
Abstract
This research aims to develop a low-cost audio prescription labeling (APL) system for visually-impaired people by using the RFID system. The developed APL system includes the APL machine and APL software. The APL machine is for visually-impaired people while APL software allows caregivers to record all important information into the APL machine. The main objective of the development of the APL machine is to reduce costs and size by designing all of the electronic devices to fit into one print circuit board. Also, it is designed so that it is easy to use and can become an electronic aid for daily living. The developed APL software is based on Java and MySQL, both of which can operate on various operating platforms and are easy to develop as commercial software. The developed APL system was first evaluated by 5 experts. The APL system was also evaluated by 50 actual visually-impaired people (30 elders and 20 blind individuals) and 20 caregivers, pharmacists and nurses. After using the APL system, evaluations were carried out, and it can be concluded from the evaluation results that this proposed APL system can be effectively used for helping visually-impaired people in terms of self-medication.
Introduction
The number of people in Thailand with vision impairment, reading disability, dyslexic or cognitive disability, and senior citizens is increasing (Ministry of Social Development and Human Security, 2014) and the (Foundation of Thai Gerontology Research and Development Institute, Citation2013). The number of all registered disabilities in Thailand was 1.73 million, from 1994 to 2013, and 10% of all registered people with disabilities are blind (Ministry of Social Development and Human Security, Citation2014). It was found from the National Statistical Office, Ministry of Information and Communication Technology (Citation2012) that more than 90% of the total number of blind people in Thailand have an education below the undergraduate level or no education at all for many reasons, such as the number of schools for the blind; only 13 schools are available in Thailand from the International Health Policy Program, Thailand (Citation2007), and very low income. Without education or with a low education level, the blind can barely read or understand Braille.
The National Statistical Office, Ministry of Information and Communication Technology (Citation2011) shows that senior citizens in Thailand increased to 7 million in 2011 and more than 60% of them have very low income, at approximately US$100 a month. It was found that there are more than 500,000 elderly living alone in Thailand. How can they safely self-medicate when they are sick? It is most likely that they will take the wrong, expired, or over dosed medication, and according to Thavornwattanayong, Anothayanon, Reungsakul, Sriphiromrak, and Chomjan (Citation2011), the elderly are at high risk for this. Braille labels are not a solution for the Thai visually impaired because most Thai blind and almost of the elderly cannot understand Braille. Therefore it is necessary to have a means to help them independently self-medicate. There are many commercial assistive technologies that respond to the need of impaired people for self-medication, such as TalkingRx (Citation2000), I.D. Mate (Citation2001) and ScripTalk (Citation2001). The TalkingRX system contains a 60-second digital recording device which is located on the bottom of a standard prescription bottle. It is not possible to use it for tablet-type medicine. The pharmacist needs to read the required medicine label to the TalkingRx device by pressing a record button and the user can then listen to the recording later at home by pressing another button on the device. TalkingRX is reusable and re-recordable; however, each prescription bottle requires its own unit, thereby requiring the user to buy as many TalkingRX units as they need. In addition, the cooperation of the pharmacist is required for using the TalkingRX which, in turn, causes the pharmacist to engage in time-consuming when the patient arrives at the store.
En-Vision America, Inc. is a company that aims to provide assistance technology for visually-impaired people. I.D. Mate (Citation2001) is a talking barcode scanner. It is a portable, electronic device which can scan barcodes and labels of various items at the grocery store, and the price is quite costly for low-income people. Additionally, the barcode location is not easy to locate for completely blind people. ScripTalk (Citation2001) is an audio medication-label system that applies RFID technology to identify prescriptions for visually-impaired people. The whole system of ScripTalk is well designed and is composed of a portable electronic reader and computer software. However, the cost for the reader is not affordable for Thai visually-impaired people. In addition, the pharmacy needs to invest large amounts of money in the system and it is not possible for pharmacies in Thailand to make this investment.
Assistive technology, developed by Lanigan, Paulos, Williams, Rossi, and Narasimhan (Citation2006), is the so-called “Trinetra” for helping the blind with their grocery shopping by using commercial off-the-shelf (COTS) components such as cell phones, the barcode reader “Baracoda Pencil,” and the RFID reader “IDBlue pen.” The Trinetra system requires many devices which are not convenient and are cumbersome in practical use. In addition, the cost of each device is not suitable for low-income people.
