

Abstract
Objective:
This study compares the cost-effectiveness of intravitreal ranibizumab vs observation and/or laser photocoagulation for treatment of macular edema secondary to retinal vein occlusion in a UK-based model.
Methods:
A Markov model was constructed using transition probabilities and frequency of adverse events derived using data from the BRAVO, CRUISE, and HORIZON trials. Outcomes associated with treatments and health states were combined to predict overall health costs and outcomes for cohorts treated with each option.
Results:
In branch retinal vein occlusion, ranibizumab produced a gain of 0.518 quality-adjusted life years at an incremental cost of £8141, compared with laser photocoagulation. The incremental cost-effectiveness ratio was £15,710 per quality-adjusted life year, and the incremental cost per month free from blindness was £658. In central retinal vein occlusion, ranibizumab produced a gain of 0.539 quality-adjusted life years at an incremental cost of £9216, compared with observation only. The incremental cost-effectiveness ratio was £17,103, and the incremental cost per month free from blindness was £423.
Conclusions:
These incremental cost-effectiveness ratios are below the £20,000–30,000 range typically accepted as a threshold for cost-effectiveness. This suggests that ranibizumab may be regarded as a cost-effective therapy for patients with macular edema secondary to retinal vein occlusion, relative to grid laser photocoagulation (for BRVO) and observation (for CRVO). Limitations include sparse data for utilities associated with the severity of visual impairment in the WSE in patients with RVO. A lack of direct comparative evidence between ranibizumab and the dexamethasone intravitreal implant for the treatment of BRVO and CRVO and the infeasibility of an indirect comparison due to significant heterogeneity in trial designs prevented the inclusion of this treatment as a comparator in the Markov model.
Introduction
Retinal vein occlusion (RVO) is an important cause of vision loss among elderly adultsCitation1 and may involve the central or branch retinal veinsCitation2. Occlusion of the retinal veins causes an increase in retinal capillary pressure resulting in up-regulation of vascular endothelial growth factor (VEGF) expression and a consequent increase in vascular permeability and new vessel proliferation within the iris and anterior chamber. As a result, blood and plasma are discharged into the retina, often causing complications including macular edema (MO) and varying degrees of ischemia, potentially leading to severe vision loss.
MO secondary to RVO can lead to a significant decrease in vision-related quality-of-lifeCitation3,Citation4. The prognosis for branch RVO (BRVO) is frequently more favorable than that for central RVO (CRVO)Citation2. The current standard of care for BRVO, according to National Institute for Health and Care Excellence (NICE) guidelines, is grid laser photocoagulation, which aims to preserve vision while minimizing complicationsCitation5,Citation6. However, recent RCT evidence indicates that anti-VEGF therapies are significantly more effective at improving BCVA than laser photocoagulationCitation7. Anti-VEGF therapy is now the standard of care for CRVO, replacing an observation-only approach which used rescue pan-retinal laser photocoagulation in the case of rubeosis iridis developmentCitation8–10. The dexamethasone intravitreal implant has received a UK marketing authorization for MO secondary to either BRVO or CRVO. Laser anastomosis and optic nerve sheathotomy are surgical procedures that have been studied in clinical trials, but these options are rarely undertaken in current clinical practiceCitation11.
This study aimed to compare the cost-effectiveness of using ranibizumab vs observation for CRVO and vs grid laser photocoagulation therapy for BRVO. The perspective of the evaluation was that of the National Health Service (NHS) in England and Wales, as cost and resource use data from England were used.
Ranibizumab (Lucentis®, Genentech Inc., San Fransisco, CA and Novartis Pharma AG, Basel, Switzerland) is an anti-VEGF drug licensed for the treatment of patients with MO secondary to RVO. It is administered as an intravitreal injection and has a recommended posology of 0.5 mg once per month for 3 months and as required thereafter, based on clinical outcomesCitation12. Ranibizumab has been studied in three pivotal RVO studies: BRAVO, which evaluated the treatment with ranibizumab in BRVOCitation13; CRUISE, which evaluated the treatment with ranibizumab in CRVOCitation14; and HORIZON (Cohort 2, comprising patients with MO after RVO who had completed the BRAVO and CRUISE studies)Citation15–17. BRAVO and CRUISE efficacy and safety data were used to populate year 1 of the model, and HORIZON data were used to populate year 2.
