

Abstract
Background:
Buprenorphine/naloxone film was developed to improve retention in treatment and reduce public health risks over the tablet formulation for opioid dependence.
Objectives:
To compare patient persistence and resource utilization between formulations for the treatment of opioid dependence.
Methods:
A longitudinal, retrospective cohort analysis was conducted to compare persistence and healthcare costs in a private US insurance claims database. Previously untreated patients, who initiated treatment with buprenorphine/naloxone following the introduction of the film, were classified in two groups according to the initial prescription. Persistence was defined as the proportion of patients continuing treatment for at least 6 months. Resource utilization and related costs were calculated over the 6- and 12-month periods after treatment initiation.
Results:
Film and tablet groups included 2796 and 1510 patients enrolled over 9.76 and 13.76 months on average, respectively, from initiation of treatment. Patient characteristics were similar between groups. Mean prescribed doses were 14.62 and 14.26 mg/day in film and tablet groups. Among patients enrolled for at least 6 months from the initial treatment, persistence rates were 63.78% with film vs 58.13% with tablet. Time to treatment discontinuation was longer in the film group, with a hazard ratio of 0.818 (p = 0.0005, 95% CI = [0.730;0.916]) adjusted for baseline characteristics. Patients treated with film had significantly more outpatient visits (+4%, p = 0.0185) and lower probability to be hospitalized (−17%, p = 0.0158), resulting in lower total healthcare costs over the 12-month period after initiation (−27%, p < 0.0001).
Conclusions:
Patients treated with the film formulation of buprenorphine/naloxone appeared to stay longer on treatment, have a lower probability of hospital admission, and lower health care costs compared to patients treated with the tablet. This study, based on insurance claims data, has the advantage of reflecting real-world practice, but one cannot rule out the existence of bias due to differences in patient or prescriber profiles, despite adjustments made for observed characteristics at treatment initiation.
Background
Opioid drug dependence is a chronic relapsing brain disorder characterized by tolerance, withdrawal, intense craving, and an individual’s inability to stop using opioids even when it is in his or her best interest to do soCitation1. It is a complex health condition that often requires long-term treatment and careCitation2. It includes dependence on prescription pain medications, heroin, and other illicit opioid agonistsCitation3,Citation4. The economic burden associated with untreated drug abuse and drug dependence is substantial; total charges associated with emergency department and hospital inpatient care for opioid-related events were estimated at $9.5 billion in 2008Citation5. Existing medication-assisted treatments (MAT) for opioid dependence in the US are buprenorphine/naloxone and methadone.
Buprenorphine is available in a monoformulation and in combination with naloxoneCitation6. Buprenorphine is a partial mu opioid agonist and naloxone is a full opioid antagonist. Naloxone has negligible bioavailability at the oral and sublingual routes, and was added to deter diversion and abuse by injection and snortingCitation7. When taken parenterally, naloxone becomes 100% bioavailable, blocks the euphoric effects of opioids including buprenorphine, and precipitates withdrawalCitation8. The buprenorphine/naloxone combination was launched in the US in 2002 in the form of sublingual tablets (Suboxone Sublingual Tablets, no longer available) and in 2010 in the form of sublingual film (Suboxone Sublingual). In 2013 generic forms of buprenorphine/naloxone tablets were approved by the FDA.
The sublingual film formulation was intended to help safeguard public health through reduction in accidental pediatric exposure by using unit dose child-resistant packaging, and to reduce diversion and abuse through the use of serialization of packaging and a formulation resistant to crushing and snorting. In contrast to the tablet, the film has a muco-adhesive quality that is expected to reduce chances of prematurely swallowing the medication before the absorption has completed in the sublingual compartment. In addition, the film formulation was designed to dissolve faster, to improve the taste, and to be easier to carry during travel. Those changes are expected to be associated with better persistence and compliance, although no real-world study has shown this yet.
Improving persistence in treatment among patients suffering from opioid-dependence is important to increase the chance of recovery and limit the economic burden of the disorderCitation9. Weiss et al.Citation10 found relapse rates greater than 90% after limiting treatment to 4 and 12 weeks with MAT. Furthermore, Cornish et al.Citation11 demonstrated that mortality risk is 9-times higher in the first 3 months of stopping treatment, and that MAT has an 85% chance of decreasing mortality among opiate dependent patients if the treatment duration approaches or exceeds 1 year. An economic model by Schackman et al.Citation12 suggested that continuing treatment with buprenorphine/naloxone beyond 6 months was cost-effective in the US compared with no treatment at a threshold of $100,000/QALY depending on assumptions about quality-of-life weights. However, many patients discontinue treatment prematurelyCitation13.