Recently, Magicavision is a company that aims to develop computer applications and electronic products to improve the everyday life of the visually impaired. MagicaCode (Citation2014) is an application that allows a smart phone to read the barcode of any product. Also, MagicaTag (Citation2014) is an application that makes any smart phone to be able to read a medicine label from the RFID tag attached to any product. Both applications can run on any Android or iOS phone. However, as mentioned above, most Thai visually-impaired people have a low income and thus a smart phone with the application is not affordable because the price of the cheapest smart phone is currently more expensive than US$150.
Boss (U.S. patent 7,408,465) has introduced an RFID system to help all visually-impaired people to be able to be independent in their daily life without canes or seeing-eye dogs. It is obvious that the system of Boss is not restricted to self-medication, and the RFID reader cannot be shared because it includes the profile of only one user. This makes the system of Boss unsuitable for helping Thai visually-impaired people to self-medicate.
It should be noted that assistive technologies or gadgets aimed particularly for visually-impaired people are very expensive because of the additional effort and cost to adapt and test the technologies with actual visually-impaired people.
The RFID systems in the works of Want, R. (Citation2006), Finkenzeller, K. (Citation2003) and Paret, D. (Citation2005) have long been used for merchandise identification, ID cards, boarding passes, ATM and credit cards, etc. Unlike the earlier bar-code technology, the RFID tags are reusable, they have the ability to hold more required information, and there are no requirements for line-of-sight reading of the tags, etc. There are two types of tags; namely, passive and active. The passive tag is applied to the label of items with battery-free remote access, composed of an antenna and an integrated circuit (IC). On the other hand, the active tag has a small battery to operate the tag’s return reporting signal. The active one is more costly but it has a long range. The passive RFID tag is well suited in this proposed APL system because it meets the requirement for developing a low-cost system.
Therefore, it is of interest to develop a low-cost APL system by using RFID for helping Thai visually-impaired people. This work focuses on two groups of visually-impaired people; namely, the blind and the elderly. When a visually-impaired person submits a prescription to a pharmacy, the pharmacist uses developed software to prepare and affix an RFID label containing important information, such as the patient’s name, drug name, dosage, general instructions, warnings, prescription number, the doctor’s name and telephone number, etc. The APL user can retrieve the information from the affixed RFID label using a portable, electronic reader unit (APL machine) with a voice synthesizer to read the label details aloud. In addition to the APL machine, computer software, the so-called APL software, was developed in this work for pharmacists to use when they need to prepare an RFID tag. In this research, we focus on the development of the APL system based on the needs of the end users, which are visually-impaired people. Thus it is very important that the APL machine is low cost, portable and comfortable to use. We also intend to develop APL software to be fool-proof for any pharmacist with only basic skills in using a computer. The APL system was evaluated by 5 experts and 70 actual end users. The evaluation was done using questionnaires or interviews to obtain all of the possible feedback from actual end users, which will then be used to develop the next generation of the APL system.
Conceptual Design of APL
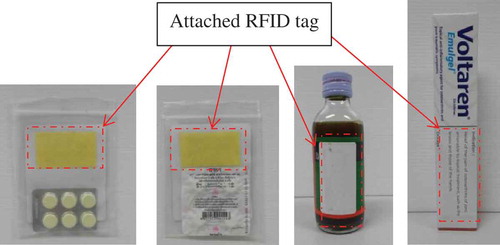
The developed APL system is composed of two parts: the APL machine and APL software. The APL machine is controlled by a microcontroller to read the RFID tag, which is attached to the corresponding medicine, as shown in . This RFID tag is needed to program the code via the developed APL software. The development of the APL software is intended to be license free and easy to use.
Fig. 1. RFID tags attached to medicine packages.
APL Machine
The block diagram of the developed APL machine is shown in . The APL machine is controlled by microcontroller ARM Cortex-M3 MB9BF506, which is simple to use and is of a reasonable price. By using the RFID reader, the APL machine can read a RFID tag attached to prescription label out loud. All of the voice files are kept in a micro SD card which is installed inside the machine and all files can be transferred via USB port by using the developed APL software. A vibrator is also included for a vibration alarm when turning on the APL machine.