The primary end-point for BRAVO and CRUISE was the mean change in best-corrected visual acuity (BCVA) letter score from baseline to month 6. The two studies demonstrated that ranibizumab 0.5 mg led to a statistically greater increase in BCVA compared with the control (in BRAVO, the change was +18.46 compared with +7.17 for ranibizumab and grid laser therapyCitation14, respectively, while CRUISE reported changes of +14.81 for ranibizumab compared with +0.92 for the sham injection)Citation13. Improvement in BCVA reported at 6 months was sustained when patients were treated for up to 12 monthsCitation15,Citation16.
Materials and methods
Model structure
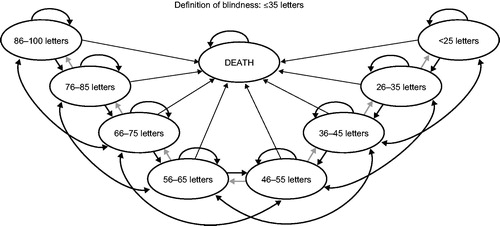
A Markov model for MO secondary to RVO was developed in Microsoft Excel. Patients moved between nine different health states at monthly intervals (cycles). The health states were based on eight different BCVA intervals, using the Early Treatment Diabetic Retinopathy Study (ETDRS) letter scaleCitation18 and a ninth state, ‘death’ ().
Figure 1. Model structure. Although different scales (e.g., logMAR, Snellen) exist to measure the severity of a patient’s visual impairment, the Early Treatment of Diabetic Retinopathy Study letter scale was chosen for this model because it is commonly used in clinical trials and is the scale used in the BRAVO and CRUISE clinical studies.
This model aimed to predict changes in BCVA, utility, resource use and costs in each patient with visual impairment due to MO secondary to RVO. Using monthly cycles in the first year, the model predicted each patient’s health state based on outcomes from BRAVO for ranibizumab vs grid laser photocoagulationCitation14 and from CRUISE for ranibizumab vs sham injection/observationCitation13.
The base-case analysis assumed a lifetime time horizon (i.e. follow-up of all patients until death) and applied a discount rate of 3.5% to costs and benefits, in line with UK guidelines for economic evaluation and health technology assessmentCitation19.
Treatment effectiveness
The model’s clinical inputs in year 1 were driven by data from the BRAVO and CRUISE trials (). Patient-level data were used to calculate monthly transition probabilities for each treatment arm separately. For ranibizumab, data from the 0.5 mg arm in BRAVO and CRUISE for up to 12 months were used. Transition probabilities for grid laser photocoagulation in BRVO were estimated from the active control arm of BRAVO for 6 months, because laser treatment in that trial was applied as per standard of care; thereafter, laser treatment was assumed to follow the same transition probabilities as ranibizumab. For observation in CRVO, transition probabilities were estimated from the control arm of CRUISE for 6 months and, for months 7–12, the same probabilities were assumed as for months 2–6 (the first month is omitted in order to avoid bias introduced by spontaneous resolution during this early period). Effectiveness data for ranibizumab in year 2 were drawn from the HORIZON (Cohort 2) study. In the absence of clinical trial data beyond year 2, it was assumed that patients achieved stability by the end of year 2 except for the natural aging effect of a progressive decrease in BCVA based on advice received from experts.
Table 1. Model inputs for effectiveness data (and adverse event rates for ranibizumab only).
