

Abstract
Objective:
Studies have indicated that outcomes may differ by choice of flowable hemostat, but there is limited evidence in spine surgery. The objective of this study was to conduct a comparison of outcomes following use of advanced flowable hemostatic matrices in a large spine surgery population.
Methods:
This is an observational retrospective cohort analysis using Premier’s US Perspective Hospital Database. Two commonly-used hemostatic matrices (Floseal and Surgiflo kitted with thrombin) were compared in cases categorized as either major or severe spine surgery. Outcomes included complications, blood product administration, hospital length of stay (LOS), surgery time, and amount of matrix used in surgery.
Results:
Major spine surgery patients treated with Surgiflo were associated with increased risk of blood product transfusion (OR = 2.56, 95% CI = 1.79–3.65, p < 0.001), longer surgery time (+8.84 min, p < 0.0001), and increased product usage (+3.34 mL, p < 0.001), compared to Floseal; however, risk of complications and LOS did not differ by choice of matrix in this patient group. Severe spine surgery patients treated with Surgiflo were associated with longer surgical time (+26.9 min, p < 0.001) and increased product usage (+1.52 mL, p < 0.01), compared to Floseal; however, risk of complications, transfusion and LOS did not differ by choice of matrix in this patient group.
Limitations:
Inherent to limitations associated with database analysis, this study did not evaluate potential physician differences such as skill and experience, assess long-term outcomes, nor include cases with missing data.
Conclusion:
The results from this analysis indicated that surgery time, risk of blood transfusion, and amount of matrix used are greater with Surgiflo patients, compared to Floseal patients. Choice of matrix did not appear to impact hospital LOS or risk of surgical complications. Future research should evaluate the cost consequences of increased clinical and resource utilization by choice of hemostatic matrix in spine surgery.
Introduction
Failure to maintain hemostasis during surgery can result in excessive bleeding, thereby complicating procedures and increasing the risk of morbidity and mortalityCitation1–3. Of special concern during spinal surgery, significant bleeding can result in loss of visualization leading to nerve injury or dural tearsCitation4, and can cause additional complications, increase operative time, and necessitate intra-operative and post-operative blood transfusionsCitation4–6.
When bleeding cannot be controlled by conventional methods (such as suturing, cautery, or manual compression) or when conventional methods are impractical, topical hemostatic agents are often usedCitation7–10. These agents can be categorized as passive or active, referring to the mechanism of action by which the agents interact to assist the body’s natural clotting cascade. Passive agents act via bleeding site contact activation and promotion of platelet aggregation, and include collagens, cellulose, gelatins, and polysaccharide spheres. Passive non-flowable hemostats are often used to address bleeding, ranging from mild capillary oozing to more broad moderate bleeding. As such, surgical practicality and effectiveness of these agents is limited; for instance, in patients who have received heparin and at surgical sites that are actively bleeding or difficult to reachCitation4,Citation11.
Active agents act biologically on the clotting cascade and may include thrombin. Categories comprised of active agents are flowable topical hemostats and sealants, including fibrin sealants, polyethylene glycol (PEG) polymers, albumin and glutaraldehyde, and cyanoacrylateCitation12,Citation13. In the US the most commonly used topical hemostats, alone or in combination, include gelatin and thrombinCitation7.
Commonly used gelatin-thrombin based flowable advanced topical hemostats are Floseal Hemostatic Matrix (Baxter Healthcare Corporation, Deerfield, IL) and Surgiflo Hemostatic Matrix Kit with thrombin (Ethicon Incorporated, Somerville, NJ). These advanced hemostats are advantageous in surgery as they can conform to wound contours and fill deep lesions. Both products have been labeled as hemostatic matrices and exhibit both passive and active mechanisms of action in the blood clotting cascade via contact activation and active biological agents (e.g., thrombin).
Product packaging for both Floseal and Surgiflo Hemostatic Matrix Kits are configured to contain both the gelatin matrix and thrombin, which are combined to form the final agent. Surgiflo also comes in an alternative product packaging configuration, where only the stand-alone gelatin matrix is made available. Additionally, the Floseal Hemostatic Matrix comes in 5 and 10 mL kits, while the Surgiflo Hemostatic Matrix comes in 8 mL kits. Each of these types of various configurations has an independent product description and codes for identification and tracking by hospital facilities and the US Food and Drug Administration (FDA).
