization and frequency of use in INSTIGATE and TREAT. OAD medication was used at insulin initiation by 40.0% (Germany) to 77.2% (Greece) of patients. Insulin regimens varied across countries. In INSTIGATE, most patients in Germany were initiated on prandial insulin only; in Greece and Spain, they were initiated on basal or pre-mixed formulationsCitation26. In TREAT, most patients in Greece and Sweden were initiated on long/intermediate insulin only; in Portugal and Romania, on long/intermediate and mixture only; and in Turkey, on mixture onlyCitation25.
Table 2. Diabetes-related resource utilization and frequency of use by country in INSTIGATE in the 6 months prior to the baseline and 12-month visits.
Table 3. Diabetes-related resource utilization and frequency of use by country in TREAT in the 6 months prior to the baseline and 12-month visits.
In INSTIGATE, an increase in the mean insulin dose was maximal by the 6-month visit. The mean total daily insulin doses at insulin initiation and at 6 months were 24.1 IU and 49.3 IU in Germany, 31.5 IU and 39.8 IU in Greece, and 20.4 IU and 24.0 IU in Spain. In TREAT, the mean insulin dose increased similarly, except in Turkey where insulin dose was high from initiation (34.3 IU at insulin initiation and 34.5 IU at 6 months).
BGM
BGM use in the 6 months prior to insulin initiation ranged from 52.2% of patients in Romania to 99.4% in Greece. After insulin initiation, the percentage of patients using BGM increased, ranging from 71.7% (Romania) to 100% (Germany) in the first 6 months and 80.8% (Turkey) to 100% (Germany and Greece) between 6–12 months. The intensity of BGM, indicated by the number of test strips used per patient per week, was variable between countries.
Healthcare visits
The percentage of patients visiting a PCP during the 6 months prior to initiation of insulin ranged from 42.6% (Greece) to 96.1% (Germany). This decreased slightly after initiation, ranging from 41.4% (Greece) to 84.1% (Germany) during the first 6 months and 37.6% (Greece) to 88.9% (Germany) during the subsequent 6 months. Overall, the percentage of patients visiting a primary-care nurse was highest in Spain and Romania and lowest in Greece. The percentage of patients in Germany, Greece, Portugal, Romania, and Spain consulting a diabetologist or endocrinologist in the 6 months prior to insulin initiation ranged from 59.9% (Spain) to 98.1% (Romania); in Sweden 5.7% and in Turkey 25.1% of patients consulted these specialists. The incidence of hospitalizations was highest during this period in Romania (43.0%).
Following insulin initiation, more than 75% of patients visited a specialist nurse in Germany, Portugal, and Sweden in the first 6 months (90.7%, 80.7%, and 81.6%, respectively); visits then decreased. In Sweden, 73.7% of patients had phone calls with a specialist nurse during the first 6 months. The percentages visiting a dietitian after insulin initiation were highest in Romania (40.2–44.9%) and Turkey (32.8–40.8%). The percentage consulting an internal medicine specialist was highest in Turkey, particularly after insulin initiation (68.3% in the first 6 months and 71.2% thereafter).
Total direct costs over 12 months
summarizes the mean total costs related to diabetes treatment in INSTIGATE and TREAT. In INSTIGATE, mean total costs over the 6-month period before insulin initiation in Germany, Greece, and Spain were €544.80, €495.50, and €658.50, respectively (medians: €422.90, €438.10, and €527.10). Over the 6-month period after insulin initiation, mean total costs were €982.30, €573.40, and €1084.70 (medians: €865.20, €538.10, and €694.00). In the following 6-month period (i.e., between the 6- and 12-month visits), mean total costs were €859.30, €495.80, and €646.20 (medians: €767.60, €422.80, and €530.80).
Table 4. Total per-patient direct costs related to diabetes care up to 12 months in the INSTIGATE and TREAT studies.
In TREAT, mean total costs over the 6-month period before insulin initiation in Greece and Sweden were €489.10 and €629.80 (medians: €426.60 and €548.30). Over the 6-month period after insulin initiation, mean total costs were €689.90 and €1002.70 (medians: €609.80 and €806.50). In the following 6-month period (i.e., between the 6- and 12-month visits), mean total costs were €534.70 and €523.90 (medians: €473.70 and €482.90).
