

Abstract
Background:
Parkinson’s disease (PD) is the second most common neurodegenerative disease, affecting ∼5.2 million people worldwide. Continuous subcutaneous apomorphine (CSAI) represents an alternative treatment option for advanced PD with motor fluctuation. The purpose of this analysis was to estimate the cost-effectiveness of CSAI compared with Levodopa/carbidopa intestinal gel (LCIG), Deep-Brain-Stimulation (DBS) and Standard-of-care (SOC).
Methods:
A multi-country Markov-Model to simulate the long-term consequences, disease progression (Hoehn & Yahr stages 3–5, percentage of waking-time in the OFF-state), complications, and adverse events was developed. Monte-Carlo simulation accounted for uncertainty. Probabilities were derived from RCT and open-label studies. Costs were estimated from the UK and German healthcare provider’s perspective. QALYs, life-years (LYs), and costs were projected over a life-time horizon.
Results:
UK lifetime costs associated with CSAI amounts to £78,251.49 and generates 2.85 QALYs and 6.28 LYs (€104,500.08, 2.92 QALYs and 6.49 LYs for Germany). Costs associated with LCIG are £130,011.34, achieves 3.06 QALYs and 6.93 LYs (€175,004.43, 3.18 QALYs and 7.18 LYs for Germany). The incremental-cost per QALY gained (ICER) was £244,684.69 (€272,914.58). Costs for DBS are £87,730.22, associated with 2.75 QALYs and 6.38 LYs (€105,737.08, 2.85 QALYs and 6.61 LYs for Germany). CSAI dominates DBS. SOC associated UK costs are £76,793.49; 2.62 QALYs and 5.76 LYs were reached (€90,011.91, 2.73 QALYs and 6 LYs for Germany).
Conclusions:
From a health economic perspective, CSAI is a cost-effective therapy and could be seen as an alternative treatment to LCIG or DBS for patients with advanced PD.
Introduction
Parkinson’s disease (PD) is one of the most common neurological disorders, affecting ∼5.2 million men and women worldwide in 2004Citation1. For Germany, the mean estimated PD prevalence was 6607/100,000 (CI range = 713–12,500/100,000)Citation2. Crude incidences in Europe range from 5–26/100,000, according to systematic literature searchCitation2.
PD is defined by the occurrence of hypokinesia (slowness in movements), together with rigidity (muscle stiffness), tremor and/or postural disturbance. PD does, however, also cause a large number of non-motor symptoms, including dementia. Dopamine replacement therapies, especially levodopa, provides significant sustained benefit. However, it is reported that over the year’s treatment loses its efficacy and a number of complications, like motor fluctuation (on-off fluctuation) and dyskinesia, appear due to the progressive loss of dopaminergic neurons and their striatal and cortical connectionsCitation3. These complications are observed in 50% of patients after 5 years of disease and in 80% of patients after 10 years of treatmentCitation4. This can initially be counteracted by adjustments of the oral/transdermal medication, but, in advanced PD (aPD), disabling motor fluctuations often escape control of oral medications. The last 25 years has seen significant progress in the management of patients with aPD with the development of Deep-Brain-Stimulation (DBS), continuous subcutaneous apomorphine infusion (CSAI), and infusion of levodopa/carbidopa intestinal gel (LCIG) in the proximal part of the small intestine. CSAI and LCIG with portable minipumps are the two clinically established forms of continuous drug deliveryCitation5. These treatments can bring considerable improvements in motor and non-motor PD symptoms, as well as in health-related quality-of-life, when applied instead of or additionally to standard peroral/transdermal PD treatments. DBS has been proven to be effective in off-time and dyskinesia reduction and provide significantly greater benefit for quality-of-life than conventional medical treatmentCitation5,Citation6.
Health economic analyses in aPD treatment are rare. Eggington et al.Citation7, Dams et al.Citation8, and Tomaszewski and HollowayCitation9 have compared DBS with pharmacotherapy. Lowin et al.Citation10 have estimated cost-effectiveness of LCIG compared to standard of care (SOC). ValldeoriolaCitation11 has compared DBS, LCIG, and CSAI over a time horizon of 5 years. The aim of the present study was to determine long-term clinical, quality-adjusted life year, and cost outcome associated with the use of these three alternatives compared to SOC (combination of oral pharmacotherapies) in patients with aPD.