Advanced topical hemostat usage can decrease blood loss, reduce the need and/or amount of blood transfusion, avoid the need for systemic hemostatic drugs, and shorten time in the operating roomCitation14,Citation15. These benefits can potentially reduce intensive care unit and hospital lengths of stay, and thus reduce the cost of careCitation16.
Several prospective randomized clinical trials (RCT) have found that clinical efficacy of an advanced flowable hemostatic matrix comparatively to non-flowable topical hemostat (e.g., Gelfoam or SurgiCel) has resulted in significant reduction in time to hemostasis and greater control of bleeding by reducing patient blood lossCitation4,Citation11,Citation17. In particular a prospective study by Renkens et al.Citation4 of 127 spine surgery patients at four US centers compared outcomes associated with Proceed (a product configuration of Floseal for spinal applications) to Gelfoam + thrombin. They found that the Floseal treated patients exhibited greater clinical efficacy based on time to and successful rates of hemostasis and reduction in surgical times comparatively to non-flowable products (i.e., Gelfoam + thrombin). Studies in other specialties, such as cardiothoracic and vascular surgery, also have reported more favorable outcomes with flowable agents compared to non-flowables, including shorter time to hemostasis, reduced risk of transfusion, and reduced units of transfused bloodCitation8,Citation11,Citation17. This, along with other evidence, has led surgeons to choose an active flowable hemostatic matrix as an effective tool to address a broad range of active bleeding in surgery. This type of tool is of particular need in spine surgery, where visualization is critical to an efficient and successful surgery.
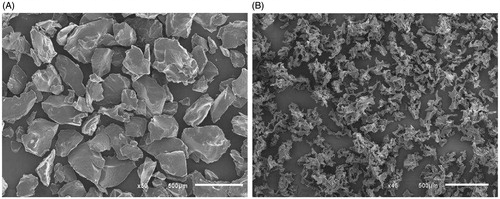
Two in-vivo animal studies evaluated Floseal and Surgiflo + thrombin in porcine liver models, and both reported faster and more effective hemostasis with FlosealCitation7,Citation18. Both studies concluded that the performance differences between these two flowable hemostatic matrices were due to the composition of the gelatin granules. That is, gelatin granule characteristics such as species type (bovine vs porcine), various shapes and sizes, smoothness, and surface areas were believed to lead to performance differences in these animal models. These animal studies, along with other simulated methods, indicate that the composition and characteristics of the gelatin granules could lead to performance differences in a human population (see ). However, despite the wide use of advanced hemostatic matrices in surgery, until recently, prospective or observational cohort studies comparing flowable hemostatic matrices have been limited.
Figure 1. Scanning electron microscopic images of (A) bovine-derived gelatin (Floseal) and (B) porcine-derived gelatin (Surgiflo). (Baxter data on file.)
Recently, an observational study analyzing the clinical outcomes of these gelatin-thrombin based flowable advanced topical hemostatic matrices in an observational cardiac surgery population, where different bleeds types are more numerous and the severity of bleeding during surgical cases can be aggressive, found that clinical outcomes and resource utilization were indeed different. This large population-based study found that Surgiflo (kitted with thrombin) treated patients were associated with significantly higher risks of complications, transfusions (rates and units), and longer surgery time, than Floseal treated patientsCitation19. However, there are no published human studies evaluating outcomes of these active flowable hemostatic matrices in a spine surgery population, where bleed types are more limited and the severity of bleeds range from broad diffuse capillary oozing to moderately brisk. Without such studies, we do not fully understand if clinical outcomes and resource utilization will be different in lower level bleed surgeries where the agents are also commonly used.
As such, the objective of this study was to conduct an observational cohort clinical evaluation and resource utilization analysis of the most commonly used advanced flowable hemostatic matrices (Floseal and Surgiflo kits) among a large spine surgery population using a large hospital-based quality and utilization benchmarking database.
Patients and methods
Study design
This observational cohort analysis assessed clinical outcomes and healthcare resource utilization between the most commonly used advanced hemostatic matrices (Floseal Hemostatic Matrix and Surgiflo Hemostatic Matrix Kit with thrombin) in spine surgery using Premier’s US Perspective Hospital Database.