Previous studies investigated the cost of treating opioid dependence. MAT was demonstrated to be associated with a reduction in the number of admissions for overdose, rehabilitation, and inpatient care, opioid-related or not, and a reduction of 29% of total healthcare costs compared to non-pharmacological treatment despite additional pharmaceutical costsCitation14. In addition, healthcare costs associated in patients treated with methadone were found to be significantly higher than those in patients treated with buprenorphine (with or without naloxone) over 6 months after the treatment initiationCitation15. The study presented here focussed on the two formulations of buprenorphine and naloxone combination.
The aim of this study, based on a private health insurance claims database, was to compare persistence in treatment, healthcare resource utilization, and total healthcare costs between patients treated with the buprenorphine/naloxone sublingual film formulation and patients treated with the buprenorphine/naloxone sublingual tablet formulation.
Methods
Data source
A longitudinal retrospective cohort analysis was conducted using the Invision DataMart databaseCitation16, which contains information on patients, pharmacy claims, medical claims, and hospitalizations representing more than 30 million covered managed care lives from several of the largest commercial health insurance plans in the US.
The data were obtained for ∼56 months before and 27 months after the launch of the film formulation of buprenorphine/naloxone (from January 1, 2006 to November 30, 2012). Data include diagnoses, coded using the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM)Citation17 for all inpatient and outpatient claims. Dates of service and costs are available for all patient claims.
Inclusion and exclusion criteria
Patients having evidence of treatment with the buprenorphine/naloxone sublingual film (launched September 1, 2010) or tablet formulation between January 1, 2006 and November 30, 2012, were identified. The first recorded pharmacy dispensing claim for buprenorphine/naloxone is termed the ‘index event’ for this analysis. As depicted in and , the study utilized a look-back period of 365 days to establish whether there was no utilization of buprenorphine/naloxone prior to the ‘index date’, and no utilization of buprenorphine monotherapy between 365 days and 14 days before the ‘index date’. This was done to ensure that patients who received buprenorphine monotherapy during the induction phase were included. Patients with at least 12 months of continuous enrolment prior to ‘index date’ and at least one renewal of buprenorphine/naloxone prescription between 30 days and 75 days after the index date (in order to exclude short term users) were included in the analysis. If a patient had more than one treatment episode matching the criteria above during the observation period (i.e. two treatment episodes with an interval of at least 12 months without buprenorphine), only the first treatment episode was taken into account. A sensitivity analysis without the requirement for a prescription renewal between 30–75 days was also performed, for the comparison of persistence between formulations.
Figure 1. Cohort selection. BUP/NAL, buprenorphine/naloxone.
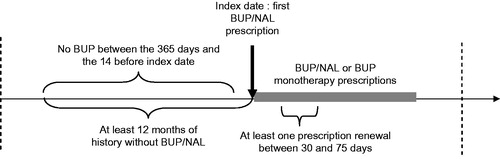
Figure 2. Population identification: patients in the database.
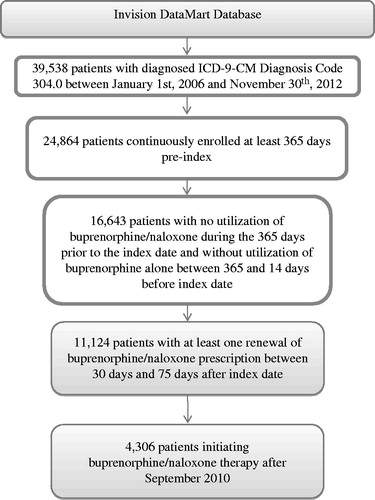
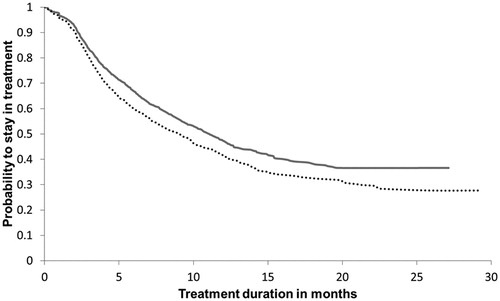
Figure 3. Kaplan Meier Curve: Time to discontinuation. BUP/NAL, buprenorphine/naloxone.