Methods
Model design
To investigate the cost-effectiveness of the use of CSAI, LCIG, DBS, and SOC, a probabilistic Markov-Model was developed to simulate the long-term consequences, disease progression, waking-time in the OFF, complications, and adverse-events (AE). Disease progression is expressed with the aid of the Hoehn & Yahr (H&Y) scale, which is a commonly used system describing the progress of symptoms of Parkinson’s disease. Stage 3–5 is characterized as an advanced state, from mild/moderate disability with impaired postural reflexes, to confinement to bed or wheelchair use.
The model is adopted on models which have been previously published for the UK and SwedenCitation10,Citation12,Citation13. Unit costs and outcomes, described as quality-adjusted life-years (QALYs) and life-years (LYs), were projected over a life-time horizon and were discounted according to the national guidelines (3.5% for the UK and 3% for Germany)Citation14,Citation15. The perspective of the analysis is that of the national healthcare providers.
The Markov model assumes that aPD patients enter the model in H&Y status 3, 4, or 5 experiencing more than 50% of waking time (14 h) in the OFF state at treatment initiation and move from state to state according to a set of transition probabilitiesCitation10,Citation16. Transition to the next state depends on the disease progression and the incidence rate of complications and AE during therapy. The model was developed so that one cycle of the model represents a 6-month time frameCitation17.
The Markov model consists of 12 aPD health states (combined H&Y and percentage of waking time in OFF), complications, AE with treatment stop, and the possibility of treatment switch and death (). A cohort of patients with aPD and H&Y status 3, 4, or 5, who experience more than 50% of waking time in the OFF state, enters the model. These characteristics are representative for patients switch to continuous drug deliveryCitation10,Citation17. The initial patient distribution was assumed to be 25% in H&Y 3, 50% in H&Y 4, and 25% in H&Y 5, and is according to Lowin et al.Citation10 and corresponds with patient characteristics from a synopsis of 19 open label studies, including 406 patients using CSAI. The median H&Y stage in this aPD population was 4.1 (range = 3–5) with a median duration of disease of 14.1 years (range = 10–19.2). The median age of patients was 59.1 years (range = 52–67). According to Lowin et al.Citation10, OFF states were split in OFF I (0–25% of time in OFF), OFF II (26–50% of time in OFF), OFF III (51–75% time in OFF), and OFF IV (76–100% of time in OFF). After treatment initiation with CSAI, LCIG, or DBS, an improvement in health states in the following cycle arises due to treatment start with continuous drug delivery or surgery (see transition probabilities). Patients with aPD receiving SOC experience disease progression without improvement (). SOC is defined as best available non-invasive pharmacotherapy. During different therapeutic alternatives AE and/or complications may arise. In the case of intolerable adverse events, patients have the opportunity to switch to an alternative treatment. Patients receiving first-line CSAI or LCIG switch to DBS, a more invasive procedure. If necessary, patients after a DBS increase SOC medication. Patients may move from all health states to death. The number of patients exiting a health state at the end of each 6-month cycle was governed by time-dependent transition probabilities.
Figure 1. Markov model design. Model overview showing the possible transitions between health states. A patient could be in only one of 12 possible aPD states during a single cycle (combined H&Y and percentage of waking time in OFF) without or with complications, AE, and death.

Table 1. Model inputs: transition probabilities, AE and complication rates.
To assess the robustness of our findings we first performed deterministic sensitivity analyses. In addition, a probabilistic sensitivity analysis was performed by incorporating probability distributions of the input variables by means of a second order Monte Carlo simulation. Each simulation was based on a different value drawn randomly from the distribution of each variable. Second order Monte Carlo simulations of 500 hypothetical patients were performed. This analysis was based on the distributions of all input variables.
The model was constructed and analysed using TreeAge Pro 2011 ().
Transition probabilities
PD health states were defined by H&Y staging and the amount of time spent in OFF experienced per waking hours. The transition probabilities between health states are derived from Lowin et al.Citation10, who had reported progression rates for SOC (). Time-adjusted treatment effects, expressed as reduced OFF time from baseline, were calculated for the CSAI, LCIG, and the DBS armCitation6,Citation18–29. According to Lowin et al.Citation10, patients may experience initial benefit due to their treatment switch during the first cycle of the model. The benefit of treatments is reflected by a considerably reduced time in the OFF state and improvement in H&Y scores. Rates were calculated based on the improvement from baseline expressed as a percentage reduction of OFF time after a 6-month follow-up in pooled clinical trialsCitation6,Citation18–29. Data suggests that CSAI patients spend 0.35 less time in OFF, LCIG 0.40, and DBS 0.37 compared to SOC. After improvement in the first cycle all CSAI, LCIG, and DBS patients were, therefore, distributed in the OFF I health state, while SOC patients remain in OFF II and OFF III. In the first cycle 44% of CSAI patients experienced an improvement in H&Y stage; 47% of LCIG patients and 46% of patients with DBSCitation6,Citation18–29.