Data source
Data were extracted from Premier’s US Perspective Hospital Database, developed for quality and utilization benchmarking, which contains over 490 million hospital encounters with ∼6 million added each month. Currently, the database captures ∼25% of hospital discharges in the USCitation20. Data include a date-stamped log of all billed items such as procedures, diagnoses, medications, laboratory, diagnostic/therapeutic services, costs, drugs, and medical devices received at the individual patient level during the hospitalization. Patient-specific data are de-identified in accordance with US Health Insurance Portability and Accountability Act (HIPAA) regulations to protect confidentiality. As such, there is no requirement for IRB approval or exemption, as it meets all current criteria set forth by the US Department of Health.
Patient selection criteria and study groups
Inclusion criteria for the study were as follows, and are shown in : Patients that underwent elective, emergent, or urgent spine surgeries with hospitalizations and discharges occurring between January 1, 2006 and June 30, 2013; and received flowable Floseal Hemostatic Matrix (either 5 mL or 10 mL) or flowable Surgiflo Hemostatic Matrix Kit with thrombin (8 mL) only, but not both, intra-operatively.
Figure 2. Patient selection criteria.
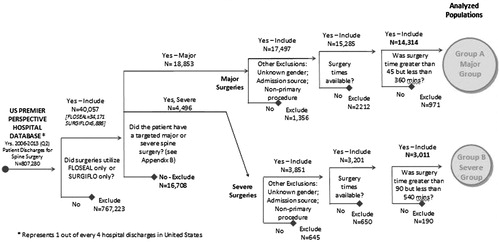
Targeted configurations of Floseal and Surgiflo were identified in the registry database based on itemized product descriptions and codes at the individual patient case level. Cases with other hemostatic agents, fibrin sealants, and sealants were eliminated from the study. The remaining individual patient cases were then identified using ICD-9 procedure codes for spine surgeries and were defined as either major or severe spine surgeries based on the categorization of spine surgery procedures performed during the hospitalization (see ). Major surgeries were categorized based on the requirement of a fusion/refusion of 2–3 vertebrae or a tumor resection spine procedure. Severe surgeries were defined as any of the following types of spine procedures: (1) fusion/refusion of 4–8 or 9+ vertebrae, (2) tumor resection with a corpectomy or fusion/refusion of more than 2+ vertebrae, (3) fracture stabilization with fusion/refusion of 2+ vertebrae, and (4) fracture stabilization with corpectomy or osteotomy, with fusion/refusion 2+ vertebras.
Table 1. Listing of primary or secondary ICD-9 procedural codes for group assignment.
Those patients excluded from the study were those surgery cases with missing baseline study variables and outcomes values. Also major surgeries with surgical times lasting less than 45 min or longer than 360 min and extreme surgeries lasting less than 90 min or longer than 540 min were excluded from the study; representing the lower and upper 2% of patients based on surgical time. This exclusion was made to eliminate the impact that observational outliers would have on study results.
Study variables
Patient characteristics included in the analysis were age, gender, race (white/black/other), Charlson comorbidity index (CCI) scoreCitation21, complexity of surgery, patient on anti-platelet/coagulants, and admission type (elective, emergent, or urgent). Hospital variables included teaching facility, bed size, and US region (see ).
Table 2. Selection patient and provider characteristics.a
Clinical outcomes were determined using ICD-9 diagnosis and procedure codes. The primary clinical outcomes of interest were (1) complications and (2) blood product administration. Complications were defined as (a) related to intra-operative blood loss (e.g., hemorrhage, anemia, thrombocytopenia, and hematoma complicating a procedure, visualization complication such as dural puncture during operation, embolic events, venous thrombosis); (b) severe (e.g., encephalopathy, sepsis, post-operative infection, acute respiratory failure); or (c) other (e.g., seroma complicating a procedure, urinary, cardiac, or respiratory complications, volume depletion/dehydration).
Blood product administration was defined as (a) any blood product transfusion during the hospitalization, (b) any blood product on Day 1 transfusion (surgery start to end of first day), (c) any blood product from Day 2–4, and (d) any pure blood transfusion (packed red blood cells) at any time during the hospitalization.