Patients initiating buprenorphine/naloxone therapy with the film formulation were compared to patients initiating therapy with the tablet formulation after the launch of the film (after September 2010). Comparisons between the two groups were done over the same period to avoid biases related to the evolution of clinical practice or of the healthcare costs over time.
Definition of outcomes
The outcomes of interest were the time to discontinuation of buprenorphine/naloxone, persistence rates, switch rates, average daily doses, resource utilization, and healthcare costs. Discontinuation was defined as a gap of at least 31 days without a claim for buprenorphine/naloxone or buprenorphine following the date when the last package claimed was expected to be consumed (determined according to claim date and duration of prescription). Persistence rates were defined as the proportions of patients who had not discontinued treatment after 6 and 12 months.
Switch was defined as a change in formulation (e.g. tablet to film, film to tablet, buprenorphine/naloxone to buprenorphine monotherapy) with a gap not exceeding 30 days between depletion of the day’s supply for the previous claim and the date of the following claim. This is reported for two reasons: (1) because switching from film to tablet would suggest that patients are dissatisfied with the film; and (2) because high switch rates would affect the interpretation of any difference in other outcomes between groups defined according to initially prescribed formulation. A switch to a different formulation was not considered as a case of discontinuation.
Average daily doses were calculated as the quantity of product prescribed (number of films or tablets) multiplied by the strength of the product and divided by the number of days for which buprenorphine/naloxone was prescribed.
The costs available in the database were estimations from the perspective of insurance plans based on different methods for all major types of healthcare services that account for the quantity of services provided, the relative resource costs involved in providing the service, and the nature of the service.
Inpatient facility costs were based on an estimated per diem cost using aggregated diagnostic and service category, the presence or not of major surgery, length of stay, and single or same day stays were treated differently than stays of 2 or more days. The costs of facility outpatients were estimated as a percent of the submitted charges. Professional service pricing was standardized at ∼130% overall of Medicare Fee for ServiceCitation18 for common services. Standard pricing for drugs and pharmacy services was based on pricing from First DatabankCitation19, adjusted by therapeutic category and generic indicator to allow for the typical difference between First Databank pricing and the allowed amounts observed in the pharmacy claims data. In this way, relative pricing within a therapeutic category and generic indicator was determined by First Databank information, while general pricing levels by therapeutic category and generic indicator were determined by observed payments. To create a standardized cost, the resulting average payment schedule was applied to each pharmacy service—based on the NDC code listed and the metric quantity for the prescription.
Total healthcare costs were calculated over periods of 12 months before index date, 6 months after index date, and 12 months after index date, including all pharmacy, inpatient, and outpatient claims. The analysis of healthcare costs was based on complete cases. For example, patients who were followed for less than 12 months from index date were excluded for the analysis of healthcare costs over 12 months. In addition, the observation period was partitioned in treatment phases: before treatment (up to 2 weeks before initiation of treatment with buprenorphine/naloxone), treatment initiation (from 2 weeks before to 2 weeks after index date), on treatment (from 2 weeks after index date to 2 weeks before discontinuation), treatment discontinuation (from 2 weeks before to 2 weeks after date of discontinuation), after treatment (from 2 weeks after discontinuation to 2 weeks before re-initiation), and treatment re-initiation (from 2 weeks before to 2 weeks after date of treatment re-initiation). Average monthly costs were calculated within each period. Periods shorter than 28 days were not considered.
Statistical analyses
The time to discontinuation was analyzed using the Kaplan Meier method, and a Cox model was used to estimate the hazard ratio associated with each buprenorphine/naloxone formulation, adjusting for patient characteristics at baseline and daily dose entered as a time-dependent variable.
The numbers of pharmacy claims and outpatient visits during the 12-month periods before and after treatment initiation were analyzed using Poisson regression with adjustment for patient characteristics. To determine whether there was a significant effect of treatment formulation on resource utilization, we also controlled resource utilization before treatment initiation to analyze resource utilization in the period after index date. Similarly, the probability to have at least one hospitalization and the probability to have at least one emergency room (ER) visit was analyzed using a logistic regression. Generalized linear models were used to estimate the effect of treatment formulation on costs by resource category, controlling for patient characteristics and costs before treatment initiation (for the analysis of costs after treatment initiation). For emergency room visits and hospitalization, adjusted average costs per admission were estimated and then multiplied by the probability to have at least one. Repeated-measures generalized linear models with a normal distribution and a log-link function were used to analyze the impact of treatment formulation on total monthly costs within each treatment phase, adjusting on confounding factors. The choice of the distribution was based on quality of fit, as assessed by the Root Mean Square Error (RMSE) criterion.