In the subsequent cycles, patients may move to a worse H&Y state and/or OFF category but cannot experience further improvement. Treatment benefit is expressed as delayed disease progression due to improvement in the first cycle. This is an established approach to measure the progression in PD patientsCitation2,Citation9,Citation10,Citation21,Citation22,Citation29–31.
According to our data pooling the efficacy (time in OFF) of CSAI has been evaluated in monotherapy or as an add-on to levodopa/SOC therapy in aPD through several open-label studies including more than 400 patients. CSAI is able to reduce OFF time by more than 50% (40–85%) and decrease pre-existing levodopa dyskinesia significantlyCitation32.
Most LCIG studies focused on motor symptoms and showed that patients with LCIG have spent more time in motor states near normal performance and less time in OFF and dyskinetic states as compared to conventional optimized therapy. The majority of studies are open-label. LCIG is able to reduce OFF time by 29–87%Citation25–28.
A randomized trial compared DBS treatment plus medication with medical managementCitation6. In the trial, 156 patients were enrolled with aPD and severe motor symptoms. With DBS, the period of immobility was reduced by 4.2 h and the period of mobility without dyskinesia was increased by 4.4 h. The time spent sleeping was increased by 0.7 h. The period of mobility with troublesome dyskinesia was also significantly reduced.
Patients with aPD develop several motor and non-motor complications with a dramatic impairment of their quality-of-life (QoL). This fact influences QALYs, resource use, costs, and, finally, influences the results. A methodological review by Dams et al.Citation33 claims to consider AE of treatment, co-morbidities, or disease complications, which are not yet sufficiently included in the models to adequately represent clinical reality.
Incidence of motor, non-motor complications, and other AE and complications were derived from clinical trials. All probabilities were adjusted to Markov cycle length by means of the actuarial method to make it usable for calculation.
The rate and types of device-related complications associated with LCIG are based on data reported by Lowin et al.Citation10. DBS complications like surgical death and surgical complications—temporary and permanent (5.4%)—were obtained from Tomaszewski and HollowayCitation9 ().
Cost assessment
The cost assessment is based on the assignment of costs to the health states. The costs of each health state are determined by the resource utilization associated with a health state. Resource use (e.g., the type and frequency of medical goods and services rendered to the patient) and monetary value (prices, tariffs, and/or opportunity costs) for each unit of medical goods and services were used to calculate the total direct costs. In order to estimate the cost of aPD and related costs including the AE and complication costs in the UK and Germany, direct costs were included in the analysis.
Health state costs (H&Y and OFF stages) were calculated based on the resource use data of Findley et al.Citation34, which were multiplied with national recent unit costs of both healthcare systems. Resource use includes the number of hospitalizations per health state, physician consultations, and number of tests like MRI, CT, and SPECT. Findley et al. evaluated the cost burden of patients with aPD according to the waking hours per day spent in OFF state by analyzing the resource use data (medical services, professional care, and informal care) from an observational, cross-sectional study with 302 PD patients at H&Y stages 3–5 (see supplement material). Furthermore, it is possible to apply the resource use data also for Germany, as routine consultation and tests are elements of the German Parkinson’s guidelines.
CSAI costs per day were calculated based on the average dosage per day (75 mg) for the continuous s.c. therapyCitation18–24 multiplied with the apomorphine mg price. Therapy change to CSAI leads to a reduction of medication vs SOC of 42.44%Citation18–24. It is reported that co-medication includes: Levodopa (96% of patients), Dopamine agonist (40%), apomorphine (intermittend injection) (17%), COMT inhibitors (16%), MAO inhibitors (10%), and amantadine (18%)Citation24. All aDP on CSAI therapy are receiving domperidone treatment to reduce nausea.
LCIG is given as mono-therapy or in combination during daytime. A long-acting peroral L-dopa and/or dopamine agonist dose is then given in the late evening to cover the night. Co-medication of patients receiving LCIG includes: Levodopa (72%), dopamine agonist (20%), COMT inhibitors (17%), and MAO inhibitors (10%)Citation28. At treatment beginning the patient is admitted to hospital where the clinical response to Duodopa is administered via a temporary nasoduodenal tube. Upon a successful response to this test a permanent PEG tube is inserted and the administration of Duodopa is continued using a portable pump. Costs also include supplies like Duodopa cassettes, replacement connectors, tubes, carrying holsters, etc. Costs for Duodopa-related problems were derived from the literature.