Cost contributors
Results of itemized costs up to 12 months are shown in and . Itemized mean costs for Germany, Spain, and Sweden in INSTIGATE are shown in Figures 1a–c. Since Greece participated in both studies, itemized mean costs for Greece in INSTIGATE and TREAT are shown side by side in .
Figure 1. (a) Itemized mean costs for diabetes care over 12 months in Germany in INSTIGATE. (b) Itemized mean costs for diabetes care over 12 months in Spain in INSTIGATE. (c) Itemized mean costs for diabetes care over 12 months in Sweden in TREAT. Total patient numbers for Germany were 155 at insulin initiation, 151 at 6 months, and 153 at 12 months. Total patient numbers for Spain were 172 at insulin initiation, 172 at 6 months, and 172 at 12 months. Total patient numbers for Sweden were 115 at insulin initiation, 109 at 6 months, and 104 at 12 months.
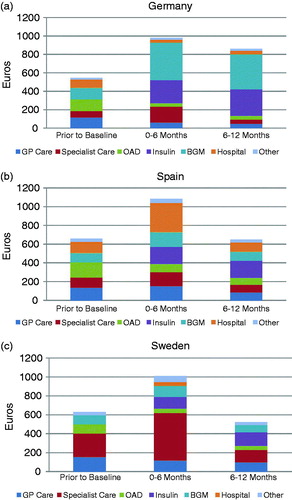
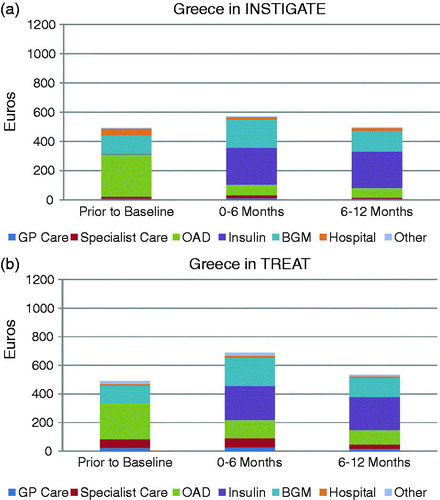
Figure 2. (a) Itemized mean costs for diabetes care over 12 months in Greece in INSTIGATE. (b) Itemized mean costs for diabetes care over 12 months in Greece in TREAT. Total patient numbers for INSTIGATE were 237 at insulin initiation, 237 at 6 months, and 237 at 12 months. Total patient numbers for TREAT were 147 at insulin initiation, 142 at 6 months, and 134 at 12 months.
During the 6 months prior to insulin initiation, in each of the four countries assessed for cost (Germany, Spain, Sweden, and Greece), OAD medication and BGM were the largest contributors to total direct cost, contributing from 15.6% (Sweden) to 58.4% (Greece) for OAD medications and 14.9% (Sweden) to 25.5% (Greece) for BGM. General practitioner (GP) care was a significant cost contributor in Germany (21.7%), Spain (20.7%), and Sweden (24.8%). Hospitalization was a significant contributor in Spain (17.8%), as was specialist care (nurse) in Sweden (38.9%).
During the 6 months after insulin initiation, the contribution of insulin to mean total cost ranged from 12.3% (Sweden) to 44.0% (Greece). The contribution of BGM to mean total cost increased in Germany from 23.5% at initiation to 41.7%, and in Greece from 25.5% and 25.3% at initiation in INSTIGATE and TREAT to 33.7% and 28.6%. The contribution of hospitalization increased in Spain (28.6% of total cost) because of eight patients with hospital stays of 1–31 days. The contribution of specialist care increased in Sweden to 49.8%. The contribution of OAD medication decreased in all countries to 4.0% (Germany) to 18.4% (Greece). That of GP care decreased in Germany (to 6.1% in the first 6 months), Spain (14.2%), and Sweden (11.8%).