Deterioration in BCVA was integrated into the model from year 3 onwards using data sourced from a population-based observational studyCitation20. This study reported that the number of patients with ‘mild’ symptoms increased from 2% in patients aged 43–54 to 9.4% between the ages of 65–74; the increase from ‘no problems’ to ‘mild’ is equivalent to around 2 lines of letters. Therefore, it was assumed that 7.4% of patients would worsen by this magnitude of reduced letter score over a period of 20 years, based on the assumption that no injections are administered from year 3 onwards, as described below. This progression rate was converted into a monthly probability for inclusion in the model, which translated to a probability of losing 2–4 lines of 0.031% per monthly cycle. The following formula was used for the above-mentioned conversion:
The economic model follows each patient’s BCVA in the treated eye, which in some cases was the better-seeing eye (BSE), due to ocular comorbidities in the fellow eye; in other cases it was the worse-seeing eye (WSE). Based on the proportions of patients in BRAVO and CRUISE whose study eye was the BSE or WSE at baseline, it was assumed that 10% of treatments would be in the patient’s BSE, rising to 21.5% at 12 months (due to two factors: first, the expectation that treatment would improve the BCVA in the study eye to the extent that, in some cases, it would become the patient’s BSE, and second, that the fellow eye would also become affected in some patients). The proportion of patients treated in their BSE impacts on the calculations for quality-of-life and mortality, because both use a weighted approach based on the number of patients with BCVA that is representative of their BSE and WSE, respectively.
Mortality
All-cause mortality was included in the model, using annual rates based on life tables for England and Wales. Studies have demonstrated a relationship between BCVA and risk of mortalityCitation21–23, with one study presenting results specific to patients with RVOCitation23. It is, therefore, appropriate to assume that the worsening of BCVA in RVO is associated with increased mortality. When the BSE was affected, the risk ratio (RR) applied to each BCVA band was 1.00 for BCVA letter scores above 56, 1.23 for letter scores between 36–55, and 1.54 for letter scores below 36Citation21. When the WSE was affected, a risk ratio was used only for BCVA levels below 35 letters score, and a ratio of 1.23 was then appliedCitation21.
Adverse events
For grid laser photocoagulation and observation, it was assumed that no ocular adverse events would be observed due to the limited data available on the occurrence of these adverse events. This conservative assumption is supported by 12-month results from SCORECitation6. Ocular adverse event frequencies for ranibizumab were included in the model based on combined rates observed within BRAVO and CRUISE. The rationale for including each adverse event was based on the relative prevalence and severity of each event (i.e., infrequent and non-severe events and events not associated with increased health resource utilization were not included). The rates of adverse events differed in the first and second years of treatment ().
Table 2. Adverse event rates in years 1 and 2.
Fellow eye involvement
Fellow eye involvement (FEI) was assumed not to impact on the effectiveness of treatment in the model, as there are no data to indicate the relationship between the outcomes in each individual eye. The model was, therefore, built to capture only the cost implications of FEI (i.e. the occurrence of RVO in both of the patient’s eyes), which is a conservative assumption. When RVO occurred in the fellow eye, the cost of treatment was effectively doubled for those patients (because two eyes would be treated), although the cost of administration and follow-up was assumed to remain the same, since both eyes could be assessed at the same visit; however, bilateral involvement is often asynchronous.
The rate of FEI was assumed to be 6.5% at 12 months and 10% at 6 years. After 6 years, the rate for FEI was assumed to remain stable at 10%. These assumptions were previously used in a health technology assessment submission to NICE and were deemed by NICE to be plausibleCitation24.
Utilities
It is generally understood that quality-of-life in people with visual impairment is associated primarily with BCVA in the BSE. Utility values are usually considered to be lower in patients whose affected eye is the BSE than in those whose affected eye is the WSE, while utility gains from improving BCVA would generally be higher among patients treated in the BSE than in those treated in the WSE, although this has not been thoroughly investigated. It was, therefore, important to choose utilities that were specific to BSE or WSECitation25. Utilities by BCVA letter score were built into the model based on the algorithm developed by Czoski-Murray et al.Citation26 and were used as the base-case for the BSE in the model, as these utilities adjust for age and reflect the societal value of visual impairment. In the absence of appropriate data for the WSE, it was assumed that patients could experience a maximum gain in utility score of 0.30 between the best and worst possible health states (this compares with 0.52 in the Czoski-Murray et al. algorithm for the BSE). These utility scores are shown in . Disutilities were applied to each patient experiencing an adverse event in the model, and were calculated as one-off events per patient, weighted by the expected duration of the quality-of-life impact.