Costs for DBS surgery were derived from national literature and include implantable pulse generator, electrode, extension lead, patient controller, accessory kit, and re-hospitalizationCitation9,Citation35. A pulse generator replacement was calculated for every 4 years. Patients with permanent complications (intracerebral hematoma, paralysis, removal of implants, leads, or pulse generator) were assumed to incur a one-time up-front cost. Temporary complications (subcutaneous infections, transient mental effects) were estimated according to Tomaszewski and HollowayCitation9. Patients receiving DBS who have either temporary or no complications require less pharmacotherapy. The reduction amounts to ∼43%Citation9.
SOC medication includes levodopa (99%), dopamine agonist (84%), apomorphine injection (54%), COMT inhibitors (4%), MAO inhibitors (70%), and amantadine (23%), and were derived from the study by García Ruiz et al.Citation18.
Patients exhibiting AE have a higher resource use, e.g., dyskinesia leads to two additional specialist consultations for medication adjustments, somnolence one GP visit, dizziness two additional specialist consultations, etc. Depression (e.g., citalopram tablets 20 mg), hallucination (aripiprazole 15 mg), and grade 3/4 nausea (domperidone 10 mg) require additional medication. All cost data were presented in . All data represents costs from 2014.
Table 2. Costs for resources used.
Health state utilities
Utilities are a measure of preference between health states and were obtained for this model by pooling information from international literature of aPD. Where necessary data were re-expressed on a utility scale from 0–1 (where 0 represents death and 1 full health) by using weighting factors. Utilities were measured in quality-adjusted life years (QALYs). Utility values were mainly derived from the publication of Lowin et al.Citation10 due to a comparable patient group. Utilities were reported based on the EuroQol Group 5-Dimension Self-report Questionnaire (EQ-5D). To avoid negative utilities, relative decrements for OFF stage reduction in the health state H&Y 3 were also applied for higher H&Y stages. When utilities are multiplied by the lengths of time individuals spend in their respective health state, the result represents a quality-adjusted life expectancy, reflecting both the quantity and quality of remaining life yearsCitation36. No country-specific utility values were used. It is assumed that these utilities could be applied to the UK and Germany ().
Table 3. Utilities per year.
Results
Base case
Total costs over a lifetime horizon range from £78,251.49 for SOC to £130,011.34 for LCIG in the UK perspective (€90,011.91 for SOC to €175,004.43 for LCIG in Germany). Per-patient costs for aPD treatment with CSAI are estimated at £78,251.49 in the UK and €104,500.08 in Germany. CSAI therapy resulted in a discounted quality-adjusted life expectancy of 2.85 years in the UK and 2.92 in Germany. The corresponding life expectancy without quality adjustment amounts to 6.28 LYs in the UK and 6.49 LYs in Germany.
LCIG are associated with the highest total costs in both countries; £130,011.34 for the UK and €175,004.43 for Germany. Quality-adjusted life expectancy is the highest compared to all comparators. DBS associated total costs amounts to £87,730.22 in the UK and €105,737.08 in Germany. Per patient, cost for SOC treatment represents the lowest total cost as well as lowest QALYs and LYs vs comparators ().
Table 4. Base case results.
Summarizing the analysis exhibits the following points: CSAI dominates DBS in the UK and show comparable results for Germany. With an ICER of £6440.45 CSAI is cost-effective against SOC in the UK. In Germany the ICER is several times higher (€74,695.62). LCIG is associated with the highest costs and an ICER vs CSAI of £244,684.69 in the UK and €272,914.58 in Germany which exceeds established cost-effectiveness thresholds. Results of lifetime costs and outcomes have to be interpreted as costs and outcomes of a treatment algorithm because a treatment switch is incorporated in the model.