Healthcare resource utilization outcomes included (1) hospital length of stay (LOS) in days; (2) surgery time in minutes; and (3) amount of hemostatic matrix used during surgery.
Statistical analyses
Descriptive analyses were conducted on all key variables. Chi-square and student T-tests were used to assess whether the two study groups were equivalent. Logistic regression models were used to estimate risk of complications and transfusions between the two productsCitation22. Generalized linear models (GLM) with log link and negative binomial distribution (negative binomial regression) were used to compare surgery time, length of stay, and amount of hemostatic matrix used. Approximately the lower and upper 2% of the distribution of outcome data were excluded from each GLM as outliers. Cases with missing baseline values (e.g., gender or severity of illness codes) were excluded.
Values for unadjusted outcome rates, and adjusted odds ratios (OR) along with 95% confidence intervals (CIs) were reported from logistic regression analyses and adjusted differences (AD) from expected number of outcomes (e.g., LOS) were reported from GLM analyses. Study covariates used were: age, sex, race, CCI score, procedure severity type (major or severe), admission type, presence of anti-platelet/coagulants, hospital teaching status, hospital bed size, and US region. SAS version 9.3 was used to perform statistical analyses with a priori significance level of 0.05Citation23.
Results
Selected baseline patient population and provider characteristics of the major and severe spine surgery groups are shown in . The major spine surgery group inclusion represented 14,314 major spine surgeries, representing 12,783 (89.3%) kitted Floseal only and 1531 (10.7%) kitted Surgiflo only cases. The severe spine surgery group was comprised of 3011 cases, of which 2837 (94.2%) were kitted Floseal only and 174 (5.8%) were kitted Surgiflo only cases. All measureable patient and hospital variables were included in the regression analyses as covariates to control for the observed baseline differences. Outcomes from logistic and GLM regression analyses are presented in and . All model measures of goodness of fit were found to be acceptable. All logistic models had c-statistics values ranging from 0.7–0.9. All GLMs had a scaled deviance values/DF ranging from 0.7–1.0.
Table 3. Results of Group A.
Table 4. Results of Group B.
Major spine surgery group
Clinical outcomes
Complications
The risks of blood loss-related complications (OR = 1.10, 95% CI = 0.86–1.43, p = 0.44), severe complications (OR = 0.74, 95% CI = 0.44–1.25, p = 0.26), and other complications (OR = 0.99, 95% CI = 0.72–1.35, p = 0.94) were not significantly different between the Floseal and Surgiflo groups.
Blood–product administration
The risk of any blood product transfusion was greater in Surgiflo cases (OR = 2.56, 95% CI = 1.79–3.65, p < 0.001), as compared to Floseal cases. Risk of Day 1 transfusion was not statistically different between the Floseal and Surgiflo treated cases (OR = 1.58, 95% CI = 0.87–2.89, p = 0.13). There was greater risk of Surgiflo-treated cases receiving Day 2–4 transfusions (OR = 3.30, 95% CI = 2.20–4.98, p < 0.001) and any packed red-blood cell transfusions (OR = 2.54, 95% CI = 1.75–3.67, p < 0.001) than Floseal-treated cases.
Healthcare resource utilization
Hospital LOS (days)
After truncating cases for hospital LOS between 1–7 days, a total of 12,952 cases were identified. Floseal patients’ mean LOS was 2.8 days (95% CI = 2.7–2.8 days) and Surgiflo was 2.7 days (95% CI = 2.5–2.8 days). There was no statistically significant difference in LOS between Surgiflo and Floseal treated cases (AD = −0.11 days, p = 0.06).
Surgical time in minutes
Surgiflo-treated cases were associated with longer surgery times; 198 min (95% CI = 194–203 min) compared to 190 min (95% CI = 187–193 min) for Floseal-treated cases (AD = 8.84 min, p < 0.0001).
Amount of hemostatic matrix used during surgery
Surgiflo-treated cases were associated with more milliliters of hemostatic matrix product (AD = 3.35 mL, p < 0.0001) compared to Floseal-treated cases. Surgiflo adjusted mean product utilized was 10.99 mL and Floseal adjusted mean product utilized was 7.64 mL.