Table 3. Utility scores by health state.
Resource use
The frequency of ranibizumab treatment during year 1 was taken from BRAVO and CRUISE directly (). This may be a conservative assumption given that patients were treated with a fixed 6-month regimen at the start of the trial, followed by as-needed dosing (this is different from the posology in the Committee for Medicinal Products for Human Use label). Year 2 rates for ranibizumab treatment were drawn from the HORIZON study, after excluding patients who did not enter the extension study. From year 3 onwards it was assumed that no injections would be required because it was expected that patients’ BCVA would have stabilized by then based on advice received from experts. It was assumed that patients would be followed-up monthly during year 1, and that most patients would attend bi-monthly monitoring during year 2.
Table 4. Frequency and cost of treatment and follow-up.
For grid laser photocoagulation in patients with BRVO, treatment frequency was taken from the SCORE trial for years 1 and 2Citation6, because patients in BRAVO were switched to ranibizumab treatment after 6 months and this would have reduced their use of laser treatmentCitation15. No laser treatment was assumed from year 3 onwards. In addition, patients were assumed to have quarterly visits from year 1 onwards. A similar pattern of follow-up was assumed for observation in patients with CRVO, although in some countries CRVO patients may be followed more closely to assess the development of rubeosisCitation2.
Costs
The level of resource use previously described was multiplied by unit costs in order to derive total costs. Unit costs were obtained from published UK sources in order to calculate the cost per intervention, for each of the treatments ()Citation27. Patients experiencing adverse events were assumed to incur the cost of managing those events. These NHS reference costs included £800.00 for the treatment of cataract, £31.67 for drug-treated intra-ocular pressure (IOP), and £872.63 for surgery ()Citation27.
A systematic review of published literature found no evidence of a link between disease severity and resource use in RVO. However, patients considered to be blind (BCVA letter score below 6/60 [ETDRS letters score lower than 35] in the BSE) have been demonstrated to incur significant costs. The costs associated with blindness were drawn from a previously published studyCitation28 and were inflated to 2011 pricesCitation29. The above-mentioned costs for blindness were applied when the patient is affected in the BSE and the BCVA letter score falls below 35.
Sensitivity analysis
One-way sensitivity analyses were performed when there was uncertainty about key parameter values. This enabled identification of the impact of different parameters on the costs and effects of treatment alternatives. These parameters are described in . In addition, a probabilistic sensitivity analysis (PSA) was performed. To do this, distributions were fitted to key parameters within the model (). For probabilities, beta-distributions were used, while cost parameters were fitted with gamma-distributions (beta-distributions are bound between the values of 0 and 1, whereas gamma-distributions produce only non-negative values). Normal distributions were assumed for parameters such as age, for which non-negative values were very unlikely, and log-normal distributions were used for risk ratios. For parameters such as the transition probability rates, the beta-distribution was determined by the trial results. Specifically, the α-input for each probability was represented by the number of patients who moved health state, while the β-value was determined by the number who did not move to that state.
Table 5. Parameter values for probabilistic sensitivity analyses.
Results
In BRVO, ranibizumab was shown to produce a gain of 0.518 quality-adjusted life years (QALYs) at an incremental cost (including drug acquisition, administration, monitoring and the cost of blindness) of £8141 when compared with grid laser photocoagulation over a lifetime horizon (). The incremental cost-effectiveness ratio (ICER) was, therefore, £15,710 per QALY. This result is below the £20,000–30,000 range, which has typically been regarded as a threshold for cost-effectiveness in the UK. In addition, the incremental cost per month free of blindness was £658.
Table 6. Base case cost-effectiveness results.
In CRVO, ranibizumab was shown to lead to a gain of 0.539 QALYs at an incremental cost of £9216 when compared with best supportive care (observation). The ICER was, therefore, £17,103 per QALY. The incremental cost per month free from blindness was £423 (). The results of the one-way sensitivity analysis are shown in , whilst the probabilistic scatter plots and cost-effectiveness acceptability curves (CEACs) are shown in .