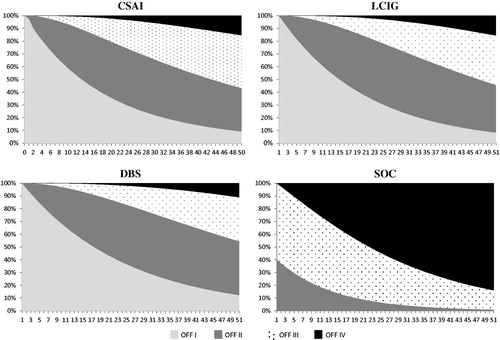
Additional analyses explored the impact of treatment on the time spent in OFF states. The expected distribution of patients over time spent within OFF differed according to the treatment arms (). CSAI, LCIG, and DBS patients spent less time in higher OFF states compared to patients maintained on SOC. This is important as the time spent in OFF significantly impacts HRQoL. Our calculation estimates that CSAI patients spent 69% of their remaining lifetime in OFF I stage, 24% in OFF II, 6% of time in OFF III, and 1% in OFF IV. Patients treated with LCIG spent 76% of their lifetime after treatment start in OFF I, 20% in OFF II, 3% in OFF III, and 1% in OFF IV. DBS shows the following effect: patients spent 78% of time in OFF I state, 19% in OFF II, 2.5% in OFF III, and 0.5 in OFF IV. Compared to that, patients remaining on SOC therapy spent 27% of time in OFF II, 57% in OFF III, and 16% in OFF IV stage.
Figure 2. Cohort distribution of comparators. Figures are based on cycle-observations after initial treatment effects (after first 6 months) and show the distribution of patients alive spent in different OFF states over months. Time expressed in months is reported along the x-axis.
Sensitivity analysis
When performing the deterministic sensitivity analysis we vary the cohort distribution, initial effect, costs, discount rate, and utility inputs. Among inputs considered the initial treatment effect and the discount rates exhibit the greatest influence. ICER for CSAI vs LCIG range between £150,623.60–£275,500.82 in the UK (€196,711.17–€346,978.58 in Germany). CSAI marginally dominates DBS in all variations. The ICER for CSAI vs SOC range from being dominant to £57,250.51 for the UK (dominant to €300,230.22 in Germany) ().
Table 5. Deterministic sensitivity analysis.
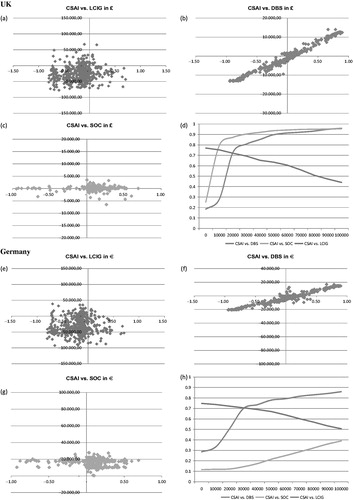
Monte Carlo probabilistic sensitivity analysis, results of 500 patient’s incremental cost vs incremental effects, revealed that CSAI is cost-effective against SOC in more than 87% of simulations in the UK with a willingness-to-pay-value up to £20,000; in 73% compared to DBS and in 72% compared to LCIG. In the German healthcare systems CSAI is cost-effective compared to LCIG in more than 72% of simulations with a willingness-to-pay threshold of €20,000, in more than 50% compared to DBS and in more than 12% against SOC ().
Figure 3. Probabilistic sensitivity analyses. The scatterplot of the Monte Carlo probabilistic analysis shows results of 500 patients incremental cost vs incremental effect. UK: (a) Scatterplot CSAI vs LOCIG; (b) Scatterplot CSAI vs DBS; (c) Scatterplot CSAI vs. SOC; (d) Acceptability curve. Germany: (e) Scatterplot CSAI vs LCIG; (f) Scatterplot CSAI vs DBS; (g) Scatterplot CSAI vs SOC; (h) Acceptability curve. Values are reported (x-axis) as £/quality-adjusted life-years (QALY) for UK and €/QALY for Germany.
Discussion
Preliminary evidence shown in our analysis suggests that CSIA, LCIG, and DBS are more effective methods to treat patients with advanced PD than SOC. When CSIA costs are compared with those of SOC, CSIA appears marginally more costly, namely with £1458.00 over the lifetime of a patient, but results in a higher QALYs (+0.23). Significantly better QALYs can also be reached with LCIG (+0.44%) and DBS (+0.13). Improvements in QoL are substantial and should not be ignored, despite the high attendant costs of alternative treatment options in comparison to SOC. Other treatments like CSIA, LCIG, and DBS for aPD do not yield dissimilar results.
Our evidence is supported by the fact that other analyses arrive at similar results; for example Lowin et al.Citation10 compared LCIG with SOC. Lifetime analysis yields an incremental cost per QALY of £36,024 for LCIG compared to SOC (incremental cost £39,644, QALY gain 1.1). The QALY gain is significantly higher compared to our results, which appear to be due to negative utility values in worse health states. Results were sensitive to time on treatment, health state on treatment initiation, and estimates of long-term benefit (one-way sensitivity analysis results from £32,127–£66,421 per QALY).