Fig. 2. Block diagram of APL machine.
The marker area on the APL machine is intentionally designed for visually-impaired people to easily touch. When a visually-impaired person brings a prior-recorded RFID tag attached to a medicine package close to the marker area as shown in , the RFID reader, located inside the APL machine, can obtain the identification (ID) code. The RFID reader sends the ID code obtained from RFID tag to the microcontroller. Then the microcontroller compares the obtained ID code with the database in the microSD. Each ID code is indexed to a corresponding audio labelling file in the microSD. After the microcontroller can find the right audio labelling file, the MP3 decoder is used to produce the actual audio signal to be amplified and sent to speaker accordingly. If an ear phone is used, the speaker is disabled and vice versa. The vibrator is a motor which is used for a vibration alarm when the machine is turned on, and a LED is also used to display operation conditions when reading or programming the RFID tag.
Fig. 3. APL machine while reading medicine label.

The main of objective of the APL machine focuses on Thai visually-impaired people with a low income. The cost of the APL machine was of the most important concern. Small size and low power consumption were also taken into account in this work. The RFID tag should be able to be attached to the medicine package, and thus an RFID label type tag at the high frequency (HF) band of 13.56 MHz was considered the best fit. There are many transmission protocols for data communication. The Mifare (ISO14443A) and I-CODE (ISO15693) are the most popular ones. It is necessary to choose the RFID reader to be consistent with the RFID tag protocol. The small size RFID 13.56 MHz Read/Write Mifare module was chosen due to its low cost, small size, low voltage, and low power consumption. The family of ARM Cortex-M3 model MB9BF506N was chosen to be a microcontroller for the APL machine because it has a low price, is small, has a high speed, and a sufficient number of I/O ports. The microSD was the best candidate due to its price and size. The MP3 Decoder model VS1011E was selected because the price was less than US$9 and it can operate at low voltage. Three AAA batteries are used as the voltage supply for the APL machine because it is cheap, small and easy to buy. The list of key devices in the APL system with the design criteria is summarized in .
Table 1. List of key devices with concept selection.
The dimension of the developed APL machine is shown in . It can be seen that the size is not too large and it is easy to carry. The weight of the APL machine is only 200 g approximately. shows the prototype of the APL machine, whose cost is approximately US$100 or less. As listed in , almost 50% of the total cost comes from the RFID reader. It was found that mass production (more than 200 APLs to be made) would reduce the cost of each component. For example, the RFID Transponders HF reader IC would cost US$5.17, the microcontroller US$4.65, the MP3 decoder US$3.75, the SD card US$3, PCB and the packaging US$8 and other overhead US$5. The total cost would be dramatically reduced to less than US$30, which could be affordable for Thai visually-impaired people with a low income.
Fig. 4. Dimension of developed APL machine.
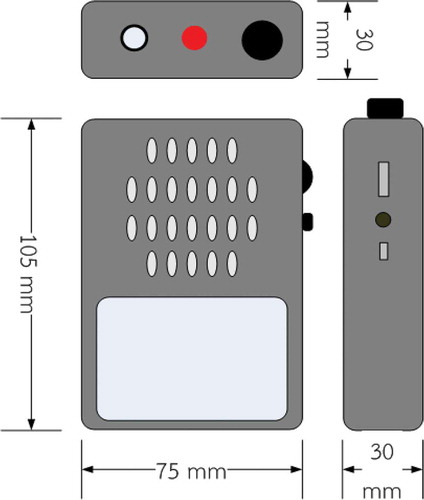
Fig. 5. Prototype of developed APL machine.