Figure 2. Sensitivity analysis tornado diagrams for (a) BRVO and (b) CRVO.
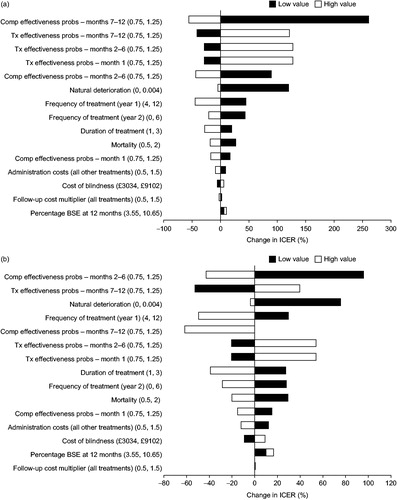
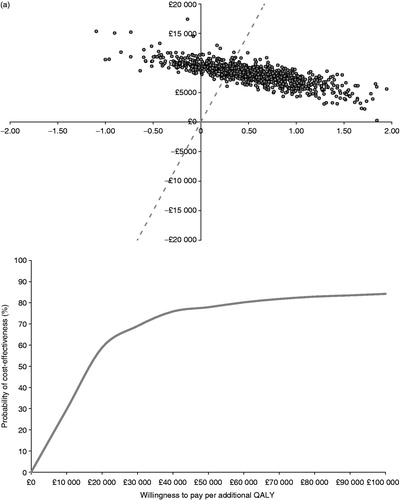
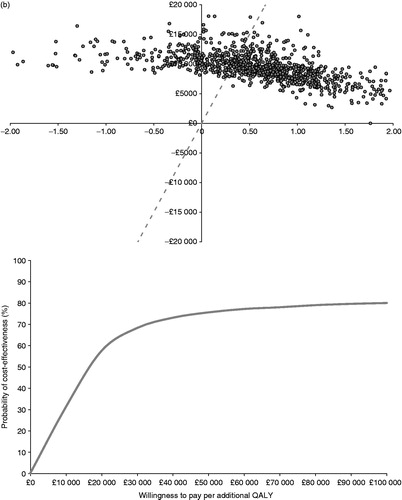
Figure 3. Probabilistic scatter planes and cost-effectiveness acceptability curves for (a) BRVO and (b) CRVO.
As shown in the one-way sensitivity analysis, when the rate of natural deterioration of BCVA was increased, or when the overall mortality rate increased, the treatment became less cost-effective. This is because the ‘capacity to benefit’ (through duration of benefit) is reduced and any benefits of treatment are lost sooner. The model is relatively sensitive to the cost associated with blindness (i.e. when the patient’s BCVA in the BSE falls below 35 letters). Again, this is to be expected, because one of the key benefits of effective treatment is to reduce the burden of patients whose sight becomes significantly affected by the disease.
The PSA allows an overall assessment of the uncertainty within the model; it generates a ‘scatter plot’, which has a ‘downward-sloping’ pattern. This represents the likely inverse relationship between incremental cost and incremental effectiveness. For example, if the PSA distributions randomly generate a ‘favorable’ iteration (i.e., when treatment is much more effective than the comparator), this is likely to have two effects. First, the patient will gain QALYs through improved quality-of-life and, to a much lesser extent, through increased survival. Second, the patient will be likely to avoid costly complications such as blindness and will, therefore, see their incremental cost reduced. Similarly, a ‘less favorable’ iteration will see reduced QALYs and increased long-term costs. The PSA found that, when there is a willingness-to-pay threshold of £20,000 for each QALY gained, the probability of ranibizumab being cost-effective is 58.8% and 57.6% in BRVO and CRVO, respectively (). At a willingness-to-pay threshold of £30,000 per QALY gained, the probability of ranibizumab being cost-effective is 69.0% for BRVO and 68.3% for CRVO.
Discussion
A key strength of economic models is that they allow the decision-maker to combine evidence from a variety of sources in order to derive a single assessment of the impact of an intervention upon utilities, survival, and overall treatment costs.