Another study was performed on LCIG treatment costs, but results have only been presented in oral and abstract formCitation37. According to this study, 2 years of LCIG treatment would cost US$93,600, which should be compared with US$28,700 for the previous conventional treatment. The cost per additional quality-adjusted life-year based on these calculations was 1.02 million US$, which is above conventional cost-effectiveness thresholdsCitation38.
Dams et al.Citation8 compare DBS with medical treatment in the German healthcare setting. In the base-case analysis, mean discounted lifetime costs amount to €126,200 for medical treatment and €133,200 for DBS. These results are slightly higher than our findings in the case of DBS lifetime cost. Patients with medical treatment accumulate 10.6 discounted QALYs compared with 11.6 QALYs for patients receiving DBS. Achieved QALYs over lifetime and costs for SOC are significantly higher, as in the present calculations.
Tomaszewski and HollowayCitation9 compared DBS with SOC. DBS provides an additional 0.72 QALY and additional costs of US$35,000 compared with SOC and results in an ICER of US$49,000.
Eggington et al.Citation7 evaluated the cost-effectiveness of DBS combined with best medication treatment (BMT), vs BMT alone over a time horizon of 5 years from a UK payer perspective. Total discounted costs in the DBS and BMT groups over 5 years were £68,970 and £48,243, respectively, with QALYs of 2.21 and 1.21, giving an incremental cost-effectiveness ratio of £20,678 per QALY gained.
Apomorphine costs vary greatly in the published literature depending on whether total cost for subcutaneously administered apomorphine or just continuous subcutaneous infusion treatment is included. A German study by Dodel et al.Citation39, based on retrospective analysis of 409 patients, revealed that apomorphine patients with continuous subcutaneous infusion had medication costs of ∼€13,500 per year resulting in 3-times higher costs than conventional aPD treatment (H&Y stages 4–5). In a small analysis based on pure medication costs of few patients in Germany using apomorphine pump treatment, the yearly medication cost was estimated to be €73,000–€91,000Citation40.
Outcomes of our results correspond with findings from Zhao et al.Citation41, who analyze the progression of PD as evaluated by Hoehn and Yahr stages. A total of 695 patients (mean age = 65.2) were studied. The median time spent in H&Y stage 3, 4, and 5 were 25, 24, and 26 months, respectively. That means that patients spent 6 years and 10 months in the aPD health states. Life expectancy in our study ranges between 7.8–8.4 years in the different treatment groups (undiscounted).
This present analysis has several limitations. First, clinical data based on open-label studies include only a few patients. Second, head-to-head comparisons were not available. Third, regarding QoL, no differentiation was made in terms of treatment choice. Age, family income, social support, and all other factors were held constant. These factors may confound the effect on QoL. QoL data in PD are sparse and typically not captured in a randomized fashionCitation9.
Finally, the effects of the advanced therapies have never been compared in an adequate way. Clinical experience seems to indicate that CSAI could be slightly less effective than LCIG and DBS concerning motor symptomatology, but has the advantage of being less invasive and probably less expensive. Prospective, randomized studies will, however, be necessary to adequately compare the effects of these treatments on motor and non-motor symptomatology as well as HRQoL.
The first case control comparative multi-center study comparing LCIG with CSAI in similarly aPD patients reports a robust improvement in motor and quality-of-life scores, with a large effect size with both therapies, differential effects on Non-Motor Symptoms Scale, and confirms that apomorphine infusion may not worsen hallucinations and can help mood dysfunctionCitation42.
Patients with advanced PD who are not eligible for alternate treatments are currently maintained on SOC and show a clear unmet need for alternative effective treatment options, especially with regard to different demographic characteristics such as age and co-morbidities. The model presented found a substantial incremental gain in QALYs for CSAI compared to SOC (0.23 QALYs). CSAI could, therefore, be considered as a cost-effective alternative to DBS and LCIG in the cohort of patients for whom it is indicated. The findings of this analysis must be considered with the limitations outlined.
Transparency
Declaration of funding
This study was funded by a grant from EVER Neuro Pharma.
Declaration of financial/other interests
EW & PO have previously received lecture fees from EVER Neuro Pharma. JME peer reviewers on this manuscript have no relevant financial or other relationships to disclose.