APL Software
The APL software was developed using Java, which can run on any Java Runtime Environment (JRE) regardless of the computer architecture. The Java is platform-independent and is open-source software. In addition, Java is object-oriented, which is easy to construct the Graphic User Interface (GUI) and it can work well with MySQL code, which is the most popular choice for an open-source database management system. Therefore, the APL software can include a database of all patients and prescriptions based on the MySQL code efficiently. When a visually-impaired person submits a prescription to a pharmacy, then the pharmacist uses the developed APL software to prepare and affix an RFID tag label containing important information, such as the medicine name and indication, dosage, expiration date, general instructions, and warnings. Users, patients that are visually-impaired people, can retrieve the information from the affixed RFID label using the APL machine via a voice synthesizer as described in the previous section.
The operation of the APL software is shown in Figure S1 and was developed by using the GUI with the main concept of being user friendly. There are two languages, Thai and English, in this software. The APL software is composed of 5 important windows as follows:
Add new patient window: used to record history and important information about the patient into the patient database.
Patient information window: used to view all recorded patient information.
Add new medicine window: used to add information about the medicine into the medicine database.
Medicine information window: used to view all recorded medicine information.
Record RFID tag window: used to record medicine information, ID code of RFID tag and the audio labelling file to the microSD in the APL machine.
From Figure S1, the database is composed of 3 parts as follows:
The patient database is used for adding new patient information into the database [Add new patient] as shown in Figure S2(a) and to read all of the patient data from the database [Patient data] as shown in Figure S2(b). The patient database consists of name, ID, medical treatment, drug allergies, and so on.
The medicine database is used for recording new medicine into the database [Add new medicine] as shown in Figure S3(a) and to read all of the medicine data from the database [Medicine data] as shown in Figure S3(b). The medicine database contains the medicine’s name, indication, dosage, expiration date, warning and so on. There are more than 100 medicines in the database of this work.
The RFID database is used for recording and reading the RFID tag [Save RFID tag] as shown in . The RFID database is composed of the patient’s name, the medicine’s name, and the RFID code. Also, the audio labelling file can be transferred to the APL machine via a USB port by using this window.
Fig. 6. Main window of APL software.

Evaluation Process
In order to verify the efficiency of this APL system, the evaluation was done by experts, Thai visually-impaired people, and APL software users.
Experience experts were selected from related professionals such as a director of a hospital, nurses, pharmacists, and programmers. The APL system, both machine and software, was evaluated by 5 experts, and the evaluation is done using a questionnaire with a score range from 5 to 1 corresponding to satisfaction level. The evaluation results are shown in . It was found that the element that was found to be most satisfactory, with an average score of 4.6, was the clarity of the audio of the APL machine, but the lowest, with an average score of 3.6, was the weight of the APL machine.
Table 2. Evaluation results of APL machine from experts.
Table 3. Evaluation results of APL software from experts.
Table 4. Number of respondents and their age range.
Table 5. Number of respondents and their gender.
Table 6. Number of medications of visually-impaired people.
Table 7. Evaluation results of APL machine from visually-impaired people.
Table 8. Opinion of visually-impaired people concerning easy to use overall.
Table 9. Opinion of visually-impaired people concerning convenience to carry.
Table 10. Opinions of visually-impaired people regarding the clarity of audio labeling from speaker.
The evaluation results for the APL software are shown in . It was found that the most satisfaction expressed by the experts, with an average score of 4.6, concerned the completeness of patient information, but the lowest degree of satisfaction, with an average score of 4.0, was with the speed of transferring files to the APL machine.
Visually-impaired people were purposively selected from actual Thai blind and elderly that had reading problems, with demographics as shown in –. The number of medications of the selected visually-impaired people is shown in . It was found that most of the selected visually-impaired people took medicine only when they needed to or when symptoms occurred. The evaluation via the interview was performed after using the APL machine. The evaluation results from the 20 blind people at the Skills Development Center for the Blind, Nonthaburi, Thailand and 30 elderly at the Bang Kruai Hospital, Nonthaburi, Thailand are shown in . It can be seen that 96% of the visually impaired samples agreed that the APL machine was easy to use. However, there was a conflict in the opinion between the blind and elderly regarding the issue of it being convenient to carry and the size of the APL machine. Most of the blind individuals wanted the APL machine to be of small size and light weight, but most of the elderly thought that the size and weight of the APL machine was suitable. This led to a low level of agreement, 64% and 72%, respectively.
