

Abstract
Objective:
Venous thromboembolism (VTE) (deep vein thrombosis [DVT] and pulmonary embolism [(PE]) represents a substantial economic burden to the healthcare system. Using data from the randomized EINSTEIN DVT and PE trials, this North American sub-group analysis investigated the potential of rivaroxaban to reduce the length of initial hospitalization in patients with acute symptomatic DVT or PE.
Methods:
A post-hoc analysis of hospitalization and length-of-stay (LOS) data was conducted in the North American sub-set of patients from the randomized, open-label EINSTEIN trial program. Patients received either rivaroxaban (15 mg twice daily for 3 weeks followed by 20 mg once daily; n = 405) or dose-adjusted subcutaneous enoxaparin overlapping with (guideline-recommended ‘bridging’ therapy) and followed by a vitamin K antagonist (VKA) (international normalized ratio = 2.0–3.0; n = 401). The open-label study design allowed for the comparison of LOS between treatment arms under conditions reflecting normal clinical practice. LOS was evaluated using investigator records of dates of admission and discharge. Analyses were carried out in the intention-to-treat population using parametric tests. Costs were applied to the LOS based on weighted mean cost per day for DVT and PE diagnoses obtained from the Healthcare Cost and Utilization Project dataset.
Results:
Of 382 patients hospitalized, 321 (84%), had acute symptomatic PE; few DVT patients required hospitalization. Similar rates of VTE patients were hospitalized in the rivaroxaban and enoxaparin/VKA treatment groups, 189/405 (47%) and 193/401 (48%), respectively. In hospitalized VTE patients, rivaroxaban treatment produced a 1.6-day mean reduction in LOS (median = 1 day) compared with enoxaparin/VKA (mean = 4.5 vs 6.1; median = 3 vs 4), translating to total costs that were $3419 lower in rivaroxaban-treated patients.
Conclusion:
In hospitalized North American patients with VTE, treatment with rivaroxaban produced a statistically significant reduction in LOS. When treating DVT and PE patients, clinicians should consider newer anti-coagulants with less complex treatment regimens.
Introduction
Venous thromboembolism (VTE), comprising both deep vein thrombosis (DVT) and pulmonary embolism (PE), remains one of the most common and preventable complications of hospitalizationCitation1. The consequences of VTE may be serious, accounting for 600,000 annual US hospitalizationsCitation2 and nearly 300,000 US deaths due to PECitation3. The complications that may arise from inadequate treatment can have serious economic consequences, which often manifest as increased length of stay and re-hospitalizationCitation3. Traditional therapy for patients presenting with acute symptomatic VTE has consisted of an initial course of low-molecular-weight heparin (LMWH), such as enoxaparin or the synthetic pentasaccharide factor Xa inhibitor fondaparinux, usually administered in the hospital, followed by a vitamin K antagonist (VKA), such as warfarin, for post-discharge useCitation4,Citation5.
A variety of factors may affect hospital discharge for patients with VTE. Because warfarin requires several days to become therapeutic, ‘bridging’ therapy—transition from the injectable agents to the oral anticoagulant—is generally administered. During this period, patients receive both agents, and those with PE often remain in the hospital solely for monitoring. Also, while LMWH has been shown to substantially reduce length of stay (LOS) compared with unfractionated heparinCitation6,Citation7, delays in discharge for patients receiving this therapy are common, for a variety of reasons ranging from hospital practiceCitation8 to physician judgmentCitation9. Premature discharge of at-risk patients has also been notedCitation10.
Rivaroxaban, a specific, direct, oral factor Xa inhibitor, is approved in the US, Canada, and Europe for reducing the risk of recurrence of DVT and of PE. In the EINSTEIN clinical program, rivaroxaban was shown to be as effective as standard anticoagulant therapy for the prevention and treatment of DVT and PE without the need for laboratory monitoringCitation11. The EINSTEIN studies showed similar efficacy and a lower incidence of major bleeding with rivaroxaban, with reductions seen mainly in fatal and non-fatal critical-site bleeding, such as intracranial and retroperitoneal bleeding, and in patients who were elderly or frail, had impaired renal function, or had cancerCitation12.