Severe spine surgery group
Clinical outcomes
Complications
The risks of intra-operative and blood loss-related complications (OR = 0.81, 95% CI = 0.50–1.32, p = 0.40), severe complications (OR = 0.62, 95% CI = 0.28–1.40, p = 0.25), and other complications (OR = 0.98, 95% CI = 0.52–1.84, p = 0.94) were not significantly different between the Floseal and Surgiflo groups.
Blood–product administration
The risks of any blood–product transfusions (OR = 1.42, 95% CI = 0.82–2.46, p = 0.21), Day 1 transfusions (OR = 0.66, 95% CI = 0.26–1.67, p = 0.38), Day 2–4 transfusions (OR = 1.60, 95% CI = 0.82–3.12, p = 0.17), and packed red-blood cells (OR = 1.28, 95% CI = 0.72–2.28, p = 0.41) were not significantly different between Surgiflo and Floseal treated cases.
Healthcare resource utilization
Hospital length of stay in days
After truncating cases for hospital LOS between 1–14 days, a total of 2852 cases were identified. Floseal patients’ mean LOS was 4.4 days (95% CI = 4.2–4.6 days) and Surgiflo was 4.3 days (95% CI = 3.9–4.8 days). There was no statistical difference in LOS between Floseal and Surgiflo cases (AD = −0.12 days, p = 0.57)
Surgical time in minutes
Surgiflo-treated cases were associated with longer surgery times; 293 min (95% CI = 276–311 min) compared to 266 min for Floseal (95% CI = 258–273 min) treated cases (AD = 26.94 min, p < 0.001).
Amount of hemostatic matrix used during surgery
Surgiflo-treated cases were associated with more hemostatic matrix (AD = 1.52 mL, p < 0.01) compared to Floseal-treated cases. Surgiflo adjusted mean product utilized was 11.71 mL and Floseal adjusted mean product utilized was 10.19 mL.
Discussion
Active flowable hemostatic matrices contain gelatin and thrombin that perform via contact activation and improve the clotting cascade to stop bleeding. The two most commonly used active flowable hemostatic matrices in the US are Floseal Hemostatic Matrix and Surgiflo Hemostatic Matrix. These active flowable agents have several advantages such as rapid hemostasis and precise application, as the gelatins in the flowable products fill and conform to the wound site shape, allowing versatility with delivery and effective tissue contact.
Multiple prospective randomized clinical trials (RCTs) across numerous surgical specialties have evaluated the clinical efficacy of an active flowable hemostatic matrix (Floseal) vs a passive non-flowable hemostat (e.g., Gelfoam or Surgicel). These studies found the hemostatic matrix (Floseal) to be clinically superior compared to these passive hemostats. In particular, Renkens et al.Citation4 found Floseal-treated spine surgery patients achieved a higher rate of successful hemostasis at 3 min and shorter surgical times. Other studies have also found Floseal to be associated with shorter times to reach successful hemostasis and surgical times, but also reductions in transfusions (rates and units) and reductions in complications. These studies provide evidence that flowable hemostatic matrices are effective in maintaining visualization via a blood-free surgical field and, therefore, may minimize risk of accidental nerve or dural injuries, lessen duration of surgery, and minimize transfusions needed due to blood loss. Furthermore, effective products can reduce the likelihood of continued bleeding, repeat applications, and product waste.
Two such hemostatic matrices used in spine surgery are Floseal, which has been on the US market since 2000, and Surgiflo, which has been available since 2006. Only a few previous studies have been conducted to compare the two products in clinical performance. In 2013, two studies analyzed liver abrasion animal models and reported that the active hemostatic matrices are different from one another based on demonstration in time and success of reaching hemostasisCitation7,Citation18. These studies reported that uniquely engineered characteristics of the gelatin granules were likely the contributing factors to performance differences. In 2014, Tackett et al.Citation19 performed an observational database study to analyze outcomes of these active flowable hemostatic matrices among a cardiac surgery population. This study found that, in this surgical population, where surgical bleed severity types are numerous and commonly range from diffuse capillary oozing to aggressive arterial spurting, there were differences in clinical outcomes amongst the two agents. This large study found that Surgiflo-treated patients were associated with a higher risks of complications, transfusions (rates and units), and longer surgery times, than Floseal-treated patients.