Potential confounding factors considered for adjustments in regression analyses were gender, age, type of health insurance plan, presence of diagnosis of mental disorder in the 12 months before index date, comorbidities (as listed in ), daily dose at index date, and healthcare costs or resource utilization over 12 months before index date when the analyzed period is after treatment initiation. All statistical tests were two-sided and set at the 5% level of significance. The chi-square independence test or Fischer’s exact test were used to test for associations between categorical variables at index date and treatment group and the Student’s t-test was applied for an association between a continuous variable and treatment group. All statistics were computed using SAS 9.3Citation20.
Table 1. ICD9-CM codes used for comorbidities.
Results
A total of 4306 subjects were included in the analysis, of which 2796 (64.93%) patients initiated buprenorphine/naloxone therapy with film formulation and 1510 (35.07%) patients initiated buprenorphine/naloxone therapy with tablet formulation after September 2010. The proportion of short-term users was very similar: 33.97% in the film group vs 33.37% in the tablet group (p = 0.49). The patients were followed on average for 9.76 and 13.76 months, respectively. The average duration of follow-up was lower in the film group because the uptake of the film was relatively low in the first months of the study period. The profiles of these patients are shown in .
Table 2. Patient characteristics at index date, by formulation.
Patient characteristics
The proportion of females (35.40%) was comparable between the two treatment groups. Patients were slightly younger in the film group (34.34 vs 35.65 years) and the distribution by geographical area was slightly different between groups (patients on film more likely to live in the South). The distribution of patients by the type of health insurance plan was comparable between groups. The majority of the patients had a point of service insurance plan (74.18%).
The proportion of patients with a diagnosis of comorbidities in the 12 months before index date is also described in . Drug abuse or dependence was reported in a majority of patients (76.47%), with comparable proportions between the two treatment groups. The second most frequently observed diagnosis was mental disorder (except drug use), with a lower proportion among patients treated with film compared to tablet (61.80% vs 66.89%; p = 0.001). In addition, soft tissues infections were reported in 8.06% of patients, with comparable percentages between groups.
Previous prescriptions for opioid-based medications and pain diagnoses
Presence of opioid prescription and pain diagnosis are reported in . Most of the patients had at least one opioid prescription during the year before index date: 66.38% of the patients treated by film and 69.14% of the patients treated by tablet. A diagnosis of chronic pain was found in 12.54% of patients over the 12 months before index date, and a diagnosis of acute pain in 5.78% of patients, without significant difference between groups.
Treatment characteristics
Co-payments and daily doses for the index date prescriptions are displayed in . The percentage of co-payment for index claim was not statistically different between the two groups, with an average of 15.61% in the tablet group and 15.19% in the film group.
The patients initially receiving the tablet formulation had a slightly lower dose for their first prescription than patients who initiated with the film formulation. Furthermore, 27.86% of the patients treated with film received a daily dose of up to 8 mg per day vs 33.11% for patients treated with tablet; and 65.20% received a dose of 12 mg or more per day with film vs 59.34% with tablet (p < 0.0001). The difference in daily dose decreased over time. After 5 months, the trend was reversed: the average daily dose with film was lower than the average daily dose with tablet.
Table 3. Adjusted healthcare costs and resource utilization in the 12 months before and after index date.
Persistence, discontinuation, and switch
There were 1134 cases of discontinuation with film formulation and 821 with tablet formulation. Persistence at 6 months was significantly higher for the film group than for the tablet group (63.78% vs 58.13%; p = 0.002). Based on Kaplan-Meier analysis shown in , the estimated probability of discontinuing treatment before 12 months was 52.86% for patients treated with film, compared to ∼58.66% for patients treated with tablet. In the tablet group, 251 (16.62%) patients switched to film. Of the patients on film, 102 (3.65%) switched to tablet.