The model used in this analysis was based mainly on data derived from the BRAVO, CRUISE, and HORIZON (Cohort 2) trials. This allows for a robust comparison of ranibizumab vs grid laser photocoagulation (for BRVO) and observation (for CRVO). The results confirm that ranibizumab is a cost-effective treatment for patients with MO secondary to RVO relative to the current standard of care for BRVO and to observation for CRVO. There remains some uncertainty over the long-term comparative impact of treatment over the comparator, because all patients in BRAVO and CRUISE were able to receive ranibizumab after 6 months; future clinical trials are needed to evaluate this.
In this analysis, conservative assumptions were made for months 7–12 and in the second year of the model, assuming that transition probabilities were identical for ranibizumab and the standard of care arm for BRVO. For CRVO, the probabilities for observation were assumed to be the same as for months 2–6 during the rest of the first year, and stability was assumed for the second year. Given the significantly better outcomes observed for ranibizumab than control in the initial 6 months of the trials, this would seem to be a conservative approach, although it is also acknowledged that the potential delayed onset of effectiveness associated with grid laser photocoagulation could partially offset this. The model also assumes that patients achieve stability in visual acuity by the end of year 2 and, therefore, that no injections are required from year 3 onwards. The HORIZON trial reported a slight decline in visual acuity in patients with CRVO associated with fewer injections in the second yearCitation17; however, additional long-term clinical data will be needed to determine the long-term trajectory for visual acuity in patients treated with ranibizumab for MO secondary to RVO. When these become available, they may be incorporated into a future model.
A key limitation of the analysis is the lack of accurate data for utilities associated with the severity of visual impairment in the WSE in patients with RVO. While several studies have estimated utilities in patients based on the BCVA letter score in their BSE, there is very little evidence related to utilities based on BCVA in the WSE of patients. It is worth noting that the absolute value of utility does not drive the results of the model, but rather the incremental QALYs gained are largely driven by the slope of the utility curve. It is difficult to quantify the benefit of improving the BCVA in a patient’s WSE, and, therefore, it seems appropriate that future studies aim to distinguish the impact on utility of BCVA in the BSE and WSE.
Ideally, both of the patients’ eyes would be modeled simultaneously using a patient-level simulation to establish the BCVA in each eye. Although the computational burden of this approach is manageable, the evidence available to populate such a model is sparse, especially in RVO. Such a model would require detailed data on the complex relationship between BCVA in each eye, which was beyond the scope of this paper.
Dexamethasone intravitreal implants are also approved for the treatment of patients with MO secondary to RVOCitation30,Citation31. While laser photocoagulation (for BRVO) and observation (for CRVO) are the most appropriate comparators for ranibizumab, it would be desirable to also compare the cost-effectiveness of the dexamethasone implant with ranibizumab. However, there is a lack of direct evidence comparing ranibizumab and the dexamethasone implant for the treatment of BRVO and CRVO, preventing comparison using standard methods for the outcomes needed for this Markov model. Moreover, the studies and enrolled populations are too heterogeneous to permit an unbiased indirect comparisonCitation32. Further studies with direct comparisons between ranibizumab and the dexamethasone implant, or sophisticated and robust indirect treatment comparisons, would be needed before the cost-effectiveness of these two therapies can be evaluated robustly and compared.
Conclusion
In summary, the existing clinical and economic evidence suggest that ranibizumab is a cost-effective treatment for patients with MO secondary to RVO relative to grid laser photocoagulation (for BRVO) and to observation (for CRVO). The present study demonstrates that the significant gains in BCVA with ranibizumab lead to significant benefits for patients, while treatment costs are to a large extent compensated by the avoidance of blindness and visual impairment in a significant proportion of patients.
Transparency
Declaration of funding
This study was funded by Novartis Pharma AG.
Declaration of financial/other relationships
Matthew Taylor, Elçin Serbetci, and Lily Lewis are employees of York Health Economics Consortium Ltd. Alberto Ferreira is an employee of Novartis and owns shares in the company. Kerry Gairy was an employee of Novartis Pharmaceuticals UK Limited, Surrey, UK at the time the study was conducted. Julie Blouin was an employee of Novartis Pharmaceuticals Canada Inc. Dorval, Quebec, Canada at the time the study was conducted. Paul Mitchell is an academic and has received honoraria and travel support from Novartis and Bayer as a consultant. JME Peer Reviewers on this manuscript have no relevant financial relationships to disclose.