From these animal studies and the large observational study in cardiac surgery, we were uncertain if a detectable clinical outcome and healthcare resource utilization performance difference would exist in a human surgical population of less aggressive bleeds, when capillary oozing to moderate brisk bleeds are common and, therefore, less strain is being placed on the agents to maintain proper hemostasis vs the high strain aggressive bleed environment found in cardiac surgery.
Our objective in this study was to understand if the performance difference found in these prior studies would be transferable to a surgical population with less aggressive bleeds; ranging from broad diffuse mild capillary oozing to moderately brisk bleeds. As such, we chose to target a spine surgery population derived of major and severe procedures as this would provide a basis for a large patient population where only kitted Floseal or kitted Surgiflo are exclusively used as the hemostatic agent of choice for the surgery, where bleed types are commonly less aggressive, and visualization is key to a successful and efficient surgery.
To conduct this observational study, we sought a large registry type database (i.e., Premier Perspective US Hospital Database designed for quality and utilization reporting and benchmarking) to assess a major and severe spine surgery patient population. Of particular interest, we sought to understand the outcomes related to complications, transfusions rates, surgery time, hospital LOS and amount of utilized product in major and severe spine surgeries. This study represents the first and largest known observational evaluation of hemostatic matrices usage only in a spine surgery patient population. The study found that more patients are treated with Floseal than with Surgiflo, probably because of two facts: Floseal has been on the market for a longer period of time than Surgiflo, and Floseal has a much larger market share in the US across all major surgical specialties. Despite Floseal’s larger market share, we did find that teaching facilities appeared to use Surgiflo more frequently, but there is no known evidence-based clinical data to support increased use in teaching vs non-teaching hospitals.
We did find statistical differences between Floseal and Surgiflo patient populations represented in both the major and severe spine surgery groups. These baseline differences led to the selection of the 10 confounding factors that were applied to regression models to understand the influence that these factors had on baseline results. These confounding factors and statistical methodology of using logistic and GLM regression models are consistent to those used in the prior observational study of hemostatic matrices using the Premier US Hospital Database in Tackett et al.’sCitation19 cardiac surgery study. As such, given the large numbers of observations, ease of interpretation, and consistency with the prior study, we maintained the use of logistic and GLM regression models as the final method for reporting results in this spine surgery population. All models measures of goodness of fit were found to be acceptable. All logistic models had c-statistics values ranging from 0.7–0.9. All GLMs had a scaled deviance values/DF ranging from 0.7–1.0. While other types of data interaction might occur within this surgical patient population we do not believe there to be any significant interactions a priori.
We also noted that, from 2006–2013, usage of anti-fibrolytic agents such as tranexamic acid (TXA) and transfusion practices may have changed, although, while use may have increased in joint replacement surgery, it is utilized infrequently in spine surgery in particular. However, we analyzed the usage of TXA and found the following: In the Floseal group, 16 of 18,444 (<0.09%) had evidence of use, while in the Surgiflo group, one of 2894 (<0.04%) had evidence of use. Therefore, we did not believe that TXA had a meaningful impact on outcomes. Furthermore, we considered that transfusion practices, policies, and guidelines may have changed over time. However, we are not aware of any transfusion best-practice standard guidelines, medical policies or medical guidance that was adopted for implementation in spine surgery during the study time period. We made an assumption in our analyses that, based on commonly accepted practices without standardized guidelines or policies, transfusion practice would, therefore, vary from hospital to hospital and from surgeon to surgeon, not based a priori on choice of hemostat. As such, there was no evidence to indicate that surgeons choosing Surgiflo were more likely to also be biased toward more frequent transfusions as a general practice.
The results from this study indicate that Surgiflo treated patients were associated with higher risks for any transfusion of blood-related products, day 2–4 transfusions, packed red-blood cell transfusions, longer surgery times, and more volume of utilized product than Floseal-treated patients in major spine surgeries. In the severe spine surgery group, Surgiflo-treated patients were associated with longer surgery times and more volume of utilized product than Floseal-treated patients.