Between 6 and 12 months after insulin initiation, the contribution of insulin to total cost increased in every country, ranging from 27.1% of total cost (Sweden) to 50.0% (Greece). The contributions of OAD medication and BGM changed little. The contribution of specialist care decreased in Sweden (to 24.7%) and Germany (to 5.0%).
Between the two study periods of INSTIGATE (2005–2008) and TREAT (2007–2010), we observed an increase in the cost contribution of specialist care in Greece. In INSTIGATE, the contribution of specialist care was 2.6% at insulin initiation, 3.3% after 6 months, and 1.9% between 6 and 12 months. In TREAT, the contribution of specialist care was 11.8%, 9.2%, and 5.8% at these time points.
Discussion
INSTIGATE and TREAT, two observational non-interventional studies in patients with T2DM in European countries, assessed diabetes-related resource utilization and direct costs before and after insulin initiation. The data for INSTIGATE for the first 6 months after insulin initiation have been publishedCitation24. It was found that, in all countries, the mean total direct cost of care for diabetes increased after initiating insulin. Itemized costs varied considerably across countries, reflecting differences in resource use patterns, prices of medical resources, and different healthcare systems. The current analysis extends these previously published findings to 12 months in INSTIGATE and to the TREAT study. Trends in resource use and cost contributions beyond 12 months remained consistent through 24 months in the two studies (data not shown).
Resource use before and after initiation of insulin varied among countries in TREAT, as it did in INSTIGATE. After insulin initiation, use of BGM increased and then stabilized. Depending on country, other resource use increased during the 6 months after insulin initiation and then decreased, including visits to a primary care nurse in Spain and Romania; visits to a specialist nurse in Germany, Portugal, and Sweden; and specialist nurse phone calls in Sweden.
Mean total direct cost of diabetes care increased in all countries during the first 6 months after insulin initiation in INSTIGATECitation24, which was also observed among the countries in TREAT in this analysis. Subsequently in both studies, mean direct costs returned to baseline or near-baseline values in every country except Germany, in which mean total cost remained higher than baseline. During the first 6 months, observed increases in mean direct costs compared with the 6 months prior to insulin initiation ranged from 16 to 80%.
The increase in cost was attributable to increased use and dose escalation of insulin during the first 6 months after initiation. The relative differences in insulin costs between countries in INSTIGATE and TREAT partly reflected differences in dosing as well as relative percentages of human insulin vs insulin analogs. In Germany and Greece, the costs associated with BGM increased as well. In Germany and Sweden, costs for specialist care increased. In Spain, costs for hospital visits, driven by extended hospital stays, increased. However, costs associated with OAD medication decreased in all countries, with a substantial number of patients on either one OAD treatment or none at insulin initiation (data not shown). Thus, it is possible that the increased costs associated with insulin treatment were offset by other cost reductions. In Germany, the combined decrease in cost contributions of healthcare professionals (HCPs) and OAD medication was ∼−30%, potentially offsetting the cost of insulin. In Spain, the decrease in cost contributions of HCPs and OAD medication was ∼−25%. In Sweden, the decrease in cost contribution of OAD medication was ∼−10%. In Greece, the decrease in cost contribution of OAD medication was ∼−45% in INSTIGATE and −35% in TREAT. Subsequently, among the four countries, mean total cost decreased by −13% to −48% in the 6 months prior to the 12-month visit compared with the 6-month visit, presumably offsetting additional costs of insulin treatment.
An initial increase in mean direct costs of diabetes care during the first few months after insulin initiation followed by a decrease has been observed in other studies. Rosenblum and KaneCitation27, in a managed care organization in the US, showed that total healthcare expenditures increased by ∼10% during the first 2 months after insulin initiation and then decreased by 40% by the end of 9 months.