References
- de Lau LML, Breteler Monique MB. Epidemiology of Parkinson’s disease. Lancet Neurol 2006;5:525-35
- von Campenhausen L, Bornschein B, Wick R, et al. Revalence and incidence of Parkinson’s disease in Europe. Eur Neuropsychopharmacol 2005;15:473-90
- Poewe WH, Lees AJ, Stern GM. Low-dose L-dopa therapy in Parkinson’s disease: a 6-year follow-up study. Neurology 1986;36:1528-30
- Schrag A, Quinn N. Dyskinesias and motor fluctuations in Parkinson’s disease A community-based study. Oxf J Med Brain 2000;123:2297-305
- Hilker R, Antonini A, Odin P. What is the best treatment for fluctuating Parkinson’s disease: continuous drug delivery or deep brain stimulation of the subthalamic nucleus? J Neural Transm 2011;118:907-14
- Deuschl G, Schade-Brittinger C, Krack P. A randomized trial of deep-brain stimulation for Parkinson’s Disease. N Engl J Med 2006;355:896-908
- Eggington S, Valldeoriola F, Chaudhuri KR, et al. The cost-effectiveness of deep brain stimulation in combination with best medical therapy, versus best medical therapy alone, in advanced Parkinson’s disease. J Neurol 2014;261:106-16
- Dams J, Siebert U, Bornschein B, et al. Cost-effectiveness of deep brain stimulation in patients with Parkinson’s disease. Mov Disord 2013;28:763-71
- Tomaszewski KJ, Holloway RG. Deep brain stimulation in the treatment of Parkinson’s disease: a cost-effectiveness analysis. Neurology 2001;57:663
- Lowin J, Bergman A, Chaudhuri KR, et al. A cost-effectiveness analysis of levodopa/carbidopa intestinal gel compared to standard care in late stage Parkinson’s disease in the UK. J Med Econ 2011;14:584-93
- Valldeoriola F. Cost and efficacy of therapies for advanced Parkinson’s disease. Barcelona, Spain: Institut de Neurociències, Hospital Clínic, Universitat de Barcelona, 2011
- Willis M, Persson U, Zoellner Y, et al. Reducing uncertainty in value-based pricing using evidence development agreements. The case of continuous intraduodenal infusion of levodopa/carbidopa (Duodopa) in Sweden. Appl Health Econ Health Policy 2010;8:1-10
- Findley LJ, Lees A, Apajasalo M, et al. Cost-effectiveness of levodopa/carbidopa/entacapone (Stalevo) compared to standard care in UK Parkinson’s disease patients with wearing-off. Curr Med Res Opin 2005;21:1005-14
- National Institute for Health and Clinical Excellence (NICE). Guide to the methods of technology appraisals. 2008. NICE, UK. http://www.nice.org.uk/media/B52/A7/TAMethodsGuideUpdatedJune2008.pdf. Accessed April 13, 2012
- IQWIG. Kosten und Nutzen in der Medizin Die Analyse von ‘Effizienzgrenzen‘: Allgemeine Methoden zur Bewertung von Verhältnissen zwischen Nutzen und Kosten; Cologne, 2009
- Sonnenberg FA, Beck JR. Markov models in medical decision making: a practical guide. Med Decsn Mak 1993;13:322-38
- Keeler E. Decision trees and Markov models in cost-effectiveness research. In: Sloan FA, ed. Valuing Health Care. Cambridge: Cambridge University Press, 1996. p. 185-205
- García Ruiz PJ, Ignacio AS, Pensado BA, et al. Efficacy of long-term continuous subcutaneous apomorphine infusion in advanced Parkinson’s disease with motor fluctuations: a multicenter study. Mov Disord 2008;23:1130-6
- Pollak P, Champay AS, Gaio JM, et al. Subcutaneous administration of apomorphine in motor fluctuations in Parkinson’s disease. Rev Neurol (Paris) 1990;146:116-22
- Gancher ST, Nutt JG, Woodward WR. Apomorphine infusional therapy in Parkinson’s disease: clinical utility and lack of tolerance. Mov Disord 1995;10:37-43
- Katzenschlager R, Hughes A, Evans A, et al. Continuous subcutaneous apomorphine therapy improves dyskinesias in Parkinson’s disease: a prospective study using single-dose challenges. Mov Disord 2005;20:151-7
- Chaudhuri KR, Critchley P, Abbott RJ, et al. Subcutaneous apomorphine for on-off oscillations in Parkinson’s disease. Lancet 1988;2:1260
- Stocchi F, Bramante L, Monge A, et al. Apomorphine and lisuride infusion. A comparative long-term study. Adv Neurol 1993;60:653-5