This study has inherent limitations associated with conducting retrospective observational evaluations of registry databases. For example, the registry database did not allow for: evaluation of potential physician differences such as skill and experience; assessment of long-term outcomes (as post-discharge data were not available); adjudication processes to eliminate registry reporting errors; evaluation of cases missed due to variation in diagnoses and/or procedures coding; and risk of selection bias and number of cases excluded typical for retrospective study design. Additionally, given the high variability in accounting methodologies of U.S. hospitals when reporting costs (i.e., variable, fixed, indirect and direct) this registry did not support the identification and classification of hospitals based on accounting methodology; which would be required as a confounding factor to perform an accurate cost study. Also recognized, US transfusion practices are not standardized as there are no medical policies or guidance, and, as such, transfusion results may reflect practice variations. Furthermore, the registry does not capture the amount of product wasted after surgery, only the choice and quantity of hemostatic kits. For example, in our analysis of major spine surgery, the mean Surgiflo product utilized was 11 mL, meaning that two 8 mL kits would have been opened on average, whereas, for Floseal, 7.6 mL was utilized and, thus, two 5 mL kits or one 10 mL kit would have been opened. Further studies are needed to understand the amount of unused product wasted after surgery due to configured product packaging sizes that could influence the amount of product used in this surgical patient population.
Many other databases could potentially be utilized; however, the US Premier Perspective Hospital Database, which was developed as a quality and utilization benchmarking reporting registry, has been sourced for these types of detailed observational evaluations for nearly two decades. The registry database is uniquely positioned as an optimal database by which to conduct such a large registry observational evaluation as detailed information regarding outcomes and utilization of inpatient resources is easily found at the patient level and are captured on a monthly basis. The registry database represents more than six million hospital encounters a month (which represents a capture rate of 25% across the US)Citation20. Thus, the study strengths include: an evaluation of a large number of cases in the US; a geographically dispersed patient population with a large number of treating physicians and teaching and non-teaching hospitals; a large sample size of spine surgeries where only hemostatic matrices were used; and uncommonly available detailed data on outcomes and resource consumptions from patient surgeries where a hemostatic matrix was used.
Avoidance of transfusions and healthcare resource utilization for spine surgery may present clinical and economic benefits to patients, physicians, hospitals, and payers. For example, operating room opportunity costs have been estimated at $15–$34 per minuteCitation21–26 and blood transfusion costs range between $522–$1183 per RBC unitCitation27. Reduction in transfusion rates, surgical time, and volume of product utilized to effectively treat patients can reduce overall clinical resource consumption and burdens associated with performing spine surgery and potentially improve efficiency due to improved operating room throughput (i.e., operating room capacity improvement).
Conclusions
This study yields important clinical and resource utilization outcomes for practicing healthcare providers, patient, and payers. This observational study analysis of a large spine surgery population, where commonly bleeds range from broad surface oozing to moderately brisk, suggests Floseal may be beneficial to Surgiflo in treating spine surgery patients. Major spine surgery patients treated with Floseal were associated with significantly lower risks of transfusions, less surgery time, and less utilized product than Surgiflo-treated patients. Additionally, in severe spine surgery, Floseal-treated patients were associated with less surgery time and decreased utilization of product than the Surgiflo-treated patients. Future research should build on this evidence by evaluating what the cost consequence of the increased clinical and resource utilization would have on total cost of care when choosing a hemostatic matrix in surgery.
Transparency
Declaration of funding
This study was funded by Baxter Healthcare Corporation. Baxter purchases data rights to Premier’s US Perspective Hospital Database.
Declaration of financial/other relationships
ST is an employee of Baxter Healthcare Corporation. A JME peer reviewer on this manuscript was an investigator on a cited trial.
Acknowledgments
We thank Therese Conner, PhD, for her manuscript writing assistance, Deborah Testa, PhD, for her contribution to dataset development, and Marc Rubinstein, MD, Michelle Reed Arnold, MD, Steve Czop, RPh, Diane Ito, MA, and Yan Xiong, MS, for their technical expertise and contributions.