Acknowledgments
This manuscript has been prepared with editorial assistance from Dr Martin Bell of Oxford PharmaGenesis™ Ltd, Oxford, UK, funded by Novartis.
References
- Rogers S, McIntosh RL, Cheung N, et al. The prevalence of retinal vein occlusion: pooled data from population studies from the United States, Europe, Asia, and Australia. Ophthalmology 2010;117:313-9
- Royal College of Ophthalmologists. Interim guidelines for management of retinal vein occlusion. 2010. Available at: http://www.rcophth.ac.uk/core/core_picker/download.asp?id=728&filetitle=Interim+Guidelines+for+Management+of+Retinal+Vein+Occlusion+2010. Accessed August 21, 2013
- Awdeh RM, Elsing SH, Deramo VA, et al. Vision-related quality of life in persons with unilateral branch retinal vein occlusion using the 25-item National Eye Institute Visual Function Questionnaire. Br J Ophthalmol 2010;94:319-23
- Deramo VA, Cox TA, Syed AB, et al. Vision-related quality of life in people with central retinal vein occlusion using the 25-item National Eye Institute Visual Function Questionnaire. Arch Ophthalmol 2003;121:1297-302
- The Branch Vein Occlusion Study Group. Argon laser photocoagulation for macular edema in branch vein occlusion. Am J Ophthalmol 1984;98:271-82
- Scott IU, Ip MS, VanVeldhuisen PC, et al. A randomized trial comparing the efficacy and safety of intravitreal triamcinolone with standard care to treat vision loss associated with macular edema secondary to branch retinal vein occlusion: the Standard Care vs Corticosteroid for Retinal Vein Occlusion (SCORE) study report 6. Arch Ophthalmol 2009;127:1115-28
- Glanville J, Patterson J, McCool R, et al. Efficacy and safety of widely used treatments for macular oedema secondary to retinal vein occlusion: a systematic review. BMC Ophthalmology 2014;14:7
- The Central Vein Occlusion Study Group M report. Evaluation of grid pattern photocoagulation for macular edema in central vein occlusion. Ophthalmology 1995;102:1425-33
- Ip MS, Scott IU, VanVeldhuisen PC, et al. A randomized trial comparing the efficacy and safety of intravitreal triamcinolone with observation to treat vision loss associated with macular edema secondary to central retinal vein occlusion: the Standard Care vs Corticosteroid for Retinal Vein Occlusion (SCORE) study report 5. Arch Ophthalmol 2009;127:1101-14
- National Institute for Health and Care Excellence. TA 283. Ranibizumab for treating visual impairment caused by macular oedema secondary to retinal vein occlusion. May 2013. Available at: http://www.nice.org.uk/nicemedia/live/14169/63851/63851.pdf. Accessed March 18, 2014
- McAllister IL, Gillies ME, Smithies LA, et al. The Central Retinal Vein Bypass Study: a trial of laser-induced chorioretinal venous anastomosis for central retinal vein occlusion. Ophthalmology. 2010;117:954-65
- Lucentis® Summary of Product Characteristics. Availabile at: http://www.medicines.org.uk/emc/medicine/19409/SPC/Lucentis+10+mg+ml+solution+for+injection/. Last updated July 17, 2013.