A subsequent analysis investigated the potential of rivaroxaban to reduce the length of initial hospitalization in VTE patients enrolled in the EINTEIN DVT and PE trialsCitation13. LOS was evaluated from investigator records of dates of hospital admission and discharge. For regional comparisons, hospitalization data were drawn from participating study centers in Western Europe, Eastern Europe, Australia and New Zealand, South America, North America, Asia, Israel, and South Africa. In the EINSTEIN DVT trial, 1781 of 3449 (52%) patients were hospitalized for the qualifying event. Median LOS was significantly shorter for rivaroxaban-treated patients compared with those treated with enoxaparin/VKA (5.0 vs 8.0 days; p < 0.0001). In the EINSTEIN PE trial, 4328 of 4832 (90%) patients were hospitalized. Median LOS was significantly shorter in patients receiving rivaroxaban than in patients receiving enoxaparin/VKA (6.0 vs 7.0 days; p < 0.0001).
Using data from the EINSTEIN DVT and PE studies, this post-hoc analysis investigated the potential of rivaroxaban to reduce the length of initial hospitalization in the North American (US and Canada) sub-set of patients presenting with acute symptomatic DVT or PE in the EINSTEIN DVT and EINSTEIN PE trials.
Methods
Treatment and study design
Full details of the EINSTEIN DVT and PE studies have been publishedCitation14,Citation15. Patients were randomized to receive open-label rivaroxaban 15 mg twice daily for the first 3 weeks, then 20 mg daily or enoxaparin at a dose of 1.0 mg/kg of body weight twice daily followed by warfarin or acenocoumarol started 48 h after randomization. Prior to randomization, 84% of all VTE patients (86% in the rivaroxaban arm and 83% in the enoxaparin/VKA arm) received parenteral LMWH pre-treatment. Enoxaparin was discontinued when the INR was ≥2.0 for 2 consecutive days and the patient had received at least 5 days of enoxaparin treatmentCitation14,Citation15.
This was an open-label study in which attending physicians made treatment decisions under conditions reflecting normal clinical practice. Hospital LOS was evaluated from investigator records of dates of admission and discharge; an LOS of 0 indicated that a patient was not hospitalizedCitation13.
Statistical and cost analyses
Analyses were performed in the intention-to-treat population. Hospital LOS data were reported using descriptive statistics. 2009 mean costs per VTE hospital day were obtained from the Healthcare Cost and Utilization Project (HCUP), sponsored by the Agency for Healthcare Research and Quality (AHRQ). The individual DVT and PE costs per day were pooled based on the distribution of DVT and PE patients in the final hospitalized dataset.
Results
Patients
Overall, 812 participants in the North American cohort of the EINSTEIN DVT and PE studies were treated for DVT (n = 326) or PE (n = 486). Of this group, 382 patients were hospitalized, of whom 189 were treated with rivaroxaban and 193 with enoxaparin/VKA (). Patient characteristics such as age, weight, and creatinine clearance were similar between treatment groups at baseline ().
Figure 1. Hospitalized DVT and PE patients in North American EINSTEIN trial.
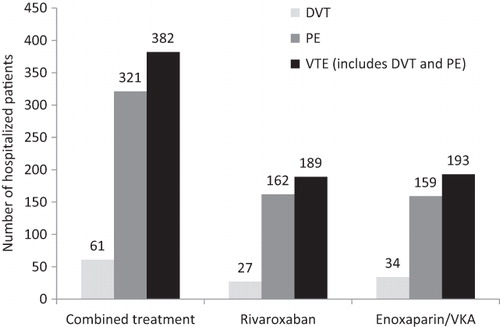
Table 1. Demographic characteristics of North American patients enrolled in the EINSTEIN DVT and PE studies.