References
- Levi M, Cromheecke ME, de Jonge E, et al. Pharmacological strategies to decrease excessive blood loss in cardiac surgery: a meta-analysis of clinically relevant endpoints. Lancet 1999;354:1940-7
- Karkouti K, Wijeysundera DN, Yau TM, et al. The independent association of massive blood loss with mortality in cardiac surgery. Transfusion 2004;44:1453-62
- Boucher BA, Traub O. Achieving hemostasis in the surgical field. Pharmacotherapy 2009;29:S2-7
- Renkens KL, Payner TD, Leipzig TJ, et al. A multicenter, prospective, randomized trial evaluating a new hemostatic agent for spine surgery. Spine 2001;26:1645-50
- Nuttall GA, Horlocker TT, Santrach PJ, et al. Predictors of blood transfusions in spinal instrumentation and fusion surgery. Spine 2000;25:596-601
- Triulzi DJ, Vanek K, Ryan DH, et al. A clinical and immunologic study of blood transfusion and postoperative bacterial infection in spinal surgery. Transfusion 1992;32:517-24
- Lewis KM, Atlee HD, Mannone AJ, et al. Comparison of two gelatin and thrombin combination hemostats in a porcine liver abrasion model. J Invest Surg 2013;26:141-8
- Nasso G, Piancone F, Bonifazi R, et al. Prospective, randomized clinical trial of the Floseal matrix sealant in cardiac surgery. Ann Thorac Surg 2009;88:1520-6
- Raga F, Sanz-Cortes M, Bonilla F, et al. Reducing blood loss at myomectomy with use of a gelatin-thrombin matrix hemostatic sealant. Fert Steril 2009;92:356-60
- Mozet C, Prettin C, Dietze M, et al. Use of Floseal and effects on wound healing and pain in adults undergoing tonsillectomy: randomised comparison versus electro-cautery. Eur Arch Otorhinolaryngol 2012;269:2247-54
- Oz MC, Cosgrove DM 3rd, Badduke BR, et al. Controlled clinical trial of a novel hemostatic agent in cardiac surgery. Ann Thorac Surg 2000;69:1376-82
- Samudrala S. Topical hemostatic agents in surgery: a surgeon’s perspective. AORN J 2008;88:S2-11
- Schreiber MA, Neveleff DJ. Achieving hemostasis with topical hemostats: making clinically and economically appropriate decisions in the surgical and trauma settings. AORN J 2011;94:S4-20
- Carless PA, Henry DA, Anthony DM. Fibrin sealant use for minimizing peri-operative allogeneic blood transfusion. Cochrane Database Syst Rev 2003;1:CD004171
- Albala DM, Lawson JH. Recent clinical and investigational applications of fibrin sealant in selected surgical specialties. J Am Coll Surg 2005;202:685-97
- Tomizawa Y. Clinical benefits and risk analysis of topical hemostats: a review. J Artif Organs 2005;8:137-42
- Weaver FA, Hood DB, Zatina M, et al. Gelatin-thrombin-based hemostatic sealant for intraoperative bleeding in vascular surgery. Ann Vasc Surg 2002;16:286-93
- Coenye KE, Bourgain C, Keibl C, et al. A qualitative morphological comparison of two haemostatic agents in a porcine liver trauma model. Surg Sci 2013;4:359-64
- Tackett SM, Calcaterra D, Magee G, et al. Real-world outcomes of hemostatic matrices in cardiac surgery. J Cardiothorac Vasc Anesth 2014;28:1558-65
- Finn T. Premier Perspectives database: Comparative effectiveness research (CER) - Validated. 2012; http://hcmatters.com/2012/04/premier-perspectives-database-comparative-effectiveness-research-cer-validated/. Accessed May 12, 2015
- Charlson ME, Pompei P, Ales KL, et al. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis 1987;40:373-83
- Zhang J, Yu KF. What's the relative risk?: a method of correcting the odds ratio in group studies of common outcomes. J Am Med Assoc 1998;280:1690-1
- SAS Institute Inc. SAS® 9.3 System options: reference, 2nd edn. Cary, NC: SAS Institute Inc, 2011
- Matin SF. Prospective randomized trial of skin adhesive versus sutures for closure of 217 laparoscopic port-site incisions. J Am Coll Surg 2003;196:845-53
- Bacchetta MD, Girardi LN, Southard EJ, et al. Comparison of open versus bedside percutaneous dilational tracheostomy in the cardiothoracic surgical patient: outcomes and financial analysis. Ann Thorac Surg 2005;79:1879-85
- Chatterjee A1, Payette MJ, Demas CP, et al. Opportunity cost: a systematic application to surgery. Surgery 2009;146:18-22
- Shander A, Hofmann A, Ozawa S, et al. Activity-based costs of blood transfusions in surgical patients at four hospitals. Transfusion 2010;50:753-65