After adjustment on age, gender, region, health plan category, co-payment proportion, and dose, the time to treatment discontinuation was significantly longer in the film group, as shown by a hazard ratio of 0.818 (p = 0.0005). Other variables with a significant effect on the time to discontinuation were age and the daily dose in the previous month. In the sensitivity analysis, including all patients with or without buprenorphine/naloxone renewal prescription between 30–75 days after initial prescription, the hazard ratio was estimated at 0.819 (p < 0.0001).
Resource use and healthcare costs
The healthcare costs and resource utilization are described by formulation group in . Adjusted mean numbers of pharmacy claims were not significantly different between the film and tablet formulations during both periods of 12 months before and after treatment initiation. The probabilities of having at least one inpatient claim were lower in the film group than in the tablet group before treatment initiation and after treatment initiation, controlling for the presence of inpatient claim before treatment initiation. The probability to have at least one ER visit was similar in the two groups before and after treatment initiation. After adjustment on patient characteristics, the average number of outpatient visits was similar before treatment initiation. The number of outpatient visits was found to be 4% higher over 12 months following treatment initiation for patients in the film group (p = 0.0185), controlling for patient characteristics (age, gender, presence of diagnosis of mental disorder during the 12 months before index date, presence of diagnosis of chronic pain during the 12 months before index date, type of health insurance plan, outpatient visits over the 12 months before index date, and daily dose at index date).
Table 4. Generalized linear models* on total healthcare costs in the 6 and 12 months post-index periods.
For each category of resources, the adjusted average costs were lower in the film group than in the tablet group, during the periods of 12 months before index date and after index date, controlling for costs before index date. The generalized linear model on the total healthcare costs is presented in . The effect of the treatment formulation on total healthcare costs over both 6 and 12 months after index date was statistically significant. Adjusted total healthcare costs were lower in the film group by $2860 (p = 0.0008) over 12 months before index date, and by $5422 (p < 0.0001) over 12 months after index date. Being treated with film rather than with tablet was associated with a reduction in total healthcare costs by 24% (95% CI = 16–32%) over 6 months and 27% (95% CI = 16–37%) over 12 months, after adjustment on baseline characteristics including costs before treatment initiation.
Table 5. Generalized linear model* on total monthly costs, by treatment phase.
presents the results of the regression analysis on monthly costs by treatment phase. The model estimated the ratio of monthly costs for each treatment phase for the two groups, relative to the monthly total healthcare costs during the period before treatment in patients initiating treatment with the tablet formulation. The monthly costs for the reference patient (i.e., fictitious patient in tablet group, male, aged 18 years, living in the Northeast region, with preferred provider organization plan, and no diagnosis of mental disorder before treatment initiation) were $979. Healthcare costs were highest in the month around initiation of buprenorphine/naloxone, in the two groups. In addition, monthly costs during treatment were significantly lower than during the discontinuation (p < 0.0001) and the re-initiation phases (p = 0.0.279), in the film group.
Discussion
This study provides evidence on persistence in treatment, resource utilization, and healthcare costs based on a large sample of 4306 privately insured patients treated with buprenorphine/naloxone. The two groups of patients treated with the film or tablet formulation appeared to have comparable socio-demographic characteristics and comorbidities at treatment initiation. The film formulation was found to be associated with significantly longer persistence in treatment. The discontinuation hazard was reduced by 18% among patients who received the film formulation, after adjustment on observed patient characteristics at baseline (p = 0.0005). In addition, the film formulation was found to be associated with a reduction in total healthcare costs over 6 and 12 months from treatment initiation, by 24% and 27% (p < 0.0001; p < 0.0001) respectively. Patients receiving the film formulation had a slightly higher number of outpatient visits, but a lower probability to have one hospitalization or more. Estimated monthly healthcare costs were lower during the period in treatment, compared to discontinuation and re-initiation period when treated with the film. Also, the improvement in persistence is likely to be a factor contributing to the reduction in healthcare costs among patients receiving the film formulation.
In a previous study based on administrative claims, the mean persistence with buprenorphine/naloxone was estimated to be 3.5 months and the median length of therapy was 1 month. The definition of discontinuation was the same, i.e. absence of refill for at least 30 days following depletion of the day’s supply for a buprenorphine/naloxone claim. The reason for the substantially higher persistence in this study lies in the selection of patients, as patients without a second prescription of buprenorphine/naloxone were excluded in order to focus on patients who entered the treatment maintenance phase.