Table 11. Opinions of visually-impaired people regarding appropriateness of using 3 AAA batteries.
Table 12. Evaluation results for APL software from users.
All of the blind individuals and 92.85% of the elderly agreed that the APL machine was easy to use, as shown in . According to , it was found that 60% of the blind did not agree that the APL was convenient to carry, while 80% of the elderly agreed. The opinions of these two sampled groups conflicted because the elderly felt comfortable when carrying the APL machine but the blind people felt that the APL machine was too big to carry. Eighty-five percent of the blind and elderly agreed that the audio labeling from the speaker of the APL machine was clear enough, according to . However, almost 20% of the sampled groups suggested that the audio labeling should be louder so that it can be used for people that are both blind and deaf or for the elderly that partially lack a sense of hearing. It was found, as can be seen in , that 50% of the blind and 73.33% of the elderly agreed that using 3 AAA batteries was appropriate for the APL machine. However, 36% of the visually impaired did not agree because they felt that it would not be convenient to replace the batteries.
The APL software users were selected from persons with demographics as shown in – that had experience in taking care of the blind or elderly, such as nurses, pharmacists, sighted persons, and so on. The evaluation via the questionnaire was carried out with 20 samples after using the APL software at the Wat Bang Phai Health Center, Nonthaburi, Thailand. The evaluation was done using a questionnaire with a score range from 5 to 1 corresponding to satisfaction level. shows the evaluation results. The highest score of satisfaction, with an average score of 4.4, was suitability of patient information. However, the lowest score, with an average score of 3.6, was suitability of information about the medicine because the medicine’s name in the APL software indicated symptoms but the users were familiar only with brand names or generic names, such as TENORETIC® (atenolol and chlorthalidone) for the treatment of hypertension or high blood pressure. Also, the satisfaction score for the suitability of the editing function was quite low at 3.7 because it was not convenient for users. They needed to enter all of the information again when they wanted to edit some information. This drawback has been fixed in the new version of the APL software.
Results and Discussion
The overall evaluation of both the APL machine and software was highly satisfactory. All of the assessors agreed that this research can help visually-impaired people to self-medicate and this developed system can improve the quality of life of visually-impaired people. The most satisfaction expressed by the visually-impaired people was that it was easy to use the machine. However, there were discrepancies regarding the weight and size of the APL machine between the blind and the elderly. The blind individuals would like to have a smaller and lighter APL machine but the elderly thought that the weight and size of developed machine was good enough. The elderly also commented on the AAA battery. They thought that it would be more convenient to use a battery pack instead of AAA batteries; thus a charging module would need to be included which would increase the cost of the machine. This is a tradeoff between price and comfort. Additionally, this APL machine has been tested for accuracy in reading prescription labeling more than 100 times and it was found that there were no errors in the reading. Some medicine packagings are made of foil to protect it from UV/visible light or moisture, and it is noted that the APL machine could not read the attached RFID tag close to the foil package of medicine because the performance of the antenna’s radiation used in the RFID tag is strongly influenced by the conductor, which is a foil package (Elliot, Citation2003). There are many techniques for handling this problem. For example, the work of Bjorninen, Sydanheimo, Ukkonen, and Rahmat-Samii (Citation2014) reviewed various types of antennas and design approaches used in metal-mountable RFID tags.
There were some useful comments from the assessors for improving this APL system as follows:
The price should be cheaper than this model.
The audio level should be louder.
The audio labeling should include more important information.
There should be a warning alarm in the APL machine before the time to take the medicine.
There should be a function to link the medicine database of the APL software with the medicine database of the hospital.
Conclusions
The overall objective of this work was to prevent deaths and injuries, while keeping the resulting device usable and cost effective. In addition, this work will prevent pharmacists from having to answer questions from patients that cannot read the print on the pill bottles, and keep patients from calling in the wrong prescriptions, which in turn causes the pharmacist to spend more time to prepare the medicine when the patient arrives at the store. This machine has been evaluated by actual visually-impaired people, nurses, pharmacists, sighed persons, doctors, and experts. The results of the evaluation from the experts revealed that the highest degree of satisfaction was the clarity of the audio from the APL machine, but the lowest degree of satisfaction was with the weight of the APL machine. For the APL software, the greatest amount of satisfaction from experts was with the completeness of the patient information and the lowest concerned the speed of transferring files to the APL machine. The evaluation from visually-impaired people showed that 96% of the visually-impaired individuals agreed that the APL machine was easy to use. Overall, the evaluation results were at a very high satisfaction level. The final stage of this work is to reproduce a prototype of the APL machine and to allow selected visually-impaired people to use it in their daily life at least for medicines for which prescriptions are not required such as those for headache, stomachache, heartburn, etc.