Hospitalized patients
The majority of hospitalized patients had PE (n = 321; 84%). Only 61 (16%) DVT patients were hospitalized. In the individual studies, there were no significant differences between treatment groups in the numbers or proportions of hospitalized patients; i.e., there were 27/162 (16.7%) vs 34/161 (21.1%) hospitalized patients in the rivaroxaban and enoxaparin/VKA treatment arms of the DVT trial, respectively, and 162/243 (66.7%) vs 159/240 (66.3%) in the rivaroxaban and enoxaparin-VKA treatment arms of the PE trial, respectively ().
LOS of hospitalized VTE patients
Hospitalized VTE patients receiving rivaroxaban (n = 189) had a 1.6-day mean reduction in LOS compared with patients treated with enoxaparin/VKA (n = 193; mean = 4.5 vs 6.1; median = 3 vs 4) (). This was primarily driven by the 1.7-day mean reduction in hospital LOS for PE patients treated with rivaroxaban (n = 162) vs enoxaparin/VKA (n = 159; mean = 4.5 vs 6.2; median = 3 vs 4; p = 0.0002). However, there was not a significant difference in LOS in the hospitalized DVT patients, mainly because of the low numbers of patients (rivaroxaban, n = 27; enoxaparin/VKA, n = 34) (mean = 4.7 vs 5.4; p = NS).
Table 2. Length of hospital stay for all patients with VTE in the EINSTEIN DVT and EINSTEIN PE trials (n = 382).
Cost savings associated with reduced LOS
Mean costs per day were $1842 for PE patients and $295 for DVT patients (). The pooled mean cost per VTE day was $2137. Thus, the reduction in LOS in all VTE patients treated with rivaroxaban (4.5 vs 6.1; a difference of 1.6) translated to a total mean cost savings of $3419 per patient.
Table 3. Pooled mean cost per VTE day.
Discussion
Medical patients account for more than half of all hospital-acquired VTE eventsCitation16. The direct (medical care and hospitalization) and indirect (e.g., reduced productivity, need for assistance with activities of daily living as the result of diminished mobility) costs related to treatment and re-treatment of VTE in these patients are substantial for both payers and patientsCitation17–21. As shown in the EINSTEIN studies, North America already has the shortest LOS compared with the other regions analyzed, and in an effort to further reduce costs, many low-risk patients with both DVT and PE are frequently treated on an outpatient basisCitation22.
In this sub-analysis from the EINSTEIN studies, PE patients, who comprised 84% of hospitalized VTE cohort, experienced a mean LOS difference of 1.7 and a median LOS of 3 days with rivaroxaban vs 4 days with a standard enoxaparin/VKA regimen. Cost savings from this 1-day reduction in LOS resulted in substantial cost offsets (>$2000 median savings per patient) using rivaroxaban compared with warfarin. It should be noted that this substantial difference in LOS occurred within the conservative clinical trial setting, but the LOS data presented here are comparable to previous studies. In a cohort of 29,275 commercial-payer patients, Lin et al.Citation23 reported a mean LOS of 5.5 days for recurrent VTE within 30 days of the initial event and 8.4 days for those recurring within 12 months. Moreover, the data were obtained before rivaroxaban was widely used and its efficacy fully understood. It is, therefore, possible that patients receiving rivaroxaban may have been discharged later than necessary as a result of clinicians’ lack of familiarity with this newer agent at the time of this study. If this was the case, greater awareness of the efficacy and safety of rivaroxaban in the treatment of DVT and PE may allay clinicians’ concerns and result in more patients being discharged earlier, further reducing costs of care.
Our study evaluated only LOS, but other factors, such as the need for bridging therapy and for regular patient monitoring at anticoagulation clinics, must be considered in any comprehensive cost-effectiveness evaluation. Consideration of costs for bridging and anti-coagulation monitoring would have further tipped the balance in favor of rivaroxaban, as both are required with LMWH/VKA therapy, and neither is required with rivaroxaban.