Using another administrative claims database, Baser et al.Citation14 estimated total healthcare costs among patients treated with buprenorphine (with or without naloxone) in 2005 at $10,710 over 6 months after index date. Previously, a study based on Veterans Health Administration data estimated healthcare costs over 6 months after initiation of buprenorphine at $11,597Citation20. Average adjusted total healthcare costs over 6 months after index date were estimated to be $10,405 for the film group and $13,751 for the tablet group, and are, thus, comparable to previous estimates.
Limitations
Some advantages of working with data from insurance databases are that they provide access to large numbers of patients and represent treatment length and economic burden in real practice. However, there are also several limitations associated with the use of such databases. One of these limitations was that, while access to pharmacy claims was available, information was not available on whether medications were taken as instructed. In a previous study reporting persistence on buprenorphine treatment, Strain et al.Citation21 defined discontinuation as 1 day without treatment. This level of precision is not possible in analyses using claims data.
In addition, the reporting of ICD-9 codes associated with claims is incomplete in the databases, as physicians may only report the top few codes that would be associated with reimbursement. This has likely led to an under-estimation of the prevalence of comorbidities. However, the extent of under-reporting should be similar in both groups, and estimated prevalences of comorbidities were generally comparable between groups, so this is unlikely to result in significant bias in the comparison between patients receiving the film and tablet formulations.
As mentioned above, the costs available were not real costs but estimations using standard pricing algorithms applied to the claims data. These algorithms were designed to create standard prices that reflect allowed payments across all provider services. In this way, comparisons across patients, data sources, and geographic areas can be made in a consistent manner—as if the data were derived from a single source using a single approach for classifying and pricing services.
There were some significant differences between groups at baseline, although most characteristics were similar. The total healthcare costs at baseline were lower for patients in the film group than for patients in the tablet group. Regression analysis was used to adjust estimates of the effect of treatment formulation on persistence and healthcare costs for differences existing at baseline. However, the possibility of residual bias due to unobserved confounding factors cannot be ruled out. One important variable to consider is the cause of dependence. Treatment outcomes are expected to differ between patients who became addicted following use of opioids in a medical context and patients who consume opioid-based medications or heroin for recreational purpose. Variables such as the presence of a chronic pain diagnosis, pharmacy claims for opioid-based medication or diagnoses of mental disorder were used as adjustment factors because they were thought to be related to the cause of dependence. There was, however, no way to identify the cause of dependence on the opioids with any certainty. It was impossible to determine whether claims for opioid-based medications before the index date were related to recreational use or medical use.
In order to determine whether the difference in persistence between the film and tablet treated groups could be due to unobserved differences in patient or physician profiles, another type of comparison reported elsewhere was performedCitation22. This other analysis compared patients treated with the film to patients who received the tablet formulation prior to the approval of the film formulation in September 2010. Different types of bias are possible in a before-and-after comparison, as clinical practices may evolve over time. However, patient and physician profiles should be more similar between the film and tablet groups. The hazard ratio for discontinuation between film and tablet was then estimated at 0.81, i.e., with the actual hazard ratio result at 0.82, which suggests that the estimated improvement in persistence is robust.
Conclusion
Patients treated with the film formulation of buprenorphine/naloxone appeared to stay longer on treatment, have lower probability to be hospitalized, and lower healthcare costs compared to patients who received the tablet formulation. As a retrospective study, it cannot be ascertained whether there is a causal relationship between treatment formulation and the studied outcomes; however, the relationship between formulation and persistence was analyzed in multiple ways, and the results were consistent with the hypothesis that the film formulation led to an improved persistence in treatment. In addition, healthcare costs were found to be higher after treatment discontinuation than during treatment, likely due to the additional expenses related to relapse and the re-initiation of treatment, which contributed to higher total costs with tablet formulation treatment.
Transparency
Declaration of funding
The study was sponsored by Reckitt-Benckiser.
Declaration of financial/other relationships
Reckitt-Benckiser has financial relations with ZRx Outcomes Research, which has financial relations with Creativ-Ceutical.
Acknowledgments
No assistance in the preparation of this article is to be declared.
Notes
*Reckitt Benckiser Pharmaceuticals, Inc., Package Insert, Richmond, VA.