Of the countries in INSTIGATE, Germany had the highest percentage of basal/bolus regimens initially prescribed (n = 46; 29.7%), with the highest mean daily dose of insulin (49.3 IU; 0.53 IU/kg) at 6 months and the highest mean number of BGM tests ( ∼ 20 test strips per week) after insulin initiationCitation28. These results may have been influenced by the fact that only diabetologists, who may initiate more intensive insulin regimens than general practitioners, participated in this study in GermanyCitation21. In Spain, the mean daily insulin dose at the 6-month visit after insulin initiation (24.0 IU; 0.31 IU/kg) was approximately half of that in Germany, possibly reflecting that approximately two-thirds (67.4%) of patients in Spain were initiated on long/intermediate insulin only and approximately one-fifth (20.9%) were initiated on mixtures. Patients in Germany reached a mean HbA1c level of 6.7% at the 12-month visit, which was the lowest level achieved in this group of countries. Thus, the higher cost of more intensive insulin regimens and BGM in Germany, associated with better glycemic control, may result in fewer complications and lower complication-related costs in the long-term. Insulin was, however, on average, initiated later than recommended guidelinesCitation9 in all countries, including Germany, with a mean baseline HbA1c of 9.2%.
Long-term insulin therapy has the potential to result in overall cost savings, because better glycemic control may be associated with less resource utilization on diabetes-related complications. It has been shown that care for chronic complications, including hospital care, represents ∼70% of all diabetes-related costsCitation3. Typically for managed care organizations in the US, only 20–30% of overall diabetes costs are attributable to pharmacy costsCitation7. Approximately one-third of pharmacy costs are directly related to glycemic control, and the remainder is related to microvascular and macrovascular complications and other diabetes-related conditionsCitation3,Citation7. Improvements in glycemic control have been associated with lower overall per-patient direct costs in managed care organizationsCitation7. Thus, sustained improvements in glycemic control may lower the risk of severe chronic complications of diabetes and, thereby, decrease the overall cost of disease, despite increased costs at insulin initiation.
In INSTIGATE and TREAT, a mean HbA1c of 7.3–8.0% was observed after 1 year of insulin treatment in most countries and of 6.7% in Germany. After 2 years of insulin treatment, overall mean HbA1c further decreased to 7.6% in TREAT, regardless of the starting insulin regimenCitation25. Thus, it seems reasonable that a mean HbA1c of ∼7.5% can be achieved with insulin treatment and at minimal cost increment vs previous oral therapy. To reach glycemic control below 7.5% would require more intensive BGM and/or insulin dose adaptation and consequently would increase the cost of insulin therapy, as observed for Germany in INSTIGATECitation20. However, there is no definite proof that lower HbA1c levels are beneficial relatively late in diabetes treatment, especially in patients with existing complicationsCitation9, vs improvement of other risk factors such as hypertension and dyslipidemia that are insufficiently controlled, as in this study, and easierCitation29 and less expensive to manage. Currie et al.Citation30 have shown accordingly in patients on insulin in the UK, in a general practice database, that the adjusted hazard ratio for all-cause mortality had a U shape, with the lowest ratio at an HbA1c of 7.5%.
Diabetes care differs between countries. In Romania, the National Health Insurance Company contracts with diabetes specialists to provide patients with free treatment, including consultations, OAD medication, and insulinCitation31. However, some resources, such as glucose meters and strips for insulin-treated patients, are rationed. Our findings are consistent with these healthcare policies. In TREAT, 100% of patients in Romania consulted with a diabetologist or endocrinologist, consistent with the availability of free consultations. Further, relative to other countries in the TREAT study, the percentage of patients using BGM were low prior to insulin initiation (52.2%) and the 6-month visit (71.7%). In Sweden, the Swedish Health Care system for patients with diabetes is managed by specialist nurses in addition to specialists in internal medicine, endocrinology or diabetology, and general medicineCitation13. This is consistent with our findings in the TREAT study that Sweden had the highest use of specialist nurses, with 81.6% of patients making visits and 73.7% making phone calls. In Greece, we observed an increased cost contribution of specialist care in the later TREAT study, in which participating physicians were primarily involved in private practice; physicians in INSTIGATE were employed in hospitalsCitation21.
Limitations of this study include 15% of patients who were lost to follow-up overall during the first 12 months after insulin initiation, which may have introduced a bias if those lost to follow-up had different characteristics than those who continued in the studyCitation26,Citation32. The centers that participated in these studies may not have represented fully all levels of care in the participating countries. Under-estimation of costs may have been possible due to retrospective data collection at some time points. OAD medications and insulin were assumed to be branded. Resource use and costs were not pro-rated to account for variable durations of follow-up; therefore, care should be exercised in interpreting these data per study visit. Strengths of this study include 1-year data that reflect the impact of insulin initiation on resources and costs in several European countries in which these data previously were limited. Although exploratory in nature, these findings highlight important trends in costs and resource use for insulin initiation as well as implications for local patterns of diabetes care.