Re-hospitalization costs must also be considered. For those who are re-hospitalized for a VTE event, costs can be considerably greater than those related to the initial event due to significantly longer hospitalization timesCitation23. Re-hospitalization rates may depend to a considerable extent on patient compliance with medication regimens post-discharge. The problems inherent in warfarin management (e.g., requirements for bridging therapy and frequent anticoagulation monitoring and numerous drug–drug and drug–food interactions) may discourage compliance. The convenience of the newer anti-coagulants, including rivaroxaban, can improve compliance and, thereby, help reduce repeat events and re-hospitalization rates.
Limitations
Canadian centers (included in this study) tend to hospitalize few patients for DVT, thus lowering the percentage of DVT patients in our cohort. Therefore, our conclusions were based mainly on the patients with PE. Secondly, cost savings in our study were estimated based on average cost per day rather than actual cost reductions due to shorter LOS. Thus, savings could have been over-estimated if VTE treatment costs were front-loaded during the hospital stay. LOS may also reflect causes other than the therapeutic regimen, such as lengthy diagnostic procedures or late discharge proceduresCitation8.
The cost savings associated with a shorter LOS were estimated using HCUP data that were compiled before the launch of rivaroxaban. While the data indicate that a shorter LOS can reduce costs, as demonstrated in the current analysis, it is important to note that this savings is not explicitly associated with any particular treatment and does not include any additional outpatient monitoring or treatment that may be required after hospitalization. Patient access to outpatient thrombosis services and cost incentives for early discharge could have affected decisions about admission and dischargeCitation24. Treatment practice in participating hospitals may also play a role. Finally, both clinicians and patients may demonstrate different behaviors when they are being studied, so our results may not reflect real-world practice.
Conclusions
In the North American EINSTEIN cohort, hospitalized patients with VTE who received initial treatment with rivaroxaban had a significantly shorter hospital LOS compared with patients who received enoxaparin/VKA. Treatment with rivaroxaban could potentially ease the clinical and economic burden of VTE by enabling earlier discharge, while the convenience of a single-drug approach with rivaroxaban may facilitate easier transition from hospitalization to outpatient care than would be possible with LMWH/VKA therapy.
Transparency
Declaration of funding
This research was funded by Janssen Scientific Affairs, LLC, Raritan, NJ, USA and Bayer. LB and MW were responsible for conducting the analyses. All authors have contributed to the elaboration of the study design and the methodology, the interpretation of the results, the development and writing of the draft manuscript, and have approved the current version.
Declaration of financial/other relationships
BB, LH, and JS are employees and stockholders of Janssen Scientific Affairs, LLC (a Johnson & Johnson company). LB is an employee of Bayer Pharma AG and is also a stockholder. MW is an employee of Bayer Healthcare Pharmaceuticals. SM is a former employee for Janssen Scientific Affairs, LLC, who was employed at Janssen when this manuscript was developed. He is a stockholder of Janssen Scientific Affairs, LLC (a Johnson & Johnson company). JME peer reviewers on this manuscript have no relevant financial or other relationships to disclose.
Acknowledgments
The authors would like to acknowledge Ruth Sussman, PhD, who provided editorial support with funding from Janssen Scientific Affairs, LLC.