Supplemental Material
Supplemental data for this article can be accessed on the publisher’s website.
UATY_1004000_Supplemental_File.docx
Download MS Word (313.7 KB)References
- Bjorninen, T., Sydanheimo, L., Ukkonen, L., & Rahmat-Samii, Y. (2014). Advances in antenna designs for UHF RFID tags mountable on conductive items. IEEE Antennas and Propagation Magazine, 56, 79–103. doi:10.1109/MAP.2014.6821761
- Boss, G. J., Dawson, C. J., & Hamilton II, R. A. (2008). Method of Using RFID Systems to Help Blind and Visually-Impaired Individuals, United States Patent, US Patent No.7,408,465.
- Elliot, S. R. (2003). Antenna theory and design. Hoboken, NJ: John Wiley&Sons.
- Finkenzeller, K. (2003). RFID handbook. Chichester, UK: John Wiley&Sons.
- Foundation of Thai Gerontology Research and Development institute (TGRI) (2013). Annual report of situation of elderly in 2012. June 1, 2014, Retrieved from http://www.oppo.opp.go.th/info/Report_OlderSituation55-TH.pdf
- International Health Policy Program, Thailand (2007). Report on situation of disabilities in Thai Society 2002 and 2007. May 15, 2014, Retrieved from http://ihppthaigov.net/DB/publication/attachresearch/316/chapter1.pdf
- Lanigan, P. E., Paulos, A. M., Williams, A. W., Rossi, D., & Narasimhan, P. (2006, October). Trinetra: Assistive technologies for grocery shopping for the blind. Wearable Computers, 2006 10th IEEE International Symposium. Montreux, Switzerland, 147–148.
- MagicaCode (2014). Magicavision. May 15, 2014, Retrieved from http://www.magicavision.fr/magicacode
- MagicaTag (2014). Magicavision. May 15, 2014, Retrieved from http://www.magicavision.fr/magicatag
- Mate, I. D. (2001). En-Vision America, Inc. May 15, 2014, from http://www.envisionamerica.com/products/idmate/
- Ministry of Social Development and Human Security (2014). Thai disability in Thailand. May 30, 2014, Retrieved from http://www.m-society.go.th/article_attach/11434/15749.pdf
- National Statistical Office, Ministry of Information and Communication Technology (2012). Number of population and number of persons with disabilities aged 5-30 years not attending school, by reason for not attending school, sex and area, Whole Kingdom 2012. June 1, 2014, Retrieved from http://service.nso.go.th/nso/nso_center/project/search_center/23project-th.htm
- National Statistical Office, Ministry of Information and Communication Technology (2011). Report of number of elderly in Thailand of 2011. May 15, 2014, Retrieved from http://service.nso.go.th/nso/nso_center/project/search_center/23project-th.htm
- Paret, D. (2005). RFID and contactless smart card applications. Chichester, UK: John Wiley&Sons.
- ScripTalk (2001). En-Vision America, Inc. May 15, 2014, Retrieved from http://www.envisionamerica.com/products/scriptalk/
- TalkingRx (2000). Millennium Compliance Corporation. May 15, 2014, Retrieved from http://www.talkingrx.com/
- Thavornwattanayong, W., Anothayanon, J., Reungsakul, N., Sriphiromrak, P., & Chomjan, R. (2011). High-risk medication use in thai elderly patients: Case study in Wangtaku subdistrict, Nakorn Pathom. Journal of Health Systems Research, 5, 187–194.
- Want, R. (2006). An introduction to rfid technology. IEEE Pervasive Computing, 5, 25–33. doi:10.1109/MPRV.2006.2