Conclusions
In each of the European countries of the INSTIGATE and TREAT observational studies, initiation of insulin therapy was accompanied by additional resources and costs that varied between countries. Mean total direct cost of diabetes care increased in the 6 months after insulin initiation and returned to baseline or near-baseline values in the next 6 months in Greece, Spain, and Sweden and remained higher than baseline in Germany. After insulin initiation, use and mean cost of BGM and insulin increased, while mean costs associated with OAD medication decreased.
Transparency
Declaration of funding
This study was funded by Eli Lilly and Company and/or one of its wholly-owned subsidiaries (Lilly).
Declaration of financial/other relationships
KB and MB declare no competing interests. CN, HS, and MR are employees of and stock holders in Lilly. JG is a medical writer whose writing support was funded by Lilly.
Acknowledgments
We are grateful to the INSTIGATE and TREAT clinical investigators for their support in this study.
References
- World Health Organization. Noncommunicable diseases country profiles 2011. WHO report. Geneva, Switzerland: WHO Press, World Health Organization, 2011. http://whqlibdoc.who.int/publications/2011/9789241502283_eng.pdf. Accessed March 2013
- Stratton IM, Adler AI, Neil HA, et al. Association of glycaemia with macrovascular and microvascular complications of type 2 diabetes (UKPDS 35): prospective observational study. BMJ 2000;321:405-12
- Henriksson F, Agardh CD, Berne C, et al. Direct medical costs for patients with type 2 diabetes in Sweden. J Intern Med 2000;248:387-96
- Bjork S. The cost of diabetes and diabetes care. Diab Res Clin Pract 2001;54:S13-18
- Massi-Benedetti M; CODE-2 Advisory Board. The cost of diabetes Type II in Europe: the CODE-2 Study. Diabetologia 2002;45:S1-4
- Killilea T. Long-term consequences of type 2 diabetes mellitus: economic impact on society and managed care. Am J Manag Care 2002;8(16 Suppl):S441-9
- Stephens JM, Botteman MF, Hay JW. Economic impact of antidiabetic medications and glycemic control on managed care organizations: a review of the literature. J Manag Care Pharm 2006;12:130-42
- Williams R, Van Gaal L, Lucioni C; CODE-2 Advisory Board. Assessing the impact of complications on the costs of Type II diabetes. Diabetologia 2002;45:S13-17
- Inzucchi SE, Bergenstal RM, Buse JB, et al. Management of hyperglycaemia in type 2 diabetes: a patient-centered approach. Position statement of the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD). Diabetologia 2012;55:1577-96
- International Diabetes Federation Clinical Guidelines Task Force. Global Guideline for Type 2 Diabetes. International Diabetes Foundation clinical practice guideline. Brussels, Belgium: International Diabetes Foundation, 2012. http://www.idf.org/guidelines. Accessed March 2013
- Rodbard HW, Jellinger PS, Davidson JA, et al. Statement by an American Association of Clinical Endocrinologists/American College of Endocrinology consensus panel on type 2 diabetes mellitus: an algorithm for glycemic control. Endocr Pract 2009;15:540-59
- Turner RC, Cull CA, Frighi V, et al; UK Prospective Diabetes Study (UKPDS) Group. Glycemic control with diet, sulfonylurea, metformin, or insulin in patients with type 2 diabetes mellitus: progressive requirement for multiple therapies (UKPDS 49). JAMA 1999;281:2005-12
- Gudbjörnsdottir S, Cederholm J, Nilsson PM, et al; Steering Committee of the Swedish National Diabetes Register. The National Diabetes Register in Sweden: an implementation of the St. Vincent Declaration for Quality Improvement in Diabetes Care. Diabetes Care 2003;26:1270-6
- UK Prospective Diabetes Study (UKPDS) Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet 1998;352:837-53