References
- Gould MK, Garcia DA, Wren SM, et al. Prevention of VTE in nonorthopedic surgical patients: antithrombotic therapy and prevention of thrombosis. 9th edn. American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest 2012;141(2 Suppl):e227S–77S
- Heit JA, Cohen AT, Anderson FA Jr, on behalf of the VTE Impact Assessment Group. Estimated annual number of incident and recurrent, non-fatal and fatal venous thromboembolism (VTE) events in the US. Blood 2005;106:Abstract 910
- Geerts WH, Pineo GF, Heit JA, et al. Prevention of venous thromboembolism: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest 2004;126:338S–400S
- Kearon C, Akl EA, Comerota AJ, et al. Antithrombotic therapy for VTE Disease: antithrombotic therapy and prevention of thrombosis. 9th edn. American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest 2012;141(2 Suppl):e419S–94S
- Knight KK, Wong J, Hauch O, et al. Economic and utilization outcomes associated with choice of treatment for venous thromboembolism in hospitalized patients. Value Health 2005;8:191–200
- Prandoni P, Lensing AW, Buller HR, et al. Comparison of subcutaneous low-molecular-weight heparin with intravenous standard heparin in proximal deep-vein thrombosis. Lancet 1992;339:441–5
- The Columbus Investigators. Low-molecular-weight heparin in the treatment of patients with venous thromboembolism. N Engl J Med 1997;337:657–62
- Panis LJGG, Kolbach DN, Hamulyak K, et al. Identifying inappropriate hospital stay in patients with venous thromboembolism. Eur J Intern Med 2004;15:39–44
- Caprini JA, Tapson VF, Hyers TM, et al, for the NABOR Steering Committee. Treatment of venous thromboembolism. Adherence to guidelines and impact of physician knowledge, attitudes, and beliefs. J Vasc Surg 2005;42:726–33
- Stein PD, Hull RD, Matta F, et al. Early discharge of patients with venous thromboembolism: Implications regarding therapy. Clin Appl Thromb Hemost 2010;16:141–5
- Turpie AG, Lassen MR, Eriksson BI, et al. Rivaroxaban for the prevention of venous thromboembolism after hip or knee arthroplasty. Pooled analysis of four studies. Thromb Haemost 2011;105:444–53
- Prins MH, Lensing AW, Bauersachs R, et al. Oral rivaroxaban versus standard therapy for the treatment of symptomatic venous thromboembolism: a pooled analysis of the EINSTEIN-DVT and PE randomized studies. Thromb J 2013 Sep 20;11(1):21
- van Bellen B, Bamber L, Correa de Carvalho F, et al. Reduction in the length of stay with rivaroxaban as a single-drug for the treatment of deep vein thrombosis and pulmonary embolism. Curr Med Res Opin 2014;30:829–37
- Bauersachs R, Berkowitz SD, Brenner B, et al. Oral rivaroxaban for symptomatic venous thromboembolism. N Engl J Med 2010;363:2499–510
- Buller HR, Prins MH, Lensin AW, et al. Oral rivaroxaban for the treatment of symptomatic pulmonary embolism. N Engl J Med 2012;366:1287–97
- Agency for Healthcare Research and Quality. VTE: Preventing hospital-acquired venous thromboembolism. Rockville, Maryland: AHRQ. www.ahrq.gov/qual/vtguide/vtguideapa.htm. Accessed December 11, 2013
- Spyroupoulos AC, Lin J. Direct medical costs of venous thromboembolism and subsequent hospital readmission rates: an administrative claims analysis from 30 managed care organizations. J Manag Care Pharm 2007;13:475–86
- Knight KK, Wong J, Hauch O, et al. Economic and utilization outcomes associated with choice of treatment for venous thromboembolism in hospitalized patients. Value Health 2005;8:191–200
- Huse DM, Cummins G, Taylor DC, et al. Outpatient treatment of venous thromboembolism with low-molecular- weight heparin: an economic evaluation. Am J Manag Care 2002;8:S10–S16
- Elting LS, Escalante CP, Cooksley C, et al. Outcomes and cost of deep venous thrombosis among patients with cancer. Arch Intern Med 2004;164:1653–61
- O’Brien JA, Caro JJ. Direct medical cost of managing deep vein thrombosis according to the occurrence of complications. Pharmacoeconomics 2002;20:603–15
- Rymes NL, Lester W, Connor C, et al. Outpatient management of DVT using low molecular weight heparin and a hospital outreach service. Clin Lab Haem 2002;24:165–70
- Lin J, Lingohr-Smith M, Kwong WJ. Incremental health care resource utilization and economic burden of venous thromboembolism recurrence from a U.S. payer perspective. J Manag Care Pharm 2014;20:174–86
- Aujesky D, Stone RA, Kim S, et al. Length of hospital stay and postdischarge mortality in patients with pulmonary embolism: a statewide perspective. Arch Intern Med 2008;168:706–12