References
- World Health Organisation. Guidelines for the psychosocially assisted pharmacological treatment of opioid dependence. Geneva, Switzerland, 2009, http://www.who.int/substance_abuse/publications/opioid_dependence_guidelines.pdf. Accessed 28 May 2014
- Nicholls L, Bragaw L, Ruetsch C. Opioid dependence treatment and guidelines. J Manag Care Pharm 2010;16(1 Suppl B):S14-21. http://www.amcp.org/data/jmcp/S14-S21.pdf. Accessed 28 May 2014
- Stoops WW, Hatton KW, Lofwall MR, et al. Intravenous oxycodone, hydrocodone, and morphine in recreational opioid users: abuse potential and relative potencies. Psychopharmacology (Berl) 2010;212:193-203
- Ling W, Mooney L, Hillhouse M. Prescription opioid abuse, pain and addiction: clinical issues and implications. Drug Alcohol Rev 2011;30:300-5
- Chandwani HS, Strassels SA, Rascati KL, et al. Estimates of charges associated with emergency department and hospital inpatient care for opioid abuse-related events. J Pain Palliat Care Pharmacother 2013;27:206-13
- Clark HW. Office-based practice and opioid-use disorders. N Engl J Med 2003;349:928-30
- Otiashvili D, Piralishvili G, Sikharulidze Z, et al. Methadone and buprenorphine-naloxone are effective in reducing illicit buprenorphine and other opioid use, and reducing HIV risk behavior-Outcomes of a randomized trial. Drug Alcohol Depend 2013;133:376-82
- Yokell MA, Zaller ND, Green TC, et al. Buprenorphine and buprenorphine/naloxone diversion, misuse, and illicit use: an international review. Curr Drug Abuse Rev 2011;4:28-41
- McLellan AT, Lewis DC, O’Brien CP, et al. Drug dependence, a chronic medical illness: implications for treatment, insurance, and outcomes evaluation. JAMA 2000;284:1689-95
- Weiss RD, Potter JS, Fiellin DA, et al. Adjunctive counseling during brief and extended buprenorphine-naloxone treatment for prescription opioid dependence: a 2-phase randomized controlled trial. Arch Gen Psychiatry 2011;68:1238-46
- Cornish R, Macleod J, Strang J, et al. Risk of death during and after opiate substitution treatment in primary care: prospective observational study in UK General Practice Research Database. BMJ 2010;341:c5475
- Schackman BR, Leff JA, Polsky D, et al. Cost-effectiveness of long-term outpatient buprenorphine-naloxone treatment for opioid dependence in primary care. J Gen Intern Med 2012;27:669-76
- Kaur AD, McQueen A, Jan S. Opioid drug utilization and cost outcomes associated with the use of buprenorphine-naloxone in patients with a history of prescription opioid use. J Manag Care Pharm 2008;14:186-94
- Baser O, Chalk M, Fiellin DA, et al. Cost and utilization outcomes of opioid-dependence treatments. Am J Manag Care 2011;17(8 Suppl):S235-48
- Barnett PG. Comparison of costs and utilization among buprenorphine and methadone patients. Stanford University, CA: Veterans Affairs Health Economics Resource Center and Department of Health Research and Policy, 2013
- Optum insight, clinformatics Data Mart. http://www.optuminsight.com/life-sciences/solutions/value-strategy/marketing-analytics/clinformatics-data-mart/~/media/Ingenix/Life_Sciences/Documents/OptumInsightLifeSciencesClinformaticsDataMart_old.pdf. Accessed 24 May 2014
- The National Center for Health Statistics (NCHS) and the Centers for Medicare and Medicaid Services. International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM). http://www.cdc.gov/nchs/icd/icd9cm.htm. Accessed 28 May 2014
- Medicare Fee-for-service. http://www.cms.gov/Medicare/Coding/ICD10/Medicare-Fee-for-Service-Provider-Resources.html. Accessed 28 May 2014
- First Databank. http://www.fdbhealth.com/. Accessed 28 May 2014
- SAS Institute Inc. SAS V9.3. Cary, NC: SAS Institute Inc, http://support.sas.com/software/93/. Accessed 28 May 2014
- Strain EC, Stitzer ML, Liebson IA, et al. Buprenorphine versus methadone in the treatment of opioid-dependent cocaine users. Psychopharmacology (Berl) 1994;116:401-6
- Zah V, Clay E, Aballea S, et al. Patient persistence with Buprenorphine/Naloxone Film and tablet formulations in the treatment of opioid dependence in the United States: results from a privately insured retrospective database, Association for Medical Education and Research in Substance Abuse, 36th Annual National Conference, Bethesda, Maryland, 2012