- Baser O, Bouchard J, DeLuzio T, et al. Assessment of adherence and healthcare costs of insulin device (FlexPen) versus conventional vial/syringe. Adv Ther 2010;27:94-104
- International Diabetes Federation--European Region and the Federation of European Nurses in Diabetes. Diabetes. The policy puzzle: is Europe making progress? Brussels, Belgium: The International Diabetes Federation Europe and Federation of European Nurses in Diabetes, 2008. http://ec.europa.eu/health/major_chronic_diseases/docs/policy_puzzle_2008.pdf. Accessed March 2013
- IDF Diabetes Atlas, 4th ed. Brussels, Belgium: The International Diabetes Federation, 2009. http://www.diabetesatlas.org/content/diabetes-and-impaired-glucose-tolerance. Accessed March 2013
- Leese B. Economic evaluations of type II diabetes. Pharmacoeconomics 1995;8(1 Suppl):23-7
- Ettaro L, Songer TJ, Zhang P, et al. Cost-of-illness studies in diabetes mellitus. Pharmacoeconomics 2004;22:149-64
- Liebl A, Breitscheidel L, Nicolay C, et al. Direct costs and health-related resource utilisation in the 6 months after insulin initiation in German patients with type 2 diabetes mellitus in 2006: INSTIGATE study. Curr Med Res Opin 2008;24:2349-58
- Jones S, Benroubi M, Castell C, et al. Characteristics of patients with type 2 diabetes mellitus initiating insulin therapy: baseline data from the INSTIGATE study. Curr Med Res Opin 2009;25:691-700
- Costi M, Dilla T, Reviriego J, et al. Clinical characteristics of patients with type 2 diabetes mellitus at the time of insulin initiation: INSTIGATE observational study in Spain. Acta Diabetol 2010;47(1 Suppl):169-75
- Liebl A, Jones S, Benroubi M, et al. Clinical outcomes after insulin initiation in patients with type 2 diabetes: 6-month data from the INSTIGATE observational study in five European countries. Curr Med Res Opin 2011;27:887-95
- Jones S, Castell C, Goday A, et al. Increase in direct diabetes-related costs and resource use in the 6 months following initiation of insulin in patients with type 2 diabetes in five European countries: data from the INSTIGATE study. Clinicoecon Outcomes Res 2012;4:383-93
- Oguz A, Benroubi M, Brismar K, et al. Clinical outcomes after 24 months of insulin therapy in patients with type 2 diabetes in 5 countries: results from the TREAT Study. Curr Med Res Opin 2013: published online 9 May 2013, doi: 10.1185/03007995.2013.803053
- Liebl A, Jones S, Goday A, et al. Clinical outcomes after insulin initiation in patients with type 2 diabetes: 24-month results from INSTIGATE. Diabetes Ther 2012;3:9
- Rosenblum MS, Kane MP. Analysis of cost and utilization of health care services before and after initiation of insulin therapy in patients with type 2 diabetes mellitus. J Manag Care Pharm 2003;9:309-16
- Smith HT, Liebl A, Jones S, et al. Cost and resource use following insulin initiation in Europe: 24 month follow up data from the INSTIGATE study. Vienna, Austria: EASD, 2009. Diabetologia
- Gaede P, Vedel P, Larsen N, et al. Multifactorial intervention and cardiovascular disease in patients with type 2 diabetes. N Engl J Med 2003;348:383-93
- Currie CJ, Peters JR, Tynan A, et al. Survival as a function of HbA(1c) in people with type 2 diabetes: a retrospective cohort study. Lancet 2010;375:481-9
- Doničová V, Brož J, Sorin I. Health care provision for people with diabetes and postgraduate training of diabetes specialists in eastern European countries. J Diabetes Sci Technol 2011;5:1124-36
- Liebl A, Breitscheidel L, Benter U, et al. Start der Insulintherapie bei Typ-2-Diabetes: 1-Jahres-Daten der INSTIGATE-Studie [Initiation of Insulin Therapy in Type 2 Diabetics: One-Year Results from the INSTIGATE Study (German 12-month data)]. Diabetes, Stoffwechsel und Herz 2012;21:13-19