- De Gaspari D, Siri C, Landi A, et al. Clinical and neuropsychological follow up at 12 months in patients with complicated Parkinson’s disease treated with subcutaneous apomorphine infusion or deep brain stimulation of the subthalamic nucleus. J Neurol Neurosurg Psychiatry 2006;77:450-3
- Eggert K, Schrader C, Hahn M, et al. Continuous jejunal levodopa infusion in patients with advanced Parkinson disease: practical aspects and outcome of motor and non-motor complications. Clin Neuropharmacol 2008;31:151-66
- Antonini A, Isaias IU, Canesi M, et al. Duodenal levodopa infusion for advanced Parkinson’s disease: 12-month treatment outcome. Mov Disord 2007;22:1145-9
- Raudino F, Garavaglia P, Pianezzola C, et al. Long-term experience with continuous duodental levodopa-carbidopa infution (Duodopa): report of six patients. Neurol Sci 2009;30:85-6
- Lisitchkina H, Ide J, Zutter D. Therapieerfahrung mit der pumpengesteuerten en-teralen Infusion eines Levodopa/Carbidopa-Gels bei fortgeschrittenem Morbus Parkinson. Schweizer Archiv für Neurologie und Psychiatrie 2011;162:122-6
- Palmer CS, Schmier JK, Snyder E, et al. Patient preferences and utilities for ‘off-time’ outcomes in the treatment of Parkinson’s disease. Qual Life Res 2000;9:819-27
- Davey P, Rajan N, Lees M, et al. Cost-effectiveness of pergolide compared to bromocriptine in the treatment of Parkinson’s disease: a decision-analytic model. Value Health 2001;4:308-15
- Palmer CS, Nuijten MJ, Schmier JK, et al. Cost effectiveness of treatment of Parkinson’s disease with entacapone in the United States. Pharmacoeconomics 2002;20:617-28
- Ceballos-Baumann A. Continuous subcutaneous infusion therapy with the Apomorphine Pump. Akt Neurol 2011;38:17-26
- Dams J, Bornschein B, Reese JP, et al. Modelling the cost effectiveness of treatments for Parkinson’s disease: A Methodological Review. Pharmacoeconomics 2011;29:1025-49
- Findley LJ, Wood E, Lowin J, et al. The economic burden of advanced Parkinson’s disease: an analysis of a UK patient dataset. J Med Econ 2011;14:130-9
- Pereira E, Nandi D, Aziz T. Deep brain stimulation: an underused panacea? ACNR 2008;8:4
- Gold M, Siegel J, Russel L, et al, eds. Cost-effectiveness in health and medicine. Philadelphi, PA: WB Staunders, 1996
- Kristiansen IS, Bingefors C, Nyholm D, et al. The cost-effectiveness of continuous duodenal delivery of levodopa (Duodopa) in patients with severe Parkinsons disease [abstract]. Mov Disord 2005;20(10 Suppl):80
- Lundqvist C. Continuous levodopa for advanced Parkinson’s disease. Neuropsychiatr Dis Treat 2007;3:335-48
- Dodel R, Eggert KM, Singer MS, et al. Costs of drug treatment in Parkinsons disease. Mov Disord 1998;13:249-54
- Meissner W, Trottenberg T, Klaffke S, et al. Apomorphinterapie versus tiefe Hirnstimulation. Nervenarzt 2001;72:924-7
- Zhao YJ, Wee HL, Chan YH, et al. Progression of Parkinson’s disease as evaluated by Hoehn and Yahr stage transition times. Mov Disord 2010;25:710-6
- Reddy P, Martinez-Martin P, Todorova A, et al. The EuroInf Study: a multi-centre European comparative study of apomorphine versus intrajejunal levodopa infusion in a real life cohort of Parkinson’s patients [abstract]. Mov Disord 2013;28(1 Suppl):596
- The World Standard Drug Database. online database from SafeScript Limited, London. http://admin.safescript.com/. Accessed April 2, 2014
- LAUER Taxe [LAUER FISCHER GmbH web site]. online database from Lauer Fischer Germany. www2.lauer-fischer.de. Accessed April 12, 2014
- Personal Social Services Research Unit [The University of Kent]. Unit costs of health and social care 2011. Personal Social Services Research Unit PSSRU, Kent. http://www.pssru.ac.uk/pdf/uc/uc2011/uc2011.pdf. Accessed October 4, 2012
- EBM – einheitlicher Bewertungsmaβstab. Kassenaerztliche Bundesvereinigung. 2014. Kassenärtzliche Bubdesvereinigung, Berlin. http://www.kbv.de. Accessed April 16, 2014
- Farkouh RA, Wilson MR, Tarrants ML, et al. Cost-effectiveness of Rasagiline compared with first-line early Parkinson disease therapies. Am J Pharm Benefits 2012;3:99-107