- Brown DM, Campochiaro PA, Singh RP, et al. Ranibizumab for macular edema following central retinal vein occlusion: six-month primary end point results of a phase III study. Ophthalmology 2010;117:1124-33
- Campochiaro PA, Heier JS, Feiner L, et al. Ranibizumab for macular edema following branch retinal vein occlusion: six-month primary end point results of a phase III study. Ophthalmology 2010;117:1102-12
- Brown DM, Campochiaro PA, Bhisitkul RB, et al. Sustained benefits from ranibizumab for macular edema following branch retinal vein occlusion: 12-month outcomes of a phase III study. Ophthalmology 2011;118:1594-602
- Campochiaro PA, Brown DM, Awh CC, et al. Sustained benefits from ranibizumab for macular edema following central retinal vein occlusion: twelve-month outcomes of a phase III study. Ophthalmology 2011;118:2041-9
- Heier JS, Campochiaro PA, Yau L, et al. Ranibizumab for macular edema due to retinal vein occlusions: long-term follow-up in the HORIZON trial. Ophthalmology 2012;119:802-9
- Gangnon RE, Davis MD, Hubbard LD, et al. A severity scale for diabetic macular edema developed from ETDRS data. Invest Ophthalmol Vis Sci 2008;49:5041-7
- National Institute for Health and Care Excellence. Guide to the methods of technology appraisal. Last updated July 2013. Available at: http://www.nice.org.uk/aboutnice/howwework/devnicetech/guidetothemethodsoftechnologyappraisal.jsp. Accessed August 21, 2013
- Klein R, Klein BE, Linton KL, et al. The Beaver Dam Eye Study: visual acuity. Ophthalmology 1991;98:1310-5
- Christ SL, Lee DJ, Lam BL, et al. Assessment of the effect of visual impairment on mortality through multiple health pathways: structural equation modeling. Invest Ophthalmol Vis Sci 2008;49:3318-23
- Cugati S, Cumming RG, Smith W, et al. Visual impairment, age-related macular degeneration, cataract, and long-term mortality: the Blue Mountains Eye Study. Arch Ophthalmol 2007;125:917-24
- Cugati S, Wang JJ, Knudtson MD, et al. Retinal vein occlusion and vascular mortality: pooled data analysis of 2 population-based cohorts. Ophthalmology. 2007;114:520-4
- National Institute for Health and Care Excellence. TA 229. Dexamethasone intravitreal implant for the treatment of macular oedema secondary to retinal vein occlusion. July 2011. Available at: http://www.nice.org.uk/guidance/TA229. Accessed August 21, 2013
- Brown GC. Vision and quality-of-life. Trans Am Ophthalmol Soc 1999;97:473-511
- Czoski-Murray C, Carlton J, Brazier J, et al. Valuing condition-specific health states using simulation contact lenses. Value Health 2009;12:793-9
- Department of Health. NHS reference costs 2009–10. January 2011. Available at: https://www.gov.uk/government/publications/nhs-reference-costs-2009-2010. Accessed August 21, 2013
- Meads C, Hyde C. What is the cost of blindness? Br J Ophthalmol 2003;87:1201-4
- Curtis L. Unit costs of health & social care 2011. Personal Social Services Research Unit. 2011. Available at: http://www.pssru.ac.uk/archive/pdf/uc/uc2011/uc2011.pdf. Accessed August 21, 2013
- Haller JA, Bandello F, Belfort R Jr, et al. Randomized, sham-controlled trial of dexamethasone intravitreal implant in patients with macular edema due to retinal vein occlusion. Ophthalmology 2010;117:1134-46
- Haller JA, Bandello F, Belfort R Jr, et al. Dexamethasone intravitreal implant in patients with macular edema related to branch or central retinal vein occlusion twelve-month study results. Ophthalmology 2011;118:2453-60
- Loewenstein A, Bandello F, Tufail A, et al. Design and rational of Como, a 12-month masked study that compares the safety and efficacy of Oozurdex® versus Ranibizumab in branch retinal vein occlusion. Proceedings of the 2nd World Congress on Controversies in Ophthalmology, 3–6 March 2011, Barcelona, Spain. Available at: http://www.comtecmed.com/cophy/2011/Uploads/assets/loewenstein.pdf. [Last accessed 12 December 2013]
- Joint Formulary Committee. British National Formulary (online). London: BMJ Group and Pharmaceutical Press. Available at: http://www.medicinescomplete.com. Accessed November 2012
- Schwander B, Gradl B, Zollner Y, et al. Cost-utility analysis of eprosartan compared to enalapril in primary prevention and nitrendipine in secondary prevention in Europe–the HEALTH model. Value Health 2009